
Hepatitis B Virus
Authors: Stevan A. Gonzalez, M.D., M.S.
VIROLOGY
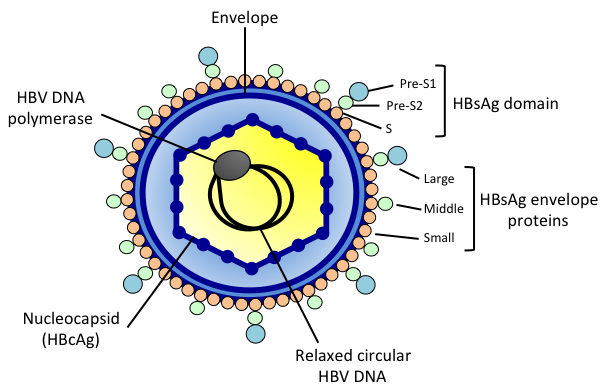
Hepatitis B virus (HBV) is an enveloped, partially double-stranded DNA virus of the Hepadnaviridae family (128). The infectious hepatitis B virion, known as the Dane particle, is approximately 42 nm in size and is composed of an outer lipid envelope containing viral glycoproteins as well as an inner nucleocapsid (Figure 1). The viral glycoproteins within the lipid envelope of the virion constitute the hepatitis B surface antigen (HBsAg). The nucleocapsid, composed of hepatitis B core antigen (HBcAg), encloses a copy of double-stranded circular HBV DNA and the HBV DNA polymerase.
{kind=link}
The HBV life cycle begins with binding of the hepatitis B virion to hepatocytes through interactions between cell surface receptors and viral envelope proteins, including the HBsAg (Figure 2) (128). Binding of the HBV envelope proteins and cellular receptors is followed by entry of the hepatitis B virion into the hepatocyte through endocytosis and the nucleocapsid is subsequently released into the cytoplasm. The nucleocapsid is uncoated at the nuclear membrane and relaxed circular HBV DNA (rcDNA) is released into the nucleus. Within the hepatocyte nucleus, rcDNA is converted into a covalently closed circular double-stranded DNA (cccDNA) molecule. The conversion of rcDNA to cccDNA involves a process of DNA repair and covalent ligation of both strands of circular DNA (144, 192). The intranuclear HBV cccDNA serves as a template for ongoing transcription of viral RNA.
{kind=link}
The double-stranded circular HBV DNA genome is approximately 3.2 kilobases (kb) in length and encodes four major RNA transcripts measuring 3.5 kb, 2.4 kb, 2.1 kb, and 0.7 kb. The largest (3.5 kb) transcript functions as both messenger RNA and as pre-genomic RNA. As transcription of the HBV cccDNA occurs within the hepatocyte nucleus, random integration of the HBV genome into the host chromosomes can also occur (16). Translation of viral RNA into the various HBV proteins involves four overlapping open reading frames (ORF): S (surface envelope), C (core), P (polymerase), and X (Figure 3). Both the S and C ORFs are characterized by in-frame initiation codons that facilitate the translation of different proteins within the RNA transcript (Figure 4). Thus, the C ORF encodes for the HBcAg and pre-core proteins, while the S ORF encodes for three different surface envelope proteins; large, middle, and small HBsAg. The pre-S domain of the large HBsAg protein appears to play a key role in binding of HBV to surface receptors on hepatocytes (110). The pre-core protein ultimately undergoes proteolysis and becomes hepatitis B e antigen (HBeAg) in the endoplasmic reticulum. The HBeAg may have an immunoregulatory role that facilitates chronic infection within the host and is an important marker of viral replication (164). The P ORF encodes the HBV polymerase, an enzyme that plays several roles in the replication process including facilitation of DNA synthesis, reverse transcription, and degradation of pre-genomic RNA. The X ORF encodes the X protein (HBxAg), which is thought to be involved in several functions such as cell cycle regulation, signal transduction, transcriptional activation, and DNA repair (12).
{kind=link}
{kind=link}
Assembly of the HBV nucleocapsid is initiated within the cytoplasm. Pre-genomic RNA enclosed within the nucleocapsid becomes a template for reverse transcription and synthesis of new HBV DNA. The conversion of pre-genomic RNA into viral rcDNA occurs via reverse transcription mediated by the HBV DNA polymerase. Further assembly of hepatitis B virions occurs at the endoplasmic reticulum. Mature virions are ultimately excreted through a process of budding and vesicular transport into the extracellular space. The HBV cccDNA molecule continues to exist as a viral minichromosome within the nucleus and is characterized by a high degree of stability, in which it can remain in the nucleus for the lifetime of the hepatocyte. Although levels of intrahepatic cccDNA can be suppressed with antiviral therapy, this form of HBV DNA appears to be resistant to eradication (48, 241).
![]()
EPIDEMIOLOGY
It is estimated that over 2 billion people have been exposed to HBV worldwide, while over 350 million people have chronic infection with HBV (2). The overall prevalence of chronic HBV infection appears to be declining in many parts of the world, likely due to increased immunization (178). The prevalence of chronic HBV varies widely based on geography. As a result, certain populations in regions of Africa, Asia, and the Pacific disproportionately comprise the largest proportion of individuals with chronic infection (59). Up to 45% of the world’s population resides in these endemic areas where the rate of HBsAg seropositivity is over 8%. In hyperendemic areas of Asia and sub-Saharan Africa, as much as 20% of the population may have chronic infection (2, 59). Other regions with high rates of HBsAg seropositivity include areas of South America, the Middle East, the Indian subcontinent, and Eastern Europe. In nonendemic regions such as North America and Western Europe, the distribution of chronic infection with HBV may reflect geographic immigration patterns of populations from endemic countries (108). Eight genotypes of HBV have been identified (A through H) as well as several subgenotypes(113). HBV genotypes are defined by greater than 8% genomic divergence in nucleotide sequence, while subgenotypes are defined by greater than 4% divergence. The global distribution of genotypes varies by geography, such that A, F, G, and H occur most frequently in western countries while genotypes B, C, and E are most commonly encountered in Asia and Africa. Genotype D is most prevalent in the Mediterranean region (113, 201).
Risk Factors for Exposure
HBV is primarily transmitted through parenteral routes, mucosal contact, or perinatal exposure. In regions characterized by a very high prevalence of HBV in the general population such as Asia and sub-Saharan Africa, infection is most commonly acquired through vertical or horizontal transmission early in life (2, 59). In developed countries, individuals at increased risk of exposure to HBV include injection drug users, persons with multiple sexual partners, incarcerated individuals, and dialysis patients (148, 168). Most cases of acute infection with HBV are asymptomatic. The development of chronic infection following acute exposure varies by age. Approximately 5% of adults acutely exposed to HBV progress to chronic infection, while as many as 90% of newborns exposed through vertical transmission may develop chronic HBV (92). Acute infection can result in a fulminant clinical course; however this is rare and occurs in less than 1% of acute HBV cases (2). Risk factors for developing acute liver failure (ALF) in the setting of HBV infection include increased age at the time of exposure, co-infection with hepatitis D virus (HDV), and co-infection with hepatitis C virus (HCV) (190, 229). Fulminant hepatitis B is associated with a high mortality of over 70% without liver transplantation (97, 176). The proportion of ALF cases in adults resulting from acute HBV infection in developed countries appears to be in decline. Early reports described HBV as the cause of ALF in up to 50% of cases; however, numbers of cases have decreased significantly over the last two decades (97, 126, 205). Recent data from one large prospective series from the United States from 1998 to 2007 reported HBV as the cause of ALF in 7% of cases (126). Individuals who are inactive HBsAg carriers are also at risk of fulminant hepatitis from either reactivation in the setting of immunosuppressive therapy or other causes, as their risk of ALF in the setting of an acute hepatitis increases 9-fold, regardless of etiology (53, 54, 207).
Hepatitis B and Hepatocellular Carcinoma
Chronic infection with HBV is a major cause of hepatocellular carcinoma (HCC), a leading cause of cancer-related death (180). The risk of HCC associated with HBV is significant and can exist in the absence of cirrhosis such that individuals with chronic infection have a 20-fold increase in risk of HCC (181). At this time, chronic HBV infection is the most common risk factor for HCC worldwide, accounting for up to 54% of cases (181). As a result, the distribution of HCC incidence throughout the world reflects the prevalence of HBV geographically (180). The incidence of HCC is highest in hyperendemic regions where the majority of individuals acquire HBV infection through vertical or horizontal transmission early in life (2, 36, 59). Early acquisition of HBV infection is a risk factor for HCC-related mortality and may contribute to the increased risk of HCC observed within families, particularly in endemic areas (36, 161, 260). First-degree relatives have over a 2-fold greater risk of HCC when one first-degree relative has HBV-associated HCC and a 5-fold greater risk when two first-degree relatives have HCC (260). A prolonged duration of infection characterized by persistence of serum HBsAg (46, 270) and HBeAg (162, 253) following early exposure to HBV is a major contributor to this increase in risk. In those who have chronic HBV infection, additional risk factors for HCC have been identified including development of cirrhosis, elevated serum alanine aminotransferase (ALT) levels, increased age, male gender, Asian or African ethnicity, alcohol or tobacco abuse, and exposure to aflatoxin. Individuals co-infected with HDV, HCV, or human immunodeficiency virus (HIV) are also at increased risk. In light of the risk of HCC in those chronically infected with HBV, surveillance in the form of hepatic imaging with or without measurement of the serum tumor marker alpha-fetoprotein (AFP) at 6 to 12 month intervals is recommended for those considered to be at increased risk (Table 1) (20, 71, 107, 177).
![]()
CLINICAL MANIFESTATIONS
Chronic liver disease associated with hepatitis B is a major cause of morbidity and mortality worldwide, accounting for over 500,000 deaths annually (82). Efforts to prevent and treat chronic HBV infection may have a major impact on the global incidence of progressive liver disease, cirrhosis, and HCC. Several factors have been associated with progression of liver disease once chronic infection with HBV is established. Early exposure to HBV is a major risk factor, as up to 25% of individuals who develop chronic infection early in life will develop cirrhosis or HCC (122). Additional risk factors for development of cirrhosis include elevated serum ALT levels, advanced age, and chronic heavy alcohol intake. Viral factors associated with disease progression include detectable serum HBeAg, increased serum HBV DNA levels, and infection with HBV genotype C (39, 56, 114, 142, 163).
Phases of Chronic Hepatitis B Infection
Once chronic infection is established within the host, the clinical course of HBV may fall into one of four phases: immune tolerance, immune clearance, inactive HBsAg carrier state, or reactivation (Table 2) (258). Immune tolerance is most frequently associated with younger individuals who likely acquired HBV infection perinatally through vertical or horizontal transmission. This phase is characterized by very high serum HBV DNA levels, detectable HBeAg, normal serum ALT levels, and minimal histologic activity on liver biopsy. In contrast, the immune clearance phase is associated with elevated ALT levels and significant HBV-associated disease on liver biopsy. In this phase, HBeAg is detectable and HBV DNA levels are typically elevated. The inactive HBsAg carrier state is notable for persistently detectable serum HBsAg, yet normal ALT levels, low or undetectable HBV DNA, and typically minimal disease on liver biopsy. This phase is also associated with seroconversion of HBeAg, defined by loss of HBeAg and emergence of antibody to HBeAg (anti-HBe). Some individuals may transition into a HBV reactivation phase also known as HBeAg-negative chronic HBV infection. This phase is characterized by negative HBeAg, positive anti-HBe, persistently or intermittently elevated ALT levels, and significant disease on liver biopsy. In the reactivation phase, HBV DNA may be elevated but typically not as elevated as observed in HBeAg-positive infection. Individuals who are in the immune clearance phase (HBeAg-positive) and the reactivation phase (HBeAg-negative) may be candidates for antiviral therapy. Several groups have developed guidelines for selection of appropriate candidates in whom therapy should be considered (Table 3). Treatment of HBV infection is not indicated in the setting of immune tolerance or the inactive HBsAg carrier state; however these individuals should be monitored longitudinally as they may transition into a more active phase of infection.
Influence of Genotype and Mutations
As a result of a high rate of viral replication of approximately 1011 virions per day and lack of a proofreading mechanism in the HBV polymerase, HBV replication is associated with a very high rate of spontaneous mutations (175). Within an infected host, HBV may exist in the form of multiple quasispecies in which viral strains will predominate as a consequence of endogenous and exogenous selection pressures, including replication fitness of specific viral mutants, host immunity, and antiviral therapy (50). Spontaneous mutations occur most frequently at the precore and core promoter regions (Figure 3). The frequencies of precore and core promoter mutations vary depending on HBV genotype. The most commonly encountered precore mutation (G1896A) is frequently associated with HBV genotype D infection and results in the formation of a stop codon within the precore region, leading to loss of production of the precore protein and HBeAg. In contrast, mutations occurring within the core promoter region are most commonly associated with genotype C infection, resulting in decreased production of HBeAg (50). Core promoter mutations have been associated with an increased risk of HCC and may in part account for the increased prevalence of HCC observed in genotype C infection (9, 28, 51, 106, 135, 138, 139, 221, 254, 267). Mutations within the pre-S region also appear to occur more frequently in the setting of genotype C infection and are similarly associated with an increased risk of HCC (35, 99, 136, 140, 210, 231). X promoter mutations and HBxAg have also been implicated in the development of HCC, although data are limited (12, 275). Mutations that arise during antiviral therapy may confer drug resistance leading to treatment failure. Strategies to minimize the potential for resistance are critical in maintaining optimal viral suppression and reducing the risk of disease progression as well as HCC.
Infection with specific HBV genotypes may have an impact on the clinical course of infection, development of advanced liver disease, and response to antiviral therapy. Genotype D has been reported with a higher prevalence in patients presenting with ALF associated with acute HBV infection (78, 229). Several studies in mostly Asian populations have reported an increased risk of HCC in patients infected with genotype C (28, 64, 105, 143, 248, 254, 262, 267) and possibly subgenotype Ce (29, 211). In Alaska natives, a population known to have a very high prevalence of chronic HBV infection, genotype C infection was associated with a delayed onset of spontaneous HBeAg seroclearance and increased vertical transmission rates (142). Factors such as prolongation of the interval to immune clearance and an increased incidence of reactivation may contribute to the increased risk of cirrhosis and HCC associated with this population (56, 114, 142). Genotype A has been associated with increased efficacy of interferon (IFN) alfa therapy with a higher potential of achieving clearance of HBeAg and HBsAg, while genotype C may be less IFN-responsive (204). Genotype A has also been associated with higher efficacy in the setting of oral nucleotide therapy based on rates of HBeAg clearance and seroconversion with tenofovir therapy (90).
Identifying Risk of Hepatocellular Carcinoma
In light of the increased risk among individuals with chronic HBV infection, elucidating viral factors that promote carcinogenesis and development of HCC are critical to identification of individuals who may be at particularly high risk, developing effective surveillance strategies, and selection of treatment candidates. Several prospective studies have established serum HBV DNA as a primary risk factor for HCC in patients with chronic HBV (29, 38, 39, 40, 254). The largest of these studies, the Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer-Hepatitis B Virus (REVEAL-HBV) study, prospectively investigated the association between serum HBV DNA levels and risk of HCC in a cohort of untreated HBsAg-positive patients in Taiwan(38).The study cohort included 3,653 mostly HBeAg-negative individuals who were followed over a mean of 11.4 years. The risk of HCC in this cohort increased in a linear relationship with serum HBV DNA levels, with the greatest risk observed at HBV DNA levels >104 copies/mL (Figure 4). The linear relationship between HBV DNA levels and risk of HCC occurred independently of cirrhosis, HBeAg positivity, or serum ALT levels. Although diminished, the risk of HCC also extends to individuals with low levels of HBV DNA, including inactive HBsAg carriers, who have an increased risk of HCC compared with HBsAg-negative controls (42). Other studies have noted that serologic markers of viral replication such as HBsAg(10, 37) and HBeAg (162, 253) are associated with an increased risk of HCC, in which the duration of antigenemia may contribute to this risk while spontaneous clearance of HBsAg may result in a reduction in risk (46, 270). The findings from the REVEAL-HBV study and others indicate that suppression of HBV with antiviral therapy plays a critical role in prevention of HCC. Prospective data involving patients with advanced liver disease have demonstrated significant reductions in the incidence of HCC with antiviral therapy (129). Additional analyses have also reported a lower incidence of HCC than predicted in patients receiving oral nucleoside or nucleotide analogue therapy vs. untreated patients over a long-term follow up, with reductions in HCC incidence by over 50% within a median of 4 years of therapy (58, 208).
Extrahepatic Manifestations of Hepatitis B
Extrahepatic manifestations of HBV infection includes various forms of vasculitis, renal disease, and arthritis, typically associated with circulating immune complexes within the host (88). Polyarteritis nodosa as well as glomerulonephritis, including membranoproliferative, membranous, and mesangial proliferative variants, appear to be associated with immune complex deposition and may improve with antiviral therapy, although data are limited. Essential mixed cryoglobulinemia can also occur in association with HBV infection, initially presenting with purpura, recurrent arthritis, and weakness, but can then progress to advanced disease characterized by features of vasculitis, glomerulonephritis, and pulmonary involvement. Additional extrahepatic manifestations of HBV may include palpable purpura and generalized arthralgias, which can appear at the time of acute infection or once chronic infection is established.
![]()
LABORATORY DIAGNOSIS
The diagnosis of HBV infection can be made with serological markers, while assessment of serum HBV DNA is instrumental in further differentiating between phases of chronic infection. Serological markers can also define prior infection with resolution or an individual who has undergone vaccination for HBV (Table 4). Serum HBsAg positivity or detection of serum HBV DNA defines the presence of HBV infection. In the setting of acute infection, both HBsAg and IgM antibodies to HBcAg may be positive; however assessment of HBV DNA is the most reliable test if ALF if present. Following the acute phase of infection, the host will develop IgG antibodies to HBcAg. In those who achieve spontaneous resolution with long-term immunity against HBV, antibodies directed against HBsAg (anti-HBs) will emerge coinciding with loss of HBsAg. In cases of chronic infection, HBsAg positivity will persist, defined by a positive serum HBsAg for greater than 6 months. Prior vaccination for HBV is characterized by the presence of anti-HBs, yet antibodies to HBcAg are absent.
PATHOGENESIS
In the setting of acute infection, development of a vigorous and multispecific cell-mediated response within the host directed towards HBV is critical in the achievement of spontaneous resolution. In contrast, a failure to develop an adequate adaptive immune response may result in persistence of viremia and subsequent development of chronic infection. Animal and human studies have demonstrated that HBV-specific CD8-positive cytotoxic T-cell immunity is essential in clearance of HBV-infected hepatocytes, while expression of pro-inflammatory cytokines such as IFN-γ play a major role in suppression of HBV replication. The host innate immune system may also contribute to achieving resolution of acute infection through activation of natural killer (NK), NKT cells, and Kupffer cells, resulting in further cytokine production and direct cytotoxicity mediated by these cell types.
The humoral immune response to HBV also plays a key role in establishing and maintaining immune control of acute infection as well as prevention of reactivation. The emergence of neutralizing antibodies directed towards HBcAg, HBeAg, and ultimately HBsAg indicate resolution of acute infection. These serologic markers also are important in monitoring long-term virologic response to therapy. Following recovery from acute infection, intranuclear HBV cccDNA can remain within hepatocytes. The persistence of host HBV-specific cell-mediated immunity as well as humoral immunity are essential to maintaining long-term immunologic control of HBV. Consequently, individuals with a history of recovery from HBV infection, particularly those who remain inactive HBsAg carriers, are at risk of HBV reactivation in the setting of immune suppression.
Acute Infection
Acute exposure to HBV is followed by an incubation phase characterized by a period of low viral replication and a subsequent progressive rise in viremia. Peak serum HBV DNA levels are reached at approximately 8 to 10 weeks following exposure, at which time up to 100% of hepatocytes can be infected with HBV (8, 84, 216, 237). The host innate immunity may have an important role during the earliest phases of acute infection in which NK cell activity may coincide with peak viremia following initial exposure to HBV (237). A subsequent vigorous polyclonal, multi-specific CD8+ T cell-mediated response directed towards HBV core, envelope, and polymerase epitopes is required in establishing immune control of HBV, leading to spontaneous resolution (72, 152, 194, 237). In particular, a clonal expansion of CD8+ T cells directed towards HBV core epitopes may be a key factor in achieving spontaneous clearance of HBV in the setting of acute infection (152, 237).
Chimpanzee studies have more precisely characterized the CD8+ T cell-mediated response during acute infection, which can be seen both in the liver and peripheral blood (216). Although a CD4+ T cell response can be observed during early phases of acute infection, a multispecific CD8+ cytotoxic response directed towards HBV envelope, core, and polymerase proteins appears to be critical in achieving viral clearance such that depletion of CD4+ T cells does not alter this response; however, depletion of CD8+ T cells will prolong HBV viremia until CD8+ subsets are restored (216). These events occur in concert with noncytolytic HBV suppression through increased intrahepatic expression of IFN-γ, TNF-α, and IFN-γ-induced genes (216, 243). This noncytolytic mechanism allows HBV to be cleared without destruction of infected hepatocytes and may be the primary means of eliminating virus in the acute setting (49, 83, 84, 166, 189), possibly through disruption of HBV nucleocapsid assembly(244, 245). The host innate immune system may also have a contributing role in achieving viral clearance through activation of NK, NKT cells, and Kupffer cells, leading to increased cytokine production, cytotoxicity, and recruitment of adaptive immunity (65, 73, 237, 257).
Chronic Infection
Individuals with chronic infection consistently demonstrate very weak or absent polyclonal and multispecific CD8+ responses to the HBeAg, polymerase, core, or surface antigens in peripheral blood compared with those who achieve spontaneous resolution (72, 167, 182, 194). However, some individuals with chronic infection maintain low level viremia and are found to have responsive peripheral and liver-infiltrating multispecific CD8+ T cells, more commonly directed towards HBV core epitopes (153, 238). In this setting, the observed CD8+ T cell reactivity appears to be narrowly focused and characterized by emergence of spontaneous mutations within epitopes that contribute to diminished T cell recognition of viral antigens, viral escape, and persistence of infection(13). A pattern of ongoing cellular activation and CD8+ T cell cytotoxicity may occur within the liver in those with chronic infection which is largely ineffective in achieving control of HBV, resulting in a persistent state of inflammation, hepatocyte injury, progressive hepatic fibrosis, cirrhosis, and increased risk of hepatocellular carcinoma (195).
Mechanisms of Persistence
In order to establish chronicity within the host and maintain persistence, HBV may have developed various mechanisms to effectively interfere with host immunity, diminish host recognition of the virus, and promote tolerance within the liver. In both human and chimpanzee studies, HBV appears to act as a stealth virus in which proinflammatory cytokine production is absent and NK cell activation is diminished following acute exposure, allowing early viral replication and immune tolerance (65, 86, 243). In particular, the HBeAg may have a central role in promoting immune tolerance during HBV infection through various immunoregulatory mechanisms including inhibition of antibody production, reduction of HBeAg- and HBcAg-specific T cell responses through clonal deletion or anergy, and inhibition of toll-like receptor (TLR) expression and signaling (44, 45, 47, 120, 145, 226). Other viral particles may also have inhibitory effects on host immunity including HBsAg effects on TLR-mediated immunity, HBV polymerase and X protein inhibition of interferon regulatory factor (IRF) signaling, and X protein disruption of proteasome activity and downregulation of the mitochondrial antiviral signaling (MAVS) protein (94, 117, 225, 230, 234, 239, 251, 263). Spontaneous mutations could also play a major role in viral persistence. Mutations within cytotoxic T cell epitopes could result in viral escape through disruption of major histocompatibility complex (MHC) binding or T cell receptor peptide recognition as demonstrated in studies revealing that mutations within the HBV core region were associated with impaired viral peptide recognition, cytotoxic activity, and IFN-γ secretory responses (14). Mutations occurring within the pre-core and core promoter regions can result in a loss or diminished expression of HBeAg. Longitudinal studies have suggested that pre-core mutations may occur under immunologic pressure at the time of HBeAg seroconversion, leading to disruption of HBeAg production (50). These events may coincide with core mutations within helper T cell epitopes, suggesting that this occurs as a result of immune pressure exerted by the host (27). Ultimately, the potential for spontaneous alterations of the core protein epitope occurring under selection pressure could be another means of viral escape and persistence through limiting host cytotoxic T cell recognition of HBV.
![]()
SUSCEPTIBILITY IN VITRO AND IN VIVO
The development of new investigational antiviral agents continues to advance with a greater understanding of the HBV life cycle and the potential to specifically target critical steps involved in HBV replication (Figure 2). Various members of the Hepadnaviridae family, including the woodchuck hepatitis virus, duck hepatitis virus, and woolly monkey hepatitis B virus, have been utilized extensively as a platform to conduct in vitro and in vivo studies to further develop new antiviral agents targeted against HBV. The majority of research associated with antiviral drug development has focused on nucleoside and nucleotide analogues, which target HBV DNA synthesis and effectively inhibit viral replication. The nucleoside analogues lamivudine, entecavir, telbivudine, and emtricitabine as well as the nucleotide analogues adefovir and tenofovir have all demonstrated antiviral potency against HBV both in vitro and in vivo, resulting in the availability of these agents as treatment options in the management of HBV infection in humans. In contrast with the nucleoside and nucleotide analogues, many investigational agents in development have thus far been limited to in vitro and animal studies. Key stages of the HBV life cycle identified as potential targets for new antiviral therapies include encapsidation, virion assembly, and various phases of HBV replication.
Inhibition of Viral Entry
The large HBsAg envelope protein has been identified as playing an important role in facilitating attachment of the hepatitis B virion to the surface of hepatocytes and is required for viral entry. The large envelope protein mediates attachment of virions to cell surface heparan sulfate proteoglycans. The sodium taurocholate cotransporting polypeptide (NTCP), a cell surface hepatocyte protein involved in transport of bile salts, functions as a receptor for HBV in which binding of NTCP to the N-terminal pre-S1 domain of the large envelope protein subsequently allows viral entry (252). Studies defining these events have led to the development of pre-S-derived lipopeptides, such as Myrcludex B, which are capable of blocking NTCP-mediated viral entry. Myrcludex B successfully inhibits the spread of HBV within the liver in a mouse model and has been well tolerated in human studies, in which HBV replication is suppressed in a dose-dependent fashion (17, 227).
Inhibition of Encapsidation
Encapsidation is a critical step in the HBV life cycle involving assembly of the HBV polymerase, pre-genomic RNA, and HBV core protein into the nucleocapsid. Following encapsidation, the pre-genomic RNA undergoes reverse transcription mediated by the HBV polymerase into new HBV DNA. Compounds known as heteroaryldihydropyrimidines (HAPs) bind to the HBV core protein, leading to dysfunctional polymer formation, degradation of core protein, and inhibition of proper nucleocapsid assembly (62, 209). The inhibitory effects of HAPs on HBV have been demonstrated in HepG2.2.15 cells and in a transgenic mouse model (62, 209, 236). Studies involving the HAP compounds BAY 41-4109 and GLS4 have reported effective inhibition of HBV replication with GLS4 demonstrating a higher potency in vitro and in a mouse model as well as a lower potential for toxicities (19, 236, 249). Peptide aptamers have also been reported to have an inhibitory effect on nucleocapsid formation through binding to the core protein (24, 220, 276). Direct inhibition of encapsidation may also occur with another class of compounds known as phenylpropenamides, as reported in studies utilizing various transfected hepatoma cell lines (61, 109, 184). The cellular inhibitor of apoptosis protein 2 (cIAP2) was found to have an inhibitory effect on HBV replication, primarily through targeting of the HBV polymerase leading to its degradation and inhibition of pre-genomic RNA encapsidation (235).The encapsidation inhibitor, NVR 3-778 has now emerged as a first-in-class agent that was well-tolerated in initial phase 1 trials and is now undergoing evaluation in patients with chronic HBV infection (77).
Hepatitis B Virion Assembly
Assembly of HBV virions requires interaction between core and envelope proteins in the endoplasmic reticulum. Alpha-glucosidase inhibitors disrupt this interaction through inhibiting the glycosylation of HBV envelope proteins, affecting the proper folding and subsequent transport of these proteins as well as infectivity of hepatitis B virions as described in HepG2.2.15 cell lines and animal models using woodchuck hepatitis virus (15, 123). Peptide aptamers have also been reported to inhibit virion assembly through binding to the HBV core protein as described in vitro (66).
Disruption of Hepatitis B Replication
Novel gene therapies have emerged with the ability to target HBV replication by promoting breakdown and degradation of HBV RNA within hepatocytes. Antisense oligodeoxyribonucleic acids (ODNs) bind to complementary viral RNA, inhibit translation or reverse transcription, and ultimately lead to RNA degradation. ODNs have demonstrated efficacy against HBV in vitro using HepG2.2.15 cell lines as well in animal models of duck hepatitis virus (112, 198). Short interfering RNAs (siRNAs) are short fragments of double-stranded RNA that can also inhibit mRNA transcription and lead to RNA breakdown. This occurs through a mechanism in which viral mRNA that is complementary to the siRNA is cleaved following introduction of siRNA into the cell. Inhibition of HBV replication through siRNAs has been demonstrated in HepG2.2.15 cells and in vivo through a mouse model (111, 161, 203). Novel nucleic acid polymers have emerged with activity targeted against the HBsAg, exerting an inhibitory effect on HBsAg release. An HBsAg release inhibitor, REP 9AC demonstrated efficacy in a duck hepatitis virus model and has now undergone evaluation in patients with chronic HBV infection, leading to clearance of HBsAg in a significant proportion (5, 173, 174). Additional HBsAg release inhibitors are now in development (265). Other targeted therapies against HBV include helioxanthin analogues, ribozymes, and immunomodulatory agents such as cytokines (Figure 2) (150, 259).
![]()
ANTIVIRAL THERAPY
Drugs of Choice
The primary goal of antiviral therapy in chronic HBV infection is the achievement of long-term virologic suppression for both HBeAg-positive and HBeAg-negative infection. Attaining this goal would provide the greatest potential to prevent disease progression, HCC, cirrhosis, and complications associated with end-stage liver disease (ESLD). At this time, five oral agents have been approved in the treatment of chronic HBV, including lamivudine, adefovir, entecavir, telbivudine, and tenofovir (Table 5). These oral agents are either nucleoside or nucleotide analogues, and are the most frequent form of therapy used for chronic HBV infection. As a class, the nucleoside and nucleotide analogues target the HBV polymerase and inhibit HBV DNA synthesis; although antiviral efficacy and the potential for drug resistance vary greatly among different agents. In light of their good tolerability, high potency, and high genetic barrier to resistance, entecavir and tenofovir are considered the preferred oral antiviral agents (3, 63, 107, 133, 148). An additional agent, IFN alfa, is administered in a subcutaneous form. In selected individuals, IFN alfa or the long-acting pegylated interferon (PegIFN) alfa may also be considered as a first-line agent.
Entecavir
Entecavir is a guanosine nucleoside analogue that inhibits HBV replication through several pathways including inhibition of base priming, HBV DNA polymerase reverse transcriptase activity, and HBV DNA synthesis. As a preferred agent, entecavir demonstrates a high potency in achieving viral suppression relative to other nucleoside or nucleotide analogues (Tables 6 and 7; Figure 6a and 6b). Entecavir is highly effective in suppressing HBV, as clearance of serum HBV DNA occurs in up to 67% and 90% of HBeAg-positive and HBeAg-negative patients, respectively, following one year of therapy (33, 118). In patients with HBeAg-positive infection, HBeAg seroconversion has been reported in over 20% of patients at one year (33). In addition, entecavir therapy is associated with achievement of HBsAg loss within one year of therapy. Although HBsAg loss occurs in a minority of patients, achievement of this parameter within one year has not been reported in other antiviral agents other than tenofovir and PegIFN alfa. Long term follow up of HBeAg-positive patients undergoing entecavir therapy has demonstrated a continued increase in the proportion of patients who achieve viral clearance, with up to 94% with undetectable serum HBV DNA after five years of therapy (34). Entecavir has a high genetic barrier to resistance. The cumulative probability of genotypic resistance has been reported to occur in only 1.2% of patients following 6 years of therapy in nucleoside-naïve patients (Figure 7) (212). However, the potential for resistance to entecavir is significant in previously treated patients with lamivudine resistance. The presence of the rtM204V/I mutation conferring resistance to lamivudine is associated with development of entecavir resistance in up to one-half of patients following 5 years of therapy (213). Based on this observation, entecavir monotherapy is not recommended in patients with known genotypic resistance to lamivudine (81, 107).
{kind=link}
{kind=link}
{kind=link}
Tenofovir
Tenofovir disproxil fumarate is a prodrug of tenofovir, an acyclic nucleotide analogue that inhibits the HBV polymerase and promotes premature HBV DNA chain termination. Similar to entecavir, tenofovir has demonstrated a high potency in achieving viral suppression relative to other oral antiviral agents for treatment of HBV infection. Tenofovir therapy is associated with achievement of undetectable serum HBV DNA in 76% of HBeAg-positive and 93% of HBeAg-negative patients, respectively, after one year (Tables 6 and 7; Figure 6a and 6b) (155). As reported with entecavir, HBsAg loss has been observed within one year of tenofovir therapy. Three year follow-up data revealed that patients treated with tenofovir maintain viral clearance and among HBeAg-positive individuals, the cumulative probability of HBsAg loss is 8% (89). Tenofovir has a very high genetic barrier to resistance in which no cases of resistance have been identified following up to eight years of therapy (Figure 7) (158). Due to potential toxicity associated with tenofovir disproxil fumarate in those with compromised renal function, monitoring of serum creatinine may be indicated in individuals at risk and dose reductions are recommended in those with an estimated creatinine clearance less than 50 mL/min. Tenofovir alafenamide is a new prodrug of tenofovir currently undergoing evaluation in clinical trials associated with a reduction in systemic exposures and a much lower potential for toxicity, particularly in the setting of renal insufficiency (4). Tenofovir is classified as pregnancy category B, in which animal studies have not demonstrated a risk to the developing fetus. Reviews of the Antiretroviral Pregnancy Registry database and several studies involving the use of tenofovir during pregnancy have reported an acceptable safety profile (232). Thus, tenofovir may be considered in the management of chronic HBV during pregnancy.
Interferon Alfa
Short-acting and long-acting forms of IFN alfa therapy are available as treatment for chronic HBV. Standard IFN alfa-2b, administered three times weekly, and PegIFN alfa-2a, administered once weekly, are currently approved in the treatment of chronic HBV in many countries. PegIFN alfa-2b has also demonstrated similar efficacy to PegIFN alfa-2a (101, 197). Treatment of HBV infection with IFN alfa may have several advantages over oral agents while demonstrating comparable antiviral efficacy. The duration of IFN alfa therapy is fixed for both HBeAg-positive and –negative infections. In addition, IFN alfa has no known association with drug resistance. However, both IFN and PegIFN alfa have been associated with many side effects that could limit tolerability. A fixed duration of 48 weeks therapy with PegIFN alfa results in viral clearance at end of treatment in up to 25% and 63% of HBeAg-positive and HBeAg-negative patients, respectively (Tables 6 and 7; Figure 6a and 6b) (101, 121, 154, 197). In HBeAg-positive infection, the rates of HBeAg loss and seroconversion at one year have been reported to be higher relative to oral nucleoside or nucleotide analogues (101, 121). In addition, the potential for HBsAg loss exists following one year of therapy for both HBeAg-positive and –negative infection (101, 121, 154). This is particularly notable in HBeAg-negative HBV, in which none of the oral agents have reported HBsAg loss within one year of therapy. Although data are limited, prolonged therapy with oral agents may result in similar rates of HBeAg seroconversion and HBsAg loss (34). The virologic response to PegIFN is durable. In one long-term follow up of patients with HBeAg-positive infection who were treated with PegIFN alfa-2b for 32 weeks, over 75% who initially achieved HBeAg seroconversion at end of treatment maintained anti-HBe positivity after 5 years (247). In addition, one-half of patients who did not demonstrate HBeAg seroconversion at the end of treatment eventually achieved this endpoint after 5 years of follow up. Caution should be used in patients with decompensated cirrhosis who receive IFN-based therapy due to risks of infection or a hepatitis flare; however, IFN is a safe option in those with well-compensated cirrhosis (22, 185).
Special Infections
Hepatitis D virus
Hepatitis D virus (HDV), also known as hepatitis Delta, is a defective virus limited to HBsAg carriers that requires the presence of HBsAg within the host for assembly of virions and infectivity. Co-infection of HDV and HBV occurs in up to 5% of all HBsAg carriers (68). The primary mode of HDV transmission is through parenteral routes and injection drug use remains a dominant source of new infections (68, 109). HDV infection is defined by the presence of the hepatitis D antigen (HDAg) and the diagnosis of chronic HDV can be made by assessment of serum HDAg and antibodies against HDAg (anti-HD). HDV infection may occur acutely with simultaneous HBV infection or in the form of superinfection with pre-existing chronic HBV, both of which can be associated with an increased risk of fulminant hepatitis. In comparison with HBV mono-infection, HBV-HDV co-infection is associated with a 2- to 3-fold greater risk of cirrhosis, HCC, clinical decompensation, and mortality (68, 70, 190). Successful treatment of chronic HDV requires clearance of HBsAg. As a result, nucleoside and nucleotide analogues are not effective and therapy is generally limited to standard IFN or long-acting PegIFN (26, 85, 172, 272). New therapies for HDV infection are emerging and currently in clinical trials, including the viral entry inhibitor Myrcludex B, which has activity against both HBV and HDV infections (17, 227).
![]()
Underlying Diseases
Hepatitis B and HIV Co-infection
Approximately 10% of individuals infected with HIV are co-infected with HBV (6). HIV and HBV have similar routes of transmission, a major factor accounting for the increased frequency of co-infection associated with these viruses. Additionally, prior infection with HIV is a risk factor for developing chronic HBV infection following acute exposure, as individuals with HIV have a six-fold increase in risk of chronicity associated with HBV (218). Low CD4+ T cell counts in HIV infection may contribute to the development of chronic infection, decreased clearance of HBeAg, increased HBV DNA levels, and a higher prevalence of cirrhosis. Data also suggest that the risk of HCC associated with HBV-HIV co-infection increases with lowering of CD4+ T cell counts (57). Consequently, HBV-HIV co-infection is associated with a higher liver-related mortality compared to those infected with HBV alone (217).
Management of HBV in the setting of HIV infection has become increasingly important in the era of highly active antiretroviral therapy (HAART), as liver disease associated with viral hepatitis has emerged as a major cause of morbidity and mortality while HIV infection has become more effectively controlled (102, 127). Due to the frequency of co-infection, all individuals with HIV should be screened for HBV infection. A first approach in the management of individuals with HBV-HIV co-infection is to achieve control of HIV. Some nucleoside and nucleotide analogues used to treat HBV such as tenofovir, emtricitabine, and lamivudine are active against HIV, thus HBV infection can be treated simultaneously. Patients treated with lamivudine should be monitored carefully as the potential for lamivudine resistance may be greater in co-infected patients than in those infected with HBV alone (11). Recent long-term data on tenofovir have noted a high proportion of co-infected patients achieving viral suppression within 5 years of therapy (60). Guidelines have recommended use of a liver biopsy to assess for evidence of histologic disease in co-infected individuals with elevated HBV DNA levels and normal ALT levels, as they are still at risk of chronic liver disease and may be candidates for antiviral therapy (107).
Hepatitis B and hepatitis C Co-infection
Chronic infections with HBV and HCV may exist simultaneously within a host and can occur commonly through shared exposure routes, including injection drug use and blood transfusions. Although definitive epidemiological data are limited, as many as 10% of anti-HCV positive individuals are positive for HBsAg, although some estimates are much lower (115). Likewise, it is estimated that up to 20% of HBsAg-positive individuals are positive for anti-HCV (52). Co-infection can occur through simultaneous acute exposure to HBV and HCV, superinfection of HCV on pre-existing chronic HBV, or superinfection with HBV on pre-existing HCV. In many cases one virus predominates with active replication, which is most commonly HCV. Patients with co-infection appear to be at greater risk of progressive fibrosis, advanced liver disease, HCC, and overall mortality (52, 115). Although no guidelines exist for the management of HBV-HCV co-infection, a consideration is initiation of therapy with combination PegIFN and ribavirin, as both HBV and HCV are responsive to an IFN-based regimen. However, the emergence of direct-acting antiviral therapy for HCV has led to major changes in treatment options, including the availability of highly effective, all oral, IFN-free regimens. Direct-acting antivirals such as sofosbuvir, a nucleotide analogue targeting the HCV RNA-dependent RNA polymerase, and ledipasvir, an HCV replication complex inhibitor, are now widely used in the treatment of chronic HCV infection. Although sofosbuvir has no significant interaction with coadminstered tenofovir, ledipasvir may increase tenofovir concentrations and could increase the potential for tenofovir-associated toxicity (1). Data assessing the role of HCV direct-acting antivirals or IFN in combination with a nucleoside or nucleotide analogue are limited, although this may be a consideration in patients with active HBV replication. Several prospective studies using IFN-based regimens have reported virologic response in both HBV and HCV (95, 137, 191, 224); however, patients should be monitored closely following completion of therapy as a significant proportion may experience a rebound in HBV DNA levels (191).
Recipients of Chemotherapy, Immunosuppression, or Organ Transplants
Individuals who are inactive HBsAg carriers and undergo cancer chemotherapy or immunosuppressive therapy are at risk of acute reactivation of hepatitis B, which can present as fulminant hepatitis. As HBV persists as highly stable cccDNA within hepatocyte nuclei, reactivation can occur in virtually all patients infected with HBV, even in patients who experience spontaneous resolution of infection or successful antiviral therapy. The risk of HBV reactivation varies within an individual based on their HBV serologic status, type of immunosuppressive therapy, and potential disruption of immunologic control. The greatest risk of reactivation has been associated with the presence of detectable serum HBV DNA, HBeAg positivity, HBsAg positivity, and the use of systemic cancer chemotherapy, B cell depleting agents such as rituximab, or high dose steroids (93, 187). Reactivation can occur in those who are HBsAg negative and has been described in association with biologic agents such as tumor necrosis factor (TNF) alpha inhibitors as well as in the setting of transarterial chemoembolization for hepatocellular carcinoma (100, 183).
The clinical presentation of HBV reactivation can vary widely, ranging from only mild elevations in serum aminotransferases to fulminant acute-on-chronic liver failure. Prophylactic antiviral therapy with an oral agent can reduce morbidity and mortality associated with reactivation and should be initiated prior to starting chemotherapy and extended beyond completion of the course for 6 to 12 months (Table 3) (151). In patients who present with acute-on-chronic liver failure as a result of acute reactivation of HBV infection, initiation of antiviral therapy may have an impact on survival, as suggested in a prospective randomized controlled trial in which patients with spontaneous reactivation who received tenofovir demonstrated a significant reduction in mortality compared with placebo (79). A meta-analysis evaluating the role of oral nucleoside or nucleotide analogue therapy in acute-on-chronic liver failure attributed to HBV infection similarly noted reductions in mortality in patients receiving either lamivudine or entecavir (264).
The risk of HBV reactivation extends to HBsAg carriers who undergo solid organ transplantation requiring long-term immunosuppressive therapy. Organ transplantation from anti-HBc-positive, HBsAg-negative donors is associated with a small, but significant risk of transmission of HBV infection to the recipient. The risk of transmission may vary by organ type, with the greatest risk reported in liver transplant recipients (228). HBV vaccination is recommended in all potential kidney transplant recipients. Post-transplant antiviral prophylaxis may be considered in recipients of anti-HBc-positive kidney transplants, although the need for this is uncertain (179). In contrast, antiviral prophylaxis is recommended for recipients of anti-HBc-positive liver transplants, particularly in recipients who are both anti-HBs and anti-HBc negative. In liver transplant recipients of anti-HBc-positive organs, post-transplant oral nucleoside or nucleotide therapy should be initiated; however the inclusion of HBIG in this regimen does not appear to have an impact on the risk of transmission (200).
![]()
Alternative Therapy
Lamivudine
The first oral antiviral agent approved as a treatment for chronic HBV infection, lamivudine, is an L-nucleoside analogue that inhibits HBV DNA synthesis by promoting premature DNA chain termination. Although lamivudine has demonstrated potency against HBV, the potential for resistance is high. Consequently, lamivudine is no longer considered a preferred first-line agent in the treatment of chronic HBV infection. Rates of resistance have been reported in over 70% of patients within four years of therapy (Figure 7) (146). Lamivudine resistance most frequently involves the rtM204V/I mutation, which occurs within the YMDD locus of the HBV polymerase (80). In patients who fail lamivudine therapy or develop resistance, the addition of adefovir or conversion to tenofovir monotherapy can be effective in achieving viral suppression (Table 8) (193, 223).
Adefovir
Adefovir is an acyclic nucleotide analogue, similar to tenofovir. Results from clinical trials have demonstrated adefovir to have modest potency against HBV; however it has a low genetic barrier to resistance, in which nearly 30% of HBeAg-negative patients develop drug resistance within five years of initiating therapy (87). As in tenofovir, adefovir toxicity can occur in the setting of renal dysfunction and dose reductions are required with decreases in estimated creatinine clearance to below 50 mL/min.
Telbivudine
Telbivudine is an L-nucleoside analogue, similar to lamivudine. Telbivudine has demonstrated relatively high antiviral potency, although it also has a low genetic barrier to resistance. Resistance to telbivudine has been reported to occur in up to 25% of patients at two years of therapy (119, 130) Telbivudine is classified as pregnancy category B and may be considered as an antiviral agent during pregnancy.
Emtricitabine
Emtricitabine is another L-nucleoside analogue with efficacy against HBV; however, it is not formally approved for the treatment of chronic HBV in most countries as either monotherapy or in combination with tenofovir. Emtricitabine appears to have substantial potency against HBV; however drug resistance is common, occurring in up to 13% within one year (134).
Combination Therapy
Combination therapy may have an important role in optimizing the potential for viral suppression in the setting of treatment failure or emergence of resistance (Table 8) (215). As increasingly potent oral antiviral agents with a high genetic barrier to resistance have become available, the potential need for combination therapy as a first-line approach may likely diminish. The results from a large prospective study evaluating the role of combination entecavir and tenofovir in HBeAg-positive and -negative treatment naïve patients revealed that entecavir alone was as effective as combination therapy (149). Although a tenofovir monotherapy arm was not included for comparison, this study demonstrated that monotherapy is sufficient in the setting of highly potent therapy. In data restricted to the HBeAg-positive subset, a modest increase in achievement of viral suppression at 96 weeks was seen in those who received combination therapy and had a high baseline HBV DNA level of >108 IU/mL, although the impact of this finding on long-term endpoints is uncertain. In contrast with treatment naïve patients, a combination of highly potent agents with a high genetic barrier to resistance, such as entecavir and tenofovir, is effective in suppressing HBV even in the presence of multidrug resistance (188). Although earlier studies involving combination lamivudine and PegIFN did not demonstrate improvements in virologic response in either HBeAg-positive or -negative patients (101,121, 154), a large randomized, controlled, open-label study reported higher rates of HBsAg loss associated with tenofovir plus PegIFN for 48 weeks compared with either tenofovir or PegIFN alone (157).
ADJUNCTIVE THERAPY
As a result of chronic HBV infection, approximately one in 3 to 4 individuals will progress to cirrhosis or HCC (55). In those who are potential candidates, liver transplantation may be considered as a treatment option with a significant benefit in long-term survival. Prior to the availability of hepatitis B immunoglobulin (HBIG) or nucleoside and nucleotide analogues, liver transplantation for HBV was associated with up to an 80% allograft re-infection rate and 50% 2-year survival (206). In contrast, current treatment strategies have improved survival rates to as high as 85% to 95% at 5 years (25). An important consideration in the management of potential transplant candidates is achievement of viral suppression prior to transplantation. Following liver transplantation, a combination of an oral antiviral agent and HBIG are given with the goal of preventing allograft re-infection, which is achieved in over 90% of patients using this regimen (206). Several strategies with an emphasis on minimizing HBIG have emerged, including HBIG dose reduction to improve cost efficacy and HBIG withdrawal; however further studies investigating the role of HBIG will be required to determine the most cost-effective option with the least potential for allograft re-infection, particularly in the context of potent oral antiviral therapy (76, 233).
![]()
ENDPOINTS FOR MONITORING THERAPY
Selection of Treatment Candidates
Clinical and laboratory parameters used in assessing treatment candidacy in patients with chronic HBV include serum HBV DNA levels, serum ALT, and liver histology. Several groups have published guidelines with recommendations for the selection of potential treatment candidates and when to initiate therapy (Table 3) (3, 107, 133, 148). Assessment of detectable HBV DNA in the presence of elevated ALT levels is a key factor in establishing treatment candidacy, particularly in light of emerging prospective data highlighting the association of elevated HBV DNA levels and risk of HCC and progressive chronic liver disease (29, 38, 39, 40, 98, 254, 266, 268). As the risk of disease progression has also been associated with low HBV DNA levels, particularly in those with HBeAg-negative infection, some guidelines recommend a lower threshold for initiation of therapy in this group (3, 107, 133). Treatment is not indicated in those classified as inactive HBsAg carriers or in the setting of immune tolerance; however these individuals should be monitored longitudinally. Initiation of antiviral therapy with oral nucleoside or nucleotide analogues may be considered in the setting of fulminant hepatitis B infection; however data evaluating this are limited (116, 219). One prospective study noted lamivudine therapy during severe acute HBV infection was associated with a more rapid decline in serum HBV DNA levels, although no clear benefit was noted in recovery from acute infection, serological markers, or biochemical parameters (116). In the setting of HBV reactivation with acute-on-chronic liver failure, oral nucleoside or nucleotide analogue therapy can be beneficial (79, 264).
Antiviral therapy should be considered in those with cirrhosis, as treatment can have an impact on the development of complications related to ESLD as well as risk of HCC. In one seminal multicenter, randomized, placebo-controlled trial of lamivudine therapy in patients with advanced fibrosis or cirrhosis found that patients randomized to receive lamivudine had a lower incidence of HCC and slower progression of liver disease within 3 years of follow up (129). Therefore, antiviral therapy with nucleoside or nucleotide analogues is recommended for all patients with decompensated cirrhosis and detectable serum HBV DNA. Additional studies involving treatment with other oral agents such as entecavir and tenofovir have reported antiviral efficacy, histologic improvement, and overall safety in this population, including those with hepatic decompensation (131, 132, 202). Long-term data have now demonstrated significant histologic benefit in patients undergoing tenofovir therapy, including regression of fibrosis and cirrhosis(156). In the setting of compensated cirrhosis, a low threshold for initiation of therapy based on HBV DNA levels has been proposed by most groups (Table 3). The use of IFN alfa therapy is not recommended in patients with decompensated cirrhosis due to a significant risk of acute exacerbation of liver disease, characterized by high serum ALT levels further clinical decompensation, and risk of infection (91, 148, 185).
Antiviral therapy can be considered during pregnancy to prevent vertical transmission; however, administration of the HBV vaccine and HBIG to the newborn to achieve active immunization immediately after birth can avoid transmission of HBV. In early studies of combination vaccine and HBIG vs. placebo or no intervention, vertical transmission was avoided in over 95% of cases (124). If treatment is considered, tenofovir and telbivudine are both classified as pregnancy category B. Pregnant women who are positive for HBsAg can potentially experience a flare of hepatic disease before or after delivery and should be followed closely (169, 214).
Monitoring Virologic Response and Management of Resistance
Monitoring serum HBV DNA levels during nucleoside or nucleotide analogue therapy is an important consideration in achieving optimal virologic response and minimizing the potential for developing antiviral drug resistance(107). During a course of therapy, the emergence of mutations conferring drug resistance can lead to persistent viremia with an increase in risk of progressive liver disease and HCC (7, 146). The incidence of resistance varies among the nucleoside and nucleotide analogues (Figure 7) (87, 119, 130, 134, 146, 158, 213) and is influenced by an agent’s respective genetic barrier to resistance, defined by the probability of mutations occurring in response to the selective pressure exerted by the agent(107). Additional factors associated with the development of drug resistance include the presence of persistent viral replication despite therapy, the frequency of mutations, and the replication fitness of new mutations (144). A treatment algorithm with on-treatment monitoring has been proposed with the goal of identifying individuals at risk of treatment failure or an inadequate virologic response associated with oral therapy. Primary treatment failure, defined by the inability to reduce HBV DNA by 1 log10 IU/mL from baseline, can be assessed at 12 weeks of therapy. HBV DNA levels at 24 weeks can be used to determine whether an individual has experienced a partial or inadequate virologic response, defined by levels of 60-2,000 IU/mL and >2,000 IU/mL, respectively (107). HBV DNA levels should be measured every 3 to 6 months thereafter for ongoing surveillance during therapy, with close follow up in partial responders to ensure continued viral suppression. An increase of ≥1 log10 IU/mL above the nadir HBV DNA level is considered virologic breakthrough and may indicate the development of resistance (147). In the setting of primary treatment failure, an inadequate virologic response, or established antiviral resistance, the addition or conversion to an oral agent of another class with a higher potency should be considered (Table 8). This strategy will promote further viral suppression while avoiding potential cross-resistance, which is more likely to occur among antiviral agents within the same class (80, 107, 148, 193). Adherence to therapy should be assessed in all patients who demonstrate an inadequate response.
Predictors of Response
Various host factors, viral factors, and on-treatment parameters have been identified as predictors of treatment response in the setting of oral antiviral therapy. Baseline characteristics such as elevated ALT levels (≥2x the upper limit of normal [ULN]) and low serum HBV DNA (< 9 log10 copies/mL) have been associated with viral clearance and HBeAg seroconversion in HBeAg-positive patients treated with telbivudine, while low body mass index (BMI) (< 22.5) is associated with viral clearance in both HBeAg-positive and HBeAg-negative infection (273). After initiation of therapy, achievement of complete viral suppression at an early time point assessed through measurement of serum HBV DNA or quantitative HBsAg is also predictive of a successful response. Achievement of complete viral suppression within 24 weeks is predictive of HBV DNA clearance, decreased incidence of drug resistance, and increased HBeAg seroconversion (87, 269, 273). In addition, a rapid decline in quantitative HBsAg levels is predictive of eventual HBsAG loss (250, 277).
Several baseline and on-treatment predictors have also been identified in association with a successful response to PegIFN therapy. In patients with HBeAg-positive infection, elevated ALT levels, low HBV DNA, and low quantitative HBeAg levels prior to initiation of therapy may be predictive of eventual HBeAg seroconversion (75, 186). Likewise, in patients with HBeAg-negative infection, elevated ALT, low HBV DNA, younger age, and female gender are predictive of viral suppression after completion of therapy (18). HBV genotype may also have an impact on virologic response to PegIFN, as genotypes A or B appear to be associated with a more favorable outcome, particularly in HBeAg-positive infection (23, 67, 74, 101, 121). During therapy, a significant decline in quantitative HBsAg levels indicated by a decline of 0.5 log10 IU/mL at 12 weeks, 1.0 log10 IU/mL at 24 weeks, or > 1.1 log10 IU/mL throughout the course of therapy have been reported to be predictive of achieving sustained viral suppression in HBeAg-negative patients (21, 165). Ultimately, identifying baseline factors associated with a favorable virologic response may be more important in the selection of candidates for PegIFN therapy as tolerability is a concern in some patients.
Long-Term Endpoints of Therapy
In contrast with IFN-based therapy, in which the duration of therapy is well defined, assessing the endpoint of antiviral therapy with oral nucleoside or nucleotide analogues can be challenging. Serologic markers are instrumental in monitoring long-term virologic response to oral therapy, particularly in HBeAg-positive infection. HBeAg seroconversion, characterized by HBeAg loss and emergence of anti-HBe, can be used as an endpoint of therapy indicating a successful response. Following HBeAg seroconversion, discontinuation of therapy can be considered at 6 months after the appearance of anti-HBe (148), although a more conservative and common recommendation involves considering discontinuation after 12 months of both HBeAg seroconversion and HBV DNA negativity (3, 107, 133). In contrast, oral antiviral therapy is frequently required over the long-term for those with HBeAg-negative infection. In both HBeAg-positive and –negative infection, discontinuation of treatment may be considered following HBsAg, although this is a rare occurrence (148). As complete eradication of HBV is not easily attainable due to persistence of intranuclear HBV cccDNA within the host, all patients in whom treatment is discontinued require long-term follow up as the risk of HBV reactivation can persist long after successful therapy.
![]()
VACCINES
Hepatitis B infection is preventable with vaccination. The HBV vaccine may be administered as recombinant or plasma-derived HBsAg and is effective in preventing chronic HBV infection in over 95% of cases. Vaccination can provide long-term immunity for over 20 years based on data from longitudinal cohort studies (171). Two single-antigen vaccines are currently approved for HBV as well as one vaccine in combination with hepatitis A virus (Table 9) (160). Overall, these vaccines are well tolerated in both children and in adults. In many countries in which a comprehensive immunization strategy has been initiated, the HBV vaccine is recommended in all routine infant vaccinations as well as unvaccinated individuals who are at risk of potential exposure to HBV including health care workers, travelers to HBV-endemic areas, household contacts of persons with chronic HBV infection, and organ transplant recipients (Table 10) (2). An additional group in whom vaccination is recommended includes patients with other underlying chronic liver diseases, as they may be at risk of a more fulminant course in the setting of superimposed acute HBV infection (160, 196). An adjunctive therapy to the HBV vaccine utilized during post-exposure prophylaxis or to prevent vertical transmission is HBIG, which can be given to individuals following a suspected exposure to HBV or to at-risk newborns immediately following delivery from HBsAg-positive mothers. Contraindications to receiving the vaccines include a history of previous severe allergic reaction or hypersensitivity to the vaccine or vaccine components. All HBV vaccines require a multiple dosing schedule, which is needed to ensure optimal immune protection against the virus. In immunocompromised individuals, assessment of quantitative anti-HBsAg may be required to ensure adequate dosing.
PREVENTION OR INFECTION CONTROL MEASURES
Decreasing the risk of transmission of HBV through immunization may be the most effective method of preventing HBV-associated disease including chronic hepatitis, cirrhosis, and HCC, particularly in high-risk populations (2). With the development of the HBV vaccine and its widespread use since 1982, HCC is regarded as the first major cancer that is preventable by the implementation of immunization programs. Through successful immunization strategies, the HBV vaccine is capable of preventing new HBV infections, subsequent chronic liver disease, and most cases of HCC on a global scale. Consequently the HBV vaccine may be considered as a primary prevention of liver cancer (2). In 1991, the World Health Organization (WHO) called for universal infant HBV immunizations, and by 2008, 177 countries had added the HBV vaccine to their immunization programs (2). However, the vaccine is not available in some endemic regions, particularly sub-Saharan Africa and the Indian subcontinent. In many countries where chronic HBV infection rates in children were as high as 8% to 15%, the rates of chronic infection have now been reduced to less than 1% through immunization programs (104). In the US, the incidence of new infections with HBV has declined by over 80% since implementation of a large-scale immunization program in 1991 according to data from the National Notifiable Diseases Surveillance System of the Centers for Disease Control and Prevention (CDC) (199). Likewise, large cohort studies involving young age groups in Taiwan have documented a significant decrease in the seroprevalence of HBsAg and decrease in the HBV carrier rate indicated by HBV core antibody seropositivity since the implementation of widespread immunization (41, 170). Recent estimates have noted a significant decline in overall HBV prevalence in many areas of the world, particularly in younger age groups, which appears be attributed to immunization programs (178).
A significant reduction in the incidence of HCC in some populations can be directly attributed to the HBV vaccine. One large study in Taiwan based on data from the Taiwan National Cancer Registry over a 13-year period found a significant decrease in HCC incidence and mortality in the years following the implementation of a national HBV immunization program in 1984 (30, 170, 171). In another large cohort study from Korea, a trend towards a reduced relative risk of HCC was seen in vaccinated patients compared with unvaccinated patients after only 4 years of follow up (125). Additional studies in Taiwan revealed that HCC incidence following implementation of the immunization program may be associated with vaccine failure or lack of hepatitis B immunoglobulin being given to infants with HBsAg-positive mothers (32).
Although these studies demonstrate the potential benefit of HBV vaccination in the prevention of HCC, some endemic areas are still at risk due to insufficient resources to support an immunization program (31). As the incidence of HCC increases with age, it is likely that the full positive impact of HBV immunization on the development of HCC will be seen in the years to come and in future generations.
![]()
CONTROVERSIES, CAVEATS, OR COMMENTS
Individualized Surveillance for Hepatocellular Carcinoma
Identifying individuals with chronic HBV who are at increased risk of HCC is an important consideration in the development of an optimal HCC surveillance strategy. Early detection of HCC through surveillance has a major impact on long-term outcomes, including survival (20, 274). Although several organizations have provided guidelines for targeting specific HBV-infected patient groups who would benefit most from surveillance as a result of their increased risk of HCC, these guidelines are based primarily on clinical and demographic risk factors (Table 1), while well-established virologic risk factors such as HBV DNA level are not included (20, 71, 107, 177). In light of these concerns, several predictive scoring systems have been published with the intent of enabling the clinician to estimate an individualized risk of HCC in a person with chronic HBV based on clinical, demographic, as well as virologic parameters (246, 255, 256, 271). An individualized predictive score could then potentially guide strategies for HCC surveillance.
Predictive HCC risk scores based on two large single-center cohort studies from Hong Kong identified the presence of cirrhosis, core promoter mutations, male gender, and elevated serum HBV DNA levels as independent risk factors for HCC in individuals with chronic HBV (246, 271). Other predictive scoring systems, including the use of nomograms as well as a risk score, have been developed from prospective data associated with the REVEAL-HBV cohort from Taiwan (255, 256). The predictive nomograms include different risk variables, such that a different nomogram could be used depending on virologic data available to the clinician (256). A major limitation of the REACH-B systems is that the study cohort did not include patients with cirrhosis.
Although these studies have provided further evidence highlighting the importance of virologic parameters in assessment of HCC risk in patients with chronic HBV, validation of these scoring systems will be required to ensure that these findings are applicable to larger populations. Adoption of an individualized surveillance strategy could be cost effective as those considered low-risk may not require surveillance; however, a concern would be the potential exclusion of individuals who would benefit from surveillance. In contrast, those at higher risk may require earlier onset of surveillance with possibly more frequent follow up. Ultimately further studies will be required to elucidate factors that contribute to HCC risk and how an individualized assessment could guide optimal treatment and surveillance strategies in this population.
New Biomarkers for Detection of Hepatocellular Carcinoma
The most widely used tumor marker for HCC, alpha-fetoprotein (AFP), is limited in its ability to discriminate between individuals at high or low risk of HCC. As a result, alpha-fetoprotein has been excluded in some guidelines on HCC surveillance. Serum alpha-fetoprotein is characterized by a low sensitivity, in which over 45% of patients with HCC may have normal serum alpha-fetoprotein levels (69). Several alternative serum markers for HCC have been identified including a fucosylated isoform of alpha-fetoprotein reactive to Lens culinaris agglutinin, known as AFP-L3, and prothrombin induced by vitamin K absence II (PIVKA II), also known as des-γ-carboxyprothrombin (DCP). AFP-L3 has an increased sensitivity and specificity compared with alpha-fetoprotein; however, it can only be used in patients with elevated baseline AFP levels (222). DCP is limited by low sensitivity, although its performance characteristics vary based on liver disease etiology and its sensitivity appears to be increased in chronic viral hepatitis, including HBV infection(159). Several additional markers have been identified as potential screening tools in the early detection of HCC including glypican-3 (GPC-3), osteopontin, golgi protein 73 (GP73), microRNA (miRNA), α-1-fucosidase, human telomerase reverse transcriptase, squamous cell carcinoma antigen, and transforming growth factor-β1. Efforts are ongoing to discover other potential biomarkers for HCC surveillance through genome-wide association studies, proteomic and metabolomic analysis, and glycomics. These techniques have identified novel genomic profiles, serum protein fragments, and alterations in N-glycosylation with differential expression in cases of HCC (43, 103, 41). Ultimately an individualized approach based on clinical risk factors and a combination of genomic profiling with other biomarkers may provide the most accurate screening tool for discriminating individuals at increased risk of HCC.
Recognition of Hepatitis B Reactivation
Early recognition of individuals at risk of HBV reactivation in the setting of immunosuppression or cancer chemotherapy is critical to successful prevention and management of cases. Despite guidelines now in place recommending screening and pre-emptive antiviral therapy to prevent HBV reactivation (3, 133, 148, 240), reported screening rates among health care providers remains low. These findings have emerged while the utilization of immunosuppressive medications in the form of biologic agents and disease-modifying antirheumatic drugs (DMARDs) has increased, particularly in the treatment of various inflammatory disorders involving a diverse range of medical specialties including gastroenterology, dermatology, and rheumatology. Apart from cancer chemotherapy and conventional immunosuppression, DMARDs include azathioprine, methotrexate, cyclosporine, and biologic agents such as tumor necrosis factor (TNF) alpha inhibitors. Recent data have revealed that a very low proportion of health care providers who prescribe chemotherapy or immunosuppression routinely screen for underlying HBV infection. Two large retrospective reviews of screening practices in US cancer centers involving over 8,000 and 10,000 patients undergoing cancer chemotherapy, respectively, found only 16% to 17% of patients underwent screening to assess for the presence of serum HBsAg or anti-HBc (96, 242). In one study, even when known risk factors for HBV infection were identified, less than 20% were screened (96).
In another study, almost 40% of patients who were screened and found to have HBV infection ultimately did not receive antiviral prophylaxis, leading to cases of reactivation (242).These findings highlight the need for increased awareness among healthcare providers involved in managing patients at risk of HBV reactivation, particularly in light of reactivation as a preventable event associated with a high potential for morbidity and mortality.
![]()
REFERENCES
1. Harvoni® (ledipasvir/sofosbuvir) [Full Prescribing Information]. Revised October, 2014. Gilead Sciences, Inc. Foster City, CA, USA.
2. World Health Organization. Hepatitis B Vaccines: WHO Position Paper. Weekly Epidemiological Record 2009;84:405-420.
3. EASL clinical practice guidelines: Management of chronic hepatitis B virus infection. J Hepatol 2012;57:167-85. [PubMed]
4. Agarwal K, Fung SK, Nguyen TT, Cheng W, Sicard E, Ryder SD, Flaherty JF, Lawson E, Zhao S, Mani Subramanian G, McHutchison JG, Gane EJ, Foster GR. Twenty-eight day safety, antiviral activity, and pharmacokinetics of tenofovir alafenamide for treatment of chronic hepatitis B infection. J Hepatol 2014;pii: S0168-8278. [PubMed]
5. Al-Mahtab M, Bazinet M, Vaillant A. REP 9AC is a potent HBsAg release inhibitor which clears serum HBsAg and elicits SVRs in patients with chronic hepatitis B [abstract]. J Hepatol 2011;54 (Suppl):S34.
6. Alter MJ. Epidemiology of viral hepatitis and HIV co-infection. J Hepatol 2006;44:S6-9. [PubMed]
7. Andreone P, Gramenzi A, Cursaro C, Biselli M, Camma C, Trevisani F, Bernardi M. High risk of hepatocellular carcinoma in anti-HBe positive liver cirrhosis patients developing lamivudine resistance. J Viral Hepat 2004;11:439-42. [PubMed]
8. Asabe S, Wieland SF, Chattopadhyay PK, Roederer M, Engle RE, Purcell RH, Chisari FV. The size of the viral inoculum contributes to the outcome of hepatitis B virus infection. J Virol 2009;83:9652-62. [PubMed]
9. Baptista M, Kramvis A, Kew MC. High prevalence of 1762(T) 1764(A) mutations in the basic core promoter of hepatitis B virus isolated from black Africans with hepatocellular carcinoma compared with asymptomatic carriers. Hepatology 1999;29:946-53. [PubMed]
10. Beasley RP, Hwang LY, Lin CC, and Chien CS. Hepatocellular carcinoma and hepatitis B virus. A prospective study of 22 707 men in Taiwan. Lancet 1981;2:1129-33. [PubMed]
11. Benhamou Y, Bochet M, Thibault V, Di Martino V, Caumes E, Bricaire F, Opolon P, Katlama C, and Poynard T. Long-term incidence of hepatitis B virus resistance to lamivudine in human immunodeficiency virus-infected patients. Hepatology 1999;30:1302-6. [PubMed]
12. Benhenda S, Cougot D, Buendia MA, and Neuveut C. Hepatitis B virus X protein molecular functions and its role in virus life cycle and pathogenesis. Adv Cancer Res 2009;103:75-109. [PubMed]
13. Bertoletti A, Costanzo A, Chisari FV, Levrero M, Artini M, Sette A, Penna A, Giuberti T, Fiaccadori F, Ferrari C. Cytotoxic T lymphocyte response to a wild type hepatitis B virus epitope in patients chronically infected by variant viruses carrying substitutions within the epitope. J Exp Med 1994;180:933-43. [PubMed]
14. Bertoletti A, Sette A, Chisari FV, Penna A, Levrero M, De Carli M, Fiaccadori F, Ferrari C. Natural variants of cytotoxic epitopes are T-cell receptor antagonists for antiviral cytotoxic T cells. Nature 1994;369:407-10. [PubMed]
15. Block TM, Lu X, Mehta AS, Blumberg BS, Tennant B, Ebling M, Korba B, Lansky DM, Jacob GS, Dwek RA. Treatment of chronic hepadnavirus infection in a woodchuck animal model with an inhibitor of protein folding and trafficking. Nat Med 1998;4:610-4. [PubMed]
16. Block TM, Mehta AS, Fimmel CJ, Jordan R. Molecular viral oncology of hepatocellular carcinoma. Oncogene 2003;22:5093-107. [PubMed]
17. Bogomolov P, Voronkova N, Allweiss L, Dandri M, Schwab M, Lempp FA, Haag M, Wedemeyer H, Alexandrov A, Urban S. A proof-of-concept phase 2a clinical trial with HBV/HDV entry inhibitor Myrcludex B [abstract]. Hepatology 2014;60 (Suppl 1):LB-20.
18. Bonino F, Marcellin P, Lau GK, Hadziyannis S, Jin R, Piratvisuth T, Germanidis G, Yurdaydin C, Diago M, Gurel S, Lai MY, Brunetto MR, Farci P, Popescu M, McCloud P. Predicting response to peginterferon alpha-2a, lamivudine and the two combined for HBeAg-negative chronic hepatitis B. Gut 2007;56:699-705. [PubMed]
19. Brezillon N, Brunelle MN, Massinet H, Giang E, Lamant C, DaSilva L, Berissi S, Belghiti J, Hannoun L, Puerstinger G, Wimmer E, Neyts J, Hantz O, Soussan P, Morosan S, Kremsdorf D. Antiviral activity of Bay 41-4109 on hepatitis B virus in humanized Alb-uPA/SCID mice. PLoS One 2011;6:e25096. [PubMed]
20. Bruix J and Sherman M. Management of Hepatocellular Carcinoma: An Update. Hepatology 2010;000:1-35. Accessed online at http://publish.aasld.org/practiceguidelines/Documents/Bookmarked Practice Guidelines/HCCUpdate2010.pdf.
21. Brunetto MR, Moriconi F, Bonino F, Lau GK, Farci P, Yurdaydin C, Piratvisuth T, Luo K, Wang Y, Hadziyannis S, Wolf E, McCloud P, Batrla R, and Marcellin P. Hepatitis B virus surface antigen levels: a guide to sustained response to peginterferon alfa-2a in HBeAg-negative chronic hepatitis B. Hepatology 2009;49:1141-50. [PubMed]
22. Buster EH, Hansen BE, Buti M, Delwaide J, Niederau C, Michielsen PP, Flisiak R, Zondervan PE, Schalm SW, Janssen HL, Group HBVS. Peginterferon alpha-2b is safe and effective in HBeAg-positive chronic hepatitis B patients with advanced fibrosis. Hepatology 2007;46:388-94. [PubMed]
23. Buster EH, Flink HJ, Cakaloglu Y, Simon K, Trojan J, Tabak F, So TM, Feinman SV, Mach T, Akarca US, Schutten M, Tielemans W, van Vuuren AJ, Hansen BE, and Janssen HL. Sustained HBeAg and HBsAg loss after long-term follow-up of HBeAg-positive patients treated with peginterferon alpha-2b. Gastroenterology 2008;135:459-67. [PubMed]
24. Butz K, Denk C, Fitscher B, Crnkovic-Mertens I, Ullmann A, Schroder CH, and Hoppe-Seyler F. Peptide aptamers targeting the hepatitis B virus core protein: a new class of molecules with antiviral activity. Oncogene 2001;20:6579-86. [PubMed]
25. Bzowej N, Han S, Degertekin B, Keeffe EB, Emre S, Brown R, Reddy R, and Lok AS. Liver transplantation outcomes among Caucasians, Asian Americans, and African Americans with hepatitis B. Liver Transpl 2009;15:1010-20. [PubMed]
26. Canbakan B, Senturk H, Tabak F, Akdogan M, Tahan V, Mert A, Sut N, Ozaras R, Midilli K, and Ozbay G. Efficacy of interferon alpha-2b and lamivudine combination treatment in comparison to interferon alpha-2b alone in chronic delta hepatitis: a randomized trial. J Gastroenterol Hepatol 2006;21:657-63. [PubMed]
27. Carman WF, Boner W, Fattovich G, Colman K, Dornan ES, Thursz M, Hadziyannis S. Hepatitis B virus core protein mutations are concentrated in B cell epitopes in progressive disease and in T helper cell epitopes during clinical remission. J Infect Dis 1997;175:1093-100. [PubMed]
28. Chan HL, Hui AY, Wong ML, Tse AM, Hung LC, Wong VW, Sung JJ. Genotype C hepatitis B virus infection is associated with an increased risk of hepatocellular carcinoma. Gut 2004;53:1494-8. [PubMed]
29. Chan HL, Tse CH, Mo F, Koh J, Wong VW, Wong GL, Lam Chan S, Yeo W, Sung JJ, Mok TS. High viral load and hepatitis B virus subgenotype ce are associated with increased risk of hepatocellular carcinoma. J Clin Oncol 2008;26:177-82. [PubMed]
30. Chang MH, Chen CJ, Lai MS, Hsu HM, Wu TC, Kong MS, Liang DC, Shau WY, Chen DS. Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. Taiwan Childhood Hepatoma Study Group. N Engl J Med 1997;336:1855-9. [PubMed]
31. Chang MH. Decreasing incidence of hepatocellular carcinoma among children following universal hepatitis B immunization. Liver Int 2003;23:309-14. [PubMed]
32. Chang MH, Chen TH, Hsu HM, Wu TC, Kong MS, Liang DC, Ni YH, Chen CJ, Chen DS. Prevention of hepatocellular carcinoma by universal vaccination against hepatitis B virus: the effect and problems. Clin Cancer Res 2005;11:7953-7. [PubMed]
33. Chang TT, Gish RG, de Man R, Gadano A, Sollano J, Chao YC, Lok AS, Han KH, Goodman Z, Zhu J, Cross A, DeHertogh D, Wilber R, Colonno R, Apelian D. A comparison of entecavir and lamivudine for HBeAg-positive chronic hepatitis B. N Engl J Med 2006;354:1001-10. [PubMed]
34. Chang TT, Lai CL, Kew Yoon S, Lee SS, Coelho HS, Carrilho FJ, Poordad F, Halota W, Horsmans Y, Tsai N, Zhang H, Tenney DJ, Tamez R, Iloeje U. Entecavir treatment for up to 5 years in patients with hepatitis B e antigen-positive chronic hepatitis B. Hepatology 2010;51:422-30. [PubMed]
35. Chen BF, Liu CJ, Jow GM, Chen PJ, Kao JH, Chen DS. High prevalence and mapping of pre-S deletion in hepatitis B virus carriers with progressive liver diseases. Gastroenterology 2006;130:1153-68. [PubMed]
36. Chen CH, Chen YY, Chen GH, Yang SS, Tang HS, Lin HH, Lin DY, Lo SK, Du JM, Chang TT, Chen SC, Liao LY, Kuo CH, Lin KC, Tai DI, Changchien CS, Chang WY, Sheu JC, Chen DS, Liaw YF, Sung JL. Hepatitis B virus transmission and hepatocarcinogenesis: a 9 year retrospective cohort of 13676 relatives with hepatocellular carcinoma. J Hepatol 2004;40:653-9. [PubMed]
37. Chen CJ, Yu MW, Liaw YF. Epidemiological characteristics and risk factors of hepatocellular carcinoma. J Gastroenterol Hepatol 1997;12:S294-308. [PubMed]
38. Chen CJ, Yang HI, Su J, Jen CL, You SL, Lu SN, Huang GT, Iloeje UH. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. Jama 2006;295:65-73. [PubMed]
- 39. Chen CJ, Yang HI, Iloeje UH. Hepatitis B virus DNA levels and outcomes in chronic hepatitis B. Hepatology 2009;49:S72-84. [PubMed]
40. Chen G, Lin W, Shen F, Iloeje UH, London WT, Evans AA. Past HBV viral load as predictor of mortality and morbidity from HCC and chronic liver disease in a prospective study. Am J Gastroenterol 2006;101:1797-803. [PubMed]
41. Chen HL, Chang MH, Ni YH, Hsu HY, Lee PI, Lee CY, Chen DS. Seroepidemiology of hepatitis B virus infection in children: Ten years of mass vaccination in Taiwan. JAMA1996;276:906-8. [PubMed]
42. Chen JD, Yang HI, Iloeje UH, You SL, Lu SN, Wang LY, Su J, Sun CA, Liaw YF, Chen CJ. Carriers of inactive hepatitis B virus are still at risk for hepatocellular carcinoma and liver-related death. Gastroenterology 2010;138:1747-54. [PubMed]
43. Chen K, Shi W, Xin Z, Wang H, Zhu X, Wu X, Li Z, Li H, Liu Y. Replication of genome wide association studies on hepatocellular carcinoma susceptibility loci in a Chinese population. PLoS One 2013;8:e77315. [PubMed]
44. Chen M, Sallberg M, Hughes J, Jones J, Guidotti LG, Chisari FV, Billaud JN, Milich DR. Immune tolerance split between hepatitis B virus precore and core proteins. J Virol 2005;79:3016-27. [PubMed]
45. Chen MT, Billaud JN, Sallberg M, Guidotti LG, Chisari FV, Jones J, Hughes J, Milich DR. A function of the hepatitis B virus precore protein is to regulate the immune response to the core antigen. Proc Natl Acad Sci USA 2004;101:14913-8. [PubMed]
46. Chen YC, Sheen IS, Chu CM, Liaw YF. Prognosis following spontaneous HBsAg seroclearance in chronic hepatitis B patients with or without concurrent infection. Gastroenterology 2002;123:1084-9. [PubMed]
47. Chen Z, Cheng Y, Xu Y, Liao J, Zhang X, Hu Y, Zhang Q, Wang J, Zhang Z, Shen F, Yuan Z. Expression profiles and function of Toll-like receptors 2 and 4 in peripheral blood mononuclear cells of chronic hepatitis B patients. Clin Immunol 2008;128:400-8. [PubMed]
48. Cheng PN, Liu WC, Tsai HW, Wu IC, Chang TT, Young KC. Association of intrahepatic cccDNA reduction with the improvement of liver histology in chronic hepatitis B patients receiving oral antiviral agents. J Med Virol 2011;83:602-7. [PubMed]
49. Chisari FV, Isogawa M, Wieland SF. Pathogenesis of hepatitis B virus infection. Pathol Biol (Paris) 2010;58:258-66. [PubMed]
50. Chotiyaputta W, Lok AS. Hepatitis B virus variants. Nat Rev Gastroenterol Hepatol 2009;6:453-62. [PubMed]

51. Chou YC, Yu MW, Wu CF, Yang SY, Lin CL, Liu CJ, Shih WL, Chen PJ, Liaw YF, Chen CJ. Temporal relationship between hepatitis B virus enhancer II/basal core promoter sequence variation and risk of hepatocellular carcinoma. Gut 2008;57:91-7. [PubMed]
52. Chu CJ, Lee SD. Hepatitis B virus/hepatitis C virus coinfection: epidemiology, clinical features, viral interactions and treatment. J Gastroenterol Hepatol 2008;23:512-20. [PubMed]
53. Chu CJ, Liaw YF. The incidence of fulminant hepatic failure in acute viral hepatitis in Taiwan: increased risk in patients with pre-existing HBsAg carrier state. Infection 1990;18:200-3. [PubMed]
54. Chu CM, Liaw YF. Increased incidence of fulminant hepatic failure in previously unrecognized HBsAg carriers with acute hepatitis independent of etiology. Infection 2005;33:136-9. [PubMed]
55. Chu CM, Liaw YF. Hepatitis B virus-related cirrhosis: natural history and treatment. Semin Liver Dis 2006;26:142-52. [PubMed]
56. Chu CM, Liaw YF. Predictive factors for reactivation of hepatitis B following hepatitis B e antigen seroconversion in chronic hepatitis B. Gastroenterology 2007;133:1458-65. [PubMed]
57. Clifford GM, Rickenbach M, Polesel J, Dal Maso L, Steffen I, Ledergerber B, Rauch A, Probst-Hensch NM, Bouchardy C, Levi F, Franceschi S. Influence of HIV-related immunodeficiency on the risk of hepatocellular carcinoma. AIDS 2008;22:2135-41. [PubMed]
58. Coffin CS, Rezaeeaval M, Pang JX, Alcantara L, Klein P, Burak KW, Myers RP. The incidence of hepatocellular carcinoma is reduced in patients with chronic hepatitis B on long-term nucleos(t)ide analogue therapy. Aliment Pharmacol Ther 2014;40:1262-9. [PubMed]
59. Custer B, Sullivan SD, Hazlet TK, Iloeje U, Veenstra DL, Kowdley KV. Global epidemiology of hepatitis B virus. J Clin Gastroenterol 2004;38:S158-68. [PubMed]
60. de Vries-Sluijs TE, Reijnders JG, Hansen BE, Zaaijer HL, Prins JM, Pas SD, Schutten M, Hoepelman AI, Richter C, Mulder JW, de Man RA, Janssen HL, van der Ende ME. Long-term therapy with tenofovir is effective for patients co-infected with human immunodeficiency virus and hepatitis B virus. Gastroenterology 2010;139:1934-41. [PubMed]
61. Delaney W 4th, Edwards R, Colledge D, Shaw T, Furman P, Painter G, Locarnini S. Phenylpropenamide derivatives AT-61 and AT-130 inhibit replication of wild-type and lamivudine-resistant strains of hepatitis B virus in vitro. Antimicrob Agents Chemother 2002;46:3057-60. [PubMed]
62. Deres K, Schroder CH, Paessens A, Goldmann S, Hacker HJ, Weber O, Kramer T, Niewohner U, Pleiss U, Stoltefuss J, Graef E, Koletzki D, Masantschek RN, Reimann A, Jaeger R, Gross R, Beckermann B, Schlemmer KH, Haebich D, Rubsamen-Waigmann H. Inhibition of hepatitis B virus replication by drug-induced depletion of nucleocapsids. Science 2003;299:893-6. [PubMed]
63. Dienstag JL. Hepatitis B virus infection. N Engl J Med 2008;359:1486-500. [PubMed]
64. Ding X, Mizokami M, Yao G, Xu B, Orito E, Ueda R, and Nakanishi M. Hepatitis B virus genotype distribution among chronic hepatitis B virus carriers in Shanghai, China. Intervirology 2001;44:43-7. [PubMed]
65. Dunn C, Peppa D, Khanna P, Nebbia G, Jones M, Brendish N, Lascar RM, Brown D, Gilson RJ, Tedder RJ, Dusheiko GM, Jacobs M, Klenerman P, Maini MK. Temporal analysis of early immune responses in patients with acute hepatitis B virus infection. Gastroenterology 2009;137:1289-300. [PubMed]
66. Dyson MR, Murray K. Selection of peptide inhibitors of interactions involved in complex protein assemblies: association of the core and surface antigens of hepatitis B virus. Proc Natl Acad Sci U S A 1995;92:2194-8. [PubMed]
67. Erhardt A, Ludwig AD, Brunetto MR, van Boemmel F, Wolf E, Goebel T, Siemer M, Adams O, Huassinger D. HBV genotypes are the strongest predictors of response to interferon-alfa treatment: Multivariate evaluation in 1229 hepatitis B patients [abstract]. Hepatology 2008;48:700A-701A.
68. Farci P. Delta hepatitis: an update. J Hepatol 2003;39 Suppl 1:S212-9. [PubMed]
69. Farinati F, Marino D, De Giorgio M, Baldan A, Cantarini M, Cursaro C, Rapaccini G, Del Poggio P, Di Nolfo MA, Benvegnu L, Zoli M, Borzio F, Bernardi M, Trevisani F. Diagnostic and prognostic role of alpha-fetoprotein in hepatocellular carcinoma: both or neither? Am J Gastroenterol 2006;101:524-32. [PubMed]
70. Fattovich G, Giustina G, Christensen E, Pantalena M, Zagni I, Realdi G, Schalm SW. Influence of hepatitis delta virus infection on morbidity and mortality in compensated cirrhosis type B. The European Concerted Action on Viral Hepatitis (Eurohep). Gut 2000;46:420-6. [PubMed]
71. Ferenci P, Fried M, Labrecque D, Bruix J, Sherman M, Omata M, Heathcote J, Piratsivuth T, Kew M, Otegbayo JA, Zheng SS, Sarin S, Hamid SS, Modawi SB, Fleig W, Fedail S, Thomson A, Khan A, Malfertheiner P, Lau G, Carillo FJ, Krabshuis J, Le Mair A. Hepatocellular carcinoma (HCC): a global perspective. J Clin Gastroenterol 2010;44:239-45. [PubMed]
72. Ferrari C, Penna A, Bertoletti A, Valli A, Antoni AD, Giuberti T, Cavalli A, Petit MA, Fiaccadori F. Cellular immune response to hepatitis B virus-encoded antigens in acute and chronic hepatitis B virus infection. J Immunol 1990;145:3442-9. [PubMed]
73. Fisicaro P, Valdatta C, Boni C, Massari M, Mori C, Zerbini A, Orlandini A, Sacchelli L, Missale G, Ferrari C. Early kinetics of innate and adaptive immune responses during hepatitis B virus infection. Gut 2009;58:974-82. [PubMed]
74. Flink HJ, van Zonneveld M, Hansen BE, de Man RA, Schalm SW, Janssen HL. Treatment with Peg-interferon alpha-2b for HBeAg-positive chronic hepatitis B: HBsAg loss is associated with HBV genotype. Am J Gastroenterol 2006;101:297-303. [PubMed]
75. Fried MW, Piratvisuth T, Lau GK, Marcellin P, Chow WC, Cooksley G, Luo KX, Paik SW, Liaw YF, Button P, Popescu M. HBeAg and hepatitis B virus DNA as outcome predictors during therapy with peginterferon alfa-2a for HBeAg-positive chronic hepatitis B. Hepatology 2008;47:428-34. [PubMed]
76. Gane E. Posttransplant prophylaxis strategies for hepatitis B. Am J Transplant 2010;10:1721-2. [PubMed]
77. Gane EJ, Schwabe C, Walker K, Flores L, Hartman GD, Klumpp K, Liaw S, Brown NA. Phase 1a safety and pharmacokinetics of NVR 3-778, a potential first-in-class HBV core inhibitor [abstract]. Hepatology 2014;60 (Suppl 1):LB19.
78. Garfein RS, Bower WA, Loney CM, Hutin YJ, Xia GL, Jawanda J, Groom AV, Nainan OV, Murphy JS, Bell BP. Factors associated with fulminant liver failure during an outbreak among injection drug users with acute hepatitis B. Hepatology 2004;40:865-73. [PubMed]
79. Garg H, Sarin SK, Kumar M, Garg V, Sharma BC, Kumar A. Tenofovir improves the outcome in patients with spontaneous reactivation of hepatitis B presenting as acute-on-chronic liver failure. Hepatology 2011;53:774-80. [PubMed]
80. Ghany M, Liang TJ. Drug targets and molecular mechanisms of drug resistance in chronic hepatitis B. Gastroenterology 2007;132:1574-85. [PubMed]
81. Ghany MG, Doo EC. Antiviral resistance and hepatitis B therapy. Hepatology 2009;49:S174-84. [PubMed]
82. Goldstein ST, Zhou F, Hadler SC, Bell BP, Mast EE, Margolis HS. A mathematical model to estimate global hepatitis B disease burden and vaccination impact. Int J Epidemiol 2005;34:1329-39. [PubMed]
83. Guidotti LG, Ishikawa T, Hobbs MV, Matzke B, Schreiber R, Chisari FV. Intracellular inactivation of the hepatitis B virus by cytotoxic T lymphocytes. Immunity 1996;4:25-36. [PubMed]
84. Guidotti LG, Rochford R, Chung J, Shapiro M, Purcell R, Chisari FV. Viral clearance without destruction of infected cells during acute HBV infection. Science 1999;284:825-9. [PubMed]
85. Gunsar F, Akarca US, Ersoz G, Kobak AC, Karasu Z, Yuce G, Ilter T, Batur Y. Two-year interferon therapy with or without ribavirin in chronic delta hepatitis. Antivir Ther 2005;10:721-6. [PubMed]
86. Guy CS, Mulrooney-Cousins PM, Churchill ND, Michalak TI. Intrahepatic expression of genes affiliated with innate and adaptive immune responses immediately after invasion and during acute infection with woodchuck hepadnavirus. J Virol 2008;82:8579-91. [PubMed]
87. Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, Chang TT, Kitis G, Rizzetto M, Marcellin P, Lim SG, Goodman Z, Ma J, Brosgart CL, Borroto-Esoda K, Arterburn S, Chuck SL. Long-term therapy with adefovir dipivoxil for HBeAg-negative chronic hepatitis B for up to 5 years. Gastroenterology 2006;131:1743-51. [PubMed]
88. Han SH. Extrahepatic manifestations of chronic hepatitis B. Clin Liver Dis 2004;8:403-18. [PubMed]
89. Heathcote EJ, Marcellin P, Buti M, Gane E, De Man RA, Krastev Z, Germanidis G, Lee SS, Flisiak R, Kaita K, Manns M, Kotzev I, Tchernev K, Buggisch P, Weilert F, Kurdas OO, Shiffman ML, Trinh H, Gurel S, Snow-Lampart A, Borroto-Esoda K, Mondou E, Anderson J, Sorbel J, Rousseau F. Three-year efficacy and safety of tenofovir disoproxil fumarate treatment for chronic hepatitis B. Gastroenterology 2011;140:132-43. [PubMed]
90. Heathcote J, Manns M, Mathurin P, Ebrahimi R, Anderson J, and Lou L. Baseline genotype and HBsAg were found to have significant association with HBeAg seroconversion following up to 4 years of tenofovir disoproxil fumarate treatment [abstract]. J Hepatol 2011;54:S287.
91. Hoofnagle JH, Di Bisceglie AM, Waggoner JG, Park Y. Interferon alfa for patients with clinically apparent cirrhosis due to chronic hepatitis B. Gastroenterology 1993;104:1116-21. [PubMed]
92. Hoofnagle JH, Doo E, Liang TJ, Fleischer R, Lok AS. Management of hepatitis B: summary of a clinical research workshop. Hepatology 2007;45:1056-75. [PubMed]
93. Hsu C, Tsou HH, Lin SJ, Wang MC, Yao M, Hwang WL, Kao WY, Chiu CF, Lin SF, Lin J, Chang CS, Tien HF, Liu TW, Chen PJ, Cheng AL, Taiwan Cooperative Oncology G. Chemotherapy-induced hepatitis B reactivation in lymphoma patients with resolved HBV infection: a prospective study. Hepatology 2014;59:2092-100. [PubMed]
94. Hu Z, Zhang Z, Doo E, Coux O, Goldberg AL, Liang TJ. Hepatitis B virus X protein is both a substrate and a potential inhibitor of the proteasome complex. J Virol 1999;73:7231-40. [PubMed]
95. Hung CH, Lee CM, Lu SN, Wang JH, Tung HD, Chen CH, Changchien CS. Combination therapy with interferon-alpha and ribavirin in patients with dual hepatitis B and hepatitis C virus infection. J Gastroenterol Hepatol 2005;20:727-32. [PubMed]
96. Hwang JP, Fisch MJ, Zhang H, Kallen MA, Routbort MJ, Lal LS, Vierling JM, Suarez-Almazor ME. Low rates of hepatitis B virus screening at the onset of chemotherapy. J Oncol Pract 2012;8:e32-9. [PubMed]
97. Ichai P, Samuel D. Etiology and prognosis of fulminant hepatitis in adults. Liver Transpl 2008;14 Suppl 2:S67-79. [PubMed]
98. Iloeje UH, Yang HI, Su J, Jen CL, You SL, Chen CJ. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology 2006;130:678-86. [PubMed]
99. Ito K, Tanaka Y, Kato M, Fujiwara K, Sugauchi F, Sakamoto T, Shinkai N, Orito E, Mizokami M. Comparison of complete sequences of hepatitis B virus genotype C between inactive carriers and hepatocellular carcinoma patients before and after seroconversion. J Gastroenterol 2007;42:837-44. [PubMed]
100. Jang JW, Kwon JH, You CR, Kim JD, Woo HY, Bae SH, Choi JY, Yoon SK, Chung KW. Risk of HBV reactivation according to viral status and treatment intensity in patients with hepatocellular carcinoma. Antivir Ther 2011;16:969-77. [PubMed]
101. Janssen HL, van Zonneveld M, Senturk H, Zeuzem S, Akarca US, Cakaloglu Y, Simon C, So TM, Gerken G, de Man RA, Niesters HG, Zondervan P, Hansen B, Schalm SW. Pegylated interferon alfa-2b alone or in combination with lamivudine for HBeAg-positive chronic hepatitis B: a randomised trial. Lancet 2005;365:123-9. [PubMed]
102. Joshi D, O'Grady J, Dieterich D, Gazzard B, Agarwal K. Increasing burden of liver disease in patients with HIV infection. Lancet 2011;377:1198-209. [PubMed]
103. Kamiyama T, Yokoo H, Furukawa J, Kurogochi M, Togashi T, Miura N, Nakanishi K, Kamachi H, Kakisaka T, Tsuruga Y, Fujiyoshi M, Taketomi A, Nishimura S, Todo S. Identification of novel serum biomarkers of hepatocellular carcinoma using glycomic analysis. Hepatology 2013;57:2314-25. [PubMed]
104. Kane MA. Global control of primary hepatocellular carcinoma with hepatitis B vaccine: the contributions of research in Taiwan. Cancer Epidemiol Biomarkers Prev 2003;12:2-3. [PubMed]
105. Kao JH, Chen PJ, Lai MY, Chen DS. Hepatitis B genotypes correlate with clinical outcomes in patients with chronic hepatitis B. Gastroenterology 2000;118:554-9. [PubMed]
106. Kao JH, Chen PJ, Lai MY, Chen DS. Basal core promoter mutations of hepatitis B virus increase the risk of hepatocellular carcinoma in hepatitis B carriers. Gastroenterology 2003;124:327-34. [PubMed]
107. Keeffe EB, Dieterich DT, Han SH, Jacobson IM, Martin P, Schiff ER, Tobias H. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2008 update. Clin Gastroenterol Hepatol 2008;6:1315-41. [PubMed]
108. Kim WR, Benson JT, Therneau TM, Torgerson HA, Yawn BP, Melton LJ, 3rd. Changing epidemiology of hepatitis B in a U.S. community. Hepatology 2004;39:811-6. [PubMed]
109. King RW, Ladner SK, Miller TJ, Zaifert K, Perni RB, Conway SC, Otto MJ. Inhibition of human hepatitis B virus replication by AT-61, a phenylpropenamide derivative, alone and in combination with (-)beta-L-2',3'-dideoxy-3'-thiacytidine. Antimicrob Agents Chemother 1998;42:3179-86. [PubMed]
110. Klingmuller U, Schaller H. Hepadnavirus infection requires interaction between the viral pre-S domain and a specific hepatocellular receptor. J Virol 1993;67:7414-22. [PubMed]
111. Konishi M, Wu CH, and Wu GY. Inhibition of HBV replication by siRNA in a stable HBV-producing cell line. Hepatology 2003;38:842-50. [PubMed]
112. Korba BE and Gerin JL. Antisense oligonucleotides are effective inhibitors of hepatitis B virus replication in vitro. Antiviral Res 1995;28:225-42. [PubMed]
113. Kramvis A, Kew M, Francois G. Hepatitis B virus genotypes. Vaccine 2005;23:2409-23. [PubMed]
114. Kramvis A and Kew MC. Relationship of genotypes of hepatitis B virus to mutations, disease progression and response to antiviral therapy. J Viral Hepat 2005;12:456-64. [PubMed]
115. Kruse RL, Kramer JR, Tyson GL, Duan Z, Chen L, El-Serag HB, Kanwal F. Clinical outcomes of hepatitis B virus coinfection in a United States cohort of hepatitis C virus-infected patients. Hepatology 2014;60:1871-8. [PubMed]
-
116. Kumar M, Satapathy S, Monga R, Das K, Hissar S, Pande C, Sharma BC, and Sarin SK. A randomized controlled trial of lamivudine to treat acute hepatitis B. Hepatology 2007;45:97-101. [PubMed]
117. Kumar M, Jung SY, Hodgson AJ, Madden CR, Qin J, Slagle BL. Hepatitis B virus regulatory HBx protein binds to adaptor protein IPS-1 and inhibits the activation of beta interferon. J Virol 2011;85:987-95. [PubMed]
118. Lai CL, Shouval D, Lok AS, Chang TT, Cheinquer H, Goodman Z, DeHertogh D, Wilber R, Zink RC, Cross A, Colonno R, Fernandes L. Entecavir versus lamivudine for patients with HBeAg-negative chronic hepatitis B. N Engl J Med 2006;354:1011-20. [PubMed]
119. Lai CL, Gane E, Liaw YF, Hsu CW, Thongsawat S, Wang Y, Chen Y, Heathcote EJ, Rasenack J, Bzowej N, Naoumov NV, Di Bisceglie AM, Zeuzem S, Moon YM, Goodman Z, Chao G, Constance BF, Brown NA. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med 2007;357:2576-88. [PubMed]
120. Lang T, Lo C, Skinner N, Locarnini S, Visvanathan K, Mansell A. The hepatitis B e antigen (HBeAg) targets and suppresses activation of the toll-like receptor signaling pathway. J Hepatol 2011;55:762-9. [PubMed]
121. Lau GK, Piratvisuth T, Luo KX, Marcellin P, Thongsawat S, Cooksley G, Gane E, Fried MW, Chow WC, Paik SW, Chang WY, Berg T, Flisiak R, McCloud P, Pluck N. Peginterferon Alfa-2a, lamivudine, and the combination for HBeAg-positive chronic hepatitis B. N Engl J Med 2005;352:2682-95. [PubMed]
122. Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J Viral Hepat 2004;11:97-107. [PubMed]
123. Lazar C, Durantel D, Macovei A, Zitzmann N, Zoulim F, Dwek RA, Branza-Nichita N. Treatment of hepatitis B virus-infected cells with alpha-glucosidase inhibitors results in production of virions with altered molecular composition and infectivity. Antiviral Res 2007;76:30-7. [PubMed]
124. Lee C, Gong Y, Brok J, Boxall EH, Gluud C. Effect of hepatitis B immunisation in newborn infants of mothers positive for hepatitis B surface antigen: systematic review and meta-analysis. BMJ 2006;332:328-36. [PubMed]
125. Lee MS, Kim DH, Kim H, Lee HS, Kim CY, Park TS, Yoo KY, Park BJ, Ahn YO. Hepatitis B vaccination and reduced risk of primary liver cancer among male adults: a cohort study in Korea. Int J Epidemiol 1998;27:316-9. [PubMed]
126. Lee WM. Etiologies of acute liver failure. Semin Liver Dis 2008;28:142-52. [PubMed]
127. Lewden C, Salmon D, Morlat P, Bevilacqua S, Jougla E, Bonnet F, Heripret L, Costagliola D, May T, Chene G. Causes of death among human immunodeficiency virus (HIV)-infected adults in the era of potent antiretroviral therapy: emerging role of hepatitis and cancers, persistent role of AIDS. Int J Epidemiol 2005;34:121-30. [PubMed]
128. Liang TJ. Hepatitis B: the virus and disease. Hepatology 2009;49:S13-21. [PubMed]
129. Liaw YF, Sung JJ, Chow WC, Farrell G, Lee CZ, Yuen H, Tanwandee T, Tao QM, Shue K, Keene ON, Dixon JS, Gray DF, and Sabbat J. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med 2004;351:1521-31. [PubMed]
130. Liaw YF, Gane E, Leung N, Zeuzem S, Wang Y, Lai CL, Heathcote EJ, Manns M, Bzowej N, Niu J, Han SH, Hwang SG, Cakaloglu Y, Tong MJ, Papatheodoridis G, Chen Y, Brown NA, Albanis E, Galil K, Naoumov NV. 2-Year GLOBE trial results: telbivudine Is superior to lamivudine in patients with chronic hepatitis B. Gastroenterology 2009;136:486-95. [PubMed]
131. Liaw YF, Raptopoulou-Gigi M, Cheinquer H, Sarin SK, Tanwandee T, Leung N, Peng CY, Myers RP, Brown RS, Jr., Jeffers L, Tsai N, Bialkowska J, Tang S, Beebe S, Cooney E. Efficacy and safety of entecavir versus adefovir in chronic hepatitis B patients with hepatic decompensation: a randomized, open-label study. Hepatology 2011;54:91-100. [PubMed]
132. Liaw YF, Sheen IS, Lee CM, Akarca US, Papatheodoridis GV, Suet-Hing Wong F, Chang TT, Horban A, Wang C, Kwan P, Buti M, Prieto M, Berg T, Kitrinos K, Peschell K, Mondou E, Frederick D, Rousseau F, and Schiff ER. Tenofovir disoproxil fumarate (TDF), emtricitabine/TDF, and entecavir in patients with decompensated chronic hepatitis B liver disease. Hepatology 2011;53:62-72. [PubMed]
133. Liaw YF, Kao J, Piratsivuth T, Chan HL, Chien R, Liu C, Gane E, Locarnini S, Lim SG, Han KH, Amarapurkar D, Cooksley G, Jafri W, Mohamed R, Hou J, Chuang WL, Lesmana LA, Sollano JD, Suh DJ, Omata M. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2012 update. Hepatol Int 2012;6:531-561.
134. Lim SG, Ng TM, Kung N, Krastev Z, Volfova M, Husa P, Lee SS, Chan S, Shiffman ML, Washington MK, Rigney A, Anderson J, Mondou E, Snow A, Sorbel J, Guan R, Rousseau F. A double-blind placebo-controlled study of emtricitabine in chronic hepatitis B. Arch Intern Med 2006;166:49-56. [PubMed]
135. Lin CL, Liao LY, Wang CS, Chen PJ, Lai MY, Chen DS, Kao JH. Basal core-promoter mutant of hepatitis B virus and progression of liver disease in hepatitis B e antigen-negative chronic hepatitis B. Liver Int 2005;25:564-70. [PubMed]
136. Lin CL, Liu CH, Chen W, Huang WL, Chen PJ, Lai MY, Chen DS, Kao JH. Association of pre-S deletion mutant of hepatitis B virus with risk of hepatocellular carcinoma. J Gastroenterol Hepatol 2007;22:1098-103. [PubMed]
137. Liu CJ, Chen PJ, Lai MY, Kao JH, Jeng YM, Chen DS. Ribavirin and interferon is effective for hepatitis C virus clearance in hepatitis B and C dually infected patients. Hepatology 2003;37:568-76. [PubMed]
138. Liu CJ, Chen BF, Chen PJ, Lai MY, Huang WL, Kao JH, Chen DS. Role of hepatitis B viral load and basal core promoter mutation in hepatocellular carcinoma in hepatitis B carriers. J Infect Dis 2006;193:1258-65. [PubMed]
139. Liu CJ, Chen BF, Chen PJ, Lai MY, Huang WL, Kao JH, Chen DS. Role of hepatitis B virus precore/core promoter mutations and serum viral load on noncirrhotic hepatocellular carcinoma: a case-control study. J Infect Dis 2006;194:594-9. [PubMed]
140. Liu S, Zhang H, Gu C, Yin J, He Y, Xie J, and Cao G. Associations between hepatitis B virus mutations and the risk of hepatocellular carcinoma: a meta-analysis. J Natl Cancer Inst 2009;101:1066-82. [PubMed]
141. Liu Z, Ma Y, Yang J, Qin H. Upregulated and downregulated proteins in hepatocellular carcinoma: a systematic review of proteomic profiling studies. OMICS 2011;15:61-71. [PubMed]
142. Livingston SE, Simonetti JP, Bulkow LR, Homan CE, Snowball MM, Cagle HH, Negus SE, McMahon BJ. Clearance of hepatitis B e antigen in patients with chronic hepatitis B and genotypes A, B, C, D, and F. Gastroenterology 2007;133:1452-7. [PubMed]
143. Livingston SE, Simonetti JP, McMahon BJ, Bulkow LR, Hurlburt KJ, Homan CE, Snowball MM, Cagle HH, Williams JL, Chulanov VP. Hepatitis B virus genotypes in Alaska Native people with hepatocellular carcinoma: preponderance of genotype F. J Infect Dis 2007;195:5-11. [PubMed]
144. Locarnini S. Molecular virology and the development of resistant mutants: implications for therapy. Semin Liver Dis 2005;25 Suppl 1:9-19. [PubMed]
145. Locarnini S, Shaw T, Dean J, Colledge D, Thompson A, Li K, Lemon SM, Lau GG, Beard MR. Cellular response to conditional expression of the hepatitis B virus precore and core proteins in cultured hepatoma (Huh-7) cells. J Clin Virol 2005;32:113-21. [PubMed]
146. Lok AS, Lai CL, Leung N, Yao GB, Cui ZY, Schiff ER, Dienstag JL, Heathcote EJ, Little NR, Griffiths DA, Gardner SD, Castiglia M. Long-term safety of lamivudine treatment in patients with chronic hepatitis B. Gastroenterology 2003;125:1714-22. [PubMed]
147. Lok AS, Zoulim F, Locarnini S, Bartholomeusz A, Ghany MG, Pawlotsky JM, Liaw YF, Mizokami M, Kuiken C. Antiviral drug-resistant HBV: standardization of nomenclature and assays and recommendations for management. Hepatology 2007;46:254-65. [PubMed]
148. Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology 2009;50:661-2. [PubMed]
149. Lok AS, Trinh H, Carosi G, Akarca US, Gadano A, Habersetzer F, Sievert W, Wong D, Lovegren M, Cohen D, Llamoso C. Efficacy of entecavir with or without tenofovir disoproxil fumarate for nucleos(t)ide-naive patients with chronic hepatitis B. Gastroenterology 2012;143:619-28. [PubMed]
150. Loomba R, Liang TJ. Novel approaches to new therapies for hepatitis B virus infection. Antivir Ther 2006;11:1-15. [PubMed]
151. Loomba R, Rowley A, Wesley R, Liang TJ, Hoofnagle JH, Pucino F, Csako G. Systematic review: the effect of preventive lamivudine on hepatitis B reactivation during chemotherapy. Ann Intern Med 2008;148:519-28. [PubMed]
152. Maini MK, Boni C, Ogg GS, King AS, Reignat S, Lee CK, Larrubia JR, Webster GJ, McMichael AJ, Ferrari C, Williams R, Vergani D, Bertoletti A. Direct ex vivo analysis of hepatitis B virus-specific CD8(+) T cells associated with the control of infection. Gastroenterology 1999;117:1386-96. [PubMed]
153. Maini MK, Boni C, Lee CK, Larrubia JR, Reignat S, Ogg GS, King AS, Herberg J, Gilson R, Alisa A, Williams R, Vergani D, Naoumov NV, Ferrari C, Bertoletti A. The role of virus-specific CD8(+) cells in liver damage and viral control during persistent hepatitis B virus infection. J Exp Med 2000;191:1269-80. [PubMed]
154. Marcellin P, Lau GK, Bonino F, Farci P, Hadziyannis S, Jin R, Lu ZM, Piratvisuth T, Germanidis G, Yurdaydin C, Diago M, Gurel S, Lai MY, Button P, Pluck N. Peginterferon alfa-2a alone, lamivudine alone, and the two in combination in patients with HBeAg-negative chronic hepatitis B. N Engl J Med 2004;351:1206-17. [PubMed]
155. Marcellin P, Heathcote EJ, Buti M, Gane E, de Man RA, Krastev Z, Germanidis G, Lee SS, Flisiak R, Kaita K, Manns M, Kotzev I, Tchernev K, Buggisch P, Weilert F, Kurdas OO, Shiffman ML, Trinh H, Washington MK, Sorbel J, Anderson J, Snow-Lampart A, Mondou E, Quinn J, Rousseau F. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med 2008;359:2442-55. [PubMed]
156. Marcellin P, Gane E, Buti M, Afdhal N, Sievert W, Jacobson IM, Washington MK, Germanidis G, Flaherty JF, Schall RA, Bornstein JD, Kitrinos KM, Subramanian GM, McHutchison JG, Heathcote EJ. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up study. Lancet 2013;381:468-75. [PubMed]
157. Marcellin P, Ahn SH, Ma H, Caruntu FA, Tak WY, Elkashab M, Chuang WL, Tabak F, Mehta R, Petersen J, Martins EB, Dinh P, Corsa AC, Charuworn P, Subramanian M, McHutchinson JG, Buti M, Gaeta GB, Papatheodoridis GV, Flisiak R, Chan HL. HBsAg loss with tenofovir disoproxil fumarate (TDF) plus peginterferon alfa-2a (PEG) in chronic hepatitis B (CHB): Results of a global randomized controlled trial. Hepatology 2014;60 (Suppl 1):294A.
158. Marcellin P, Gane E, Flisiak R, Trinh H, Petersen J, Gurel S, Kaita KD, Kotzev IA, Tsai N, Flaherty JF, Augilar Schall RE, Kitrinos KM, Subramanian M, McHutchinson JG, George J, Janssen HL, and Buti M. Long term treatment with tenofovir disoproxil fumarate for chronic hepatitis B infection is safe and well tolerated and associated with durable virologic response with no detectable resistance: 8 year results from two phase 3 trials [abstract]. Hepatology 2014;60 (Suppl 1):313A-314A.
159. Marrero JA, Feng Z, Wang Y, Nguyen MH, Befeler AS, Roberts LR, Reddy KR, Harnois D, Llovet JM, Normolle D, Dalhgren J, Chia D, Lok AS, Wagner PD, Srivastava S, Schwartz M. Alpha-fetoprotein, des-gamma carboxyprothrombin, and lectin-bound alpha-fetoprotein in early hepatocellular carcinoma. Gastroenterology 2009;137:110-8. [PubMed]
160. Mast EE, Weinbaum CM, Fiore AE, Alter MJ, Bell BP, Finelli L, Rodewald LE, Douglas JM, Janssen RS, Ward JW. A comprehensive Immunization strategy to eliminate transmission of hepatitis B virus infection in the United States. MMWR Recomm Rep 2006;55:1-25. [PubMed]
161. McCaffrey AP, Nakai H, Pandey K, Huang Z, Salazar FH, Xu H, Wieland SF, Marion PL, Kay MA. Inhibition of hepatitis B virus in mice by RNA interference. Nat Biotechnol 2003;21:639-44. [PubMed]
162. McMahon BJ, Holck P, Bulkow L, Snowball M. Serologic and clinical outcomes of 1536 Alaska Natives chronically infected with hepatitis B virus. Ann Intern Med 2001;135:759-68. [PubMed]
163. McMahon BJ. The natural history of chronic hepatitis B virus infection. Hepatology 2009;49:S45-55. [PubMed]
164. Milich D and Liang TJ. Exploring the biological basis of hepatitis B e antigen in hepatitis B virus infection. Hepatology 2003;38:1075-86. [PubMed]
165. Moucari R, Mackiewicz V, Lada O, Ripault MP, Castelnau C, Martinot-Peignoux M, Dauvergne A, Asselah T, Boyer N, Bedossa P, Valla D, Vidaud M, Nicolas-Chanoine MH, Marcellin P. Early serum HBsAg drop: a strong predictor of sustained virological response to pegylated interferon alfa-2a in HBeAg-negative patients. Hepatology 2009;49:1151-7. [PubMed]
166. Murray JM, Wieland SF, Purcell RH, Chisari FV. Dynamics of hepatitis B virus clearance in chimpanzees. Proc Natl Acad Sci USA 2005;102:17780-5. [PubMed]
167. Nayersina R, Fowler P, Guilhot S, Missale G, Cerny A, Schlicht HJ, Vitiello A, Chesnut R, Person JL, Redeker AG, Chisari FV. HLA A2 restricted cytotoxic T lymphocyte responses to multiple hepatitis B surface antigen epitopes during hepatitis B virus infection. J Immunol 1993;150:4659-71. [PubMed]
168. Nelson PK, Mathers BM, Cowie B, Hagan H, Des Jarlais D, Horyniak D, Degenhardt L. Global epidemiology of hepatitis B and hepatitis C in people who inject drugs: results of systematic reviews. Lancet 2011;378:571-83. [PubMed]
169. Nguyen G, Garcia RT, Nguyen N, Trinh H, Keeffe EB, Nguyen MH. Clinical course of hepatitis B virus infection during pregnancy. Aliment Pharmacol Ther 2009;29:755-64. [PubMed]
170. Ni YH, Chang MH, Huang LM, Chen HL, Hsu HY, Chiu TY, Tsai KS, Chen DS. Hepatitis B virus infection in children and adolescents in a hyperendemic area: 15 years after mass hepatitis B vaccination. Ann Intern Med 2001;135:796-800. [PubMed]
171. Ni YH, Huang LM, Chang MH, Yen CJ, Lu CY, You SL, Kao JH, Lin YC, Chen HL, Hsu HY, Chen DS. Two decades of universal hepatitis B vaccination in taiwan: impact and implication for future strategies. Gastroenterology 2007;132:1287-93. [PubMed]
172. Niro GA, Ciancio A, Gaeta GB, Smedile A, Marrone A, Olivero A, Stanzione M, David E, Brancaccio G, Fontana R, Perri F, Andriulli A, Rizzetto M. Pegylated interferon alpha-2b as monotherapy or in combination with ribavirin in chronic hepatitis delta. Hepatology 2006;44:713-20. [PubMed]
173. Noordeen F, Vaillant A, Jilbert AR. Nucleic acid polymers inhibit duck hepatitis B virus infection in vitro. Antimicrob Agents Chemother 2013;57:5291-8. [PubMed]
174. Noordeen F, Vaillant A, Jilbert AR. Nucleic acid polymers prevent the establishment of duck hepatitis B virus infection in vivo. Antimicrob Agents Chemother 2013;57:5299-306. [PubMed]
175. Nowak MA, Bonhoeffer S, Hill AM, Boehme R, Thomas HC, McDade H. Viral dynamics in hepatitis B virus infection. Proc Natl Acad Sci U S A 1996;93:4398-402. [PubMed]
176. O'Grady JG, Alexander GJ, Hayllar KM, Williams R. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology 1989;97:439-45. [PubMed]
177. Omata M, Lesmana LA, Tateishi R, Chen PJ, Lin SM, Yoshida H, Kudo M, Lee JM, Choi BI, Poon RT, Shiina S, Cheng AL, Jia JD, Obi S, Han KH, Jafri W, Chow P, Lim SG, Chawla YK, Budihusodo U, Gani RA, Lesmana CR, Putranto TA, Liaw YF, Sarin SK. Asian Pacific Association for the Study of the Liver consensus recommendations on hepatocellular carcinoma. Hepatol Int 2010;4:439-74. [PubMed]
178. Ott JJ, Stevens GA, Groeger J, Wiersma ST. Global epidemiology of hepatitis B virus infection: new estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine 2012;30:2212-9. [PubMed]
179. Ouseph R, Eng M, Ravindra K, Brock GN, Buell JF, Marvin MR. Review of the use of hepatitis B core antibody-positive kidney donors. Transplant Rev (Orlando) 2010;24:167-71. [PubMed]
180. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005;55:74-108. [PubMed]
181. Parkin DM. The global health burden of infection-associated cancers in the year 2002. Int J Cancer 2006;118:3030-44. [PubMed]
182. Penna A, Chisari FV, Bertoletti A, Missale G, Fowler P, Giuberti T, Fiaccadori F, Ferrari C. Cytotoxic T lymphocytes recognize an HLA-A2-restricted epitope within the hepatitis B virus nucleocapsid antigen. J Exp Med 1991;174:1565-70.
183. Perez-Alvarez R, Diaz-Lagares C, Garcia-Hernandez F, Lopez-Roses L, Brito-Zeron P, Perez-de-Lis M, Retamozo S, Bove A, Bosch X, Sanchez-Tapias JM, Forns X, Ramos-Casals M, and Group BS. Hepatitis B virus (HBV) reactivation in patients receiving tumor necrosis factor (TNF)-targeted therapy: analysis of 257 cases. Medicine 2011;90:359-71. [PubMed]
184. Perni RB, Conway SC, Ladner SK, Zaifert K, Otto MJ, King RW. Phenylpropenamide derivatives as inhibitors of hepatitis B virus replication. Bioorg Med Chem Lett 2000;10:2687-90. [PubMed]
185. Perrillo R, Tamburro C, Regenstein F, Balart L, Bodenheimer H, Silva M, Schiff E, Bodicky C, Miller B, Denham C, and et al. Low-dose, titratable interferon alfa in decompensated liver disease caused by chronic infection with hepatitis B virus. Gastroenterology 1995;109:908-16. [PubMed]
186. Perrillo RP. Therapy of hepatitis B -- viral suppression or eradication? Hepatology 2006;43:S182-93. [PubMed]
187. Perrillo RP, Gish R, Falck-Ytter YT. American Gastroenterological Association Institute Technical Review on Prevention and Treatment of Hepatitis B Reactivation During Immunosuppressive Drug Therapy. Gastroenterology 2014;148:221-24. [PubMed]
188. Petersen J, Ratziu V, Buti M, Janssen HL, Brown A, Lampertico P, Schollmeyer J, Zoulim F, Wedemeyer H, Sterneck M, Berg T, Sarrazin C, Lutgehetmann M, Buggisch P. Entecavir Plus Tenofovir Combination as Rescue Therapy in Pretreated Chronic Hepatitis B Patients. An International Multicenter Cohort Study. J Hepatol 2011;56:520-6. [PubMed]
189. Phillips S, Chokshi S, Riva A, Evans A, Williams R, Naoumov NV. CD8(+) T cell control of hepatitis B virus replication: direct comparison between cytolytic and noncytolytic functions. J Immunol 2010;184:287-95. [PubMed]
190. Polish LB, Gallagher M, Fields HA, Hadler SC. Delta hepatitis: molecular biology and clinical and epidemiological features. Clin Microbiol Rev 1993;6:211-29. [PubMed]
191. Potthoff A, Wedemeyer H, Boecher WO, Berg T, Zeuzem S, Arnold J, Spengler U, Gruengreiff K, Kaeser T, Schuchmann M, Bergk A, Forestier N, Deterding K, Manns MP, Trautwein C. The HEP-NET B/C co-infection trial: A prospective multicenter study to investigate the efficacy of pegylated interferon-alpha2b and ribavirin in patients with HBV/HCV co-infection. J Hepatol 2008;49:688-94. [PubMed]
192. Rabe B, Vlachou A, Pante N, Helenius A, Kann M. Nuclear import of hepatitis B virus capsids and release of the viral genome. Proc Natl Acad Sci U S A 2003;100:9849-54. [PubMed]
193. Rapti I, Dimou E, Mitsoula P, Hadziyannis SJ. Adding-on versus switching-to adefovir therapy in lamivudine-resistant HBeAg-negative chronic hepatitis B. Hepatology 2007;45:307-13. [PubMed]
194. Rehermann B, Fowler P, Sidney J, Person J, Redeker A, Brown M, Moss B, Sette A, Chisari FV. The cytotoxic T lymphocyte response to multiple hepatitis B virus polymerase epitopes during and after acute viral hepatitis. J Exp Med 1995;181:1047-58. [PubMed]
195. Rehermann B. Intrahepatic T cells in hepatitis B: viral control versus liver cell injury. J Exp Med 2000;191:1263-8. [PubMed]
196. Reiss G, Keeffe EB. Review article: hepatitis vaccination in patients with chronic liver disease. Aliment Pharmacol Ther 2004;19:715-27. [PubMed]
197. Rijckborst V, ter Borg MJ, Cakaloglu Y, Ferenci P, Tabak F, Akdogan M, Simon K, Raptopoulou-Gigi M, Ormeci N, Zondervan PE, Verhey E, van Vuuren AJ, Hansen BE, Janssen HL. A randomized trial of peginterferon alpha-2a with or without ribavirin for HBeAg-negative chronic hepatitis B. Am J Gastroenterol 2010;105:1762-9. [PubMed]
198. Robaczewska M, Guerret S, Remy JS, Chemin I, Offensperger WB, Chevallier M, Behr JP, Podhajska AJ, Blum HE, Trepo C, Cova L. Inhibition of hepadnaviral replication by polyethylenimine-based intravenous delivery of antisense phosphodiester oligodeoxynucleotides to the liver. Gene Ther 2001;8:874-81. [PubMed]
199. Roush SW, Murphy TV. Historical comparisons of morbidity and mortality for vaccine-preventable diseases in the United States. Jama 2007;298:2155-63. [PubMed]
200. Saab S, Waterman B, Chi AC, Tong MJ. Comparison of different immunoprophylaxis regimens after liver transplantation with hepatitis B core antibody-positive donors: a systematic review. Liver Transpl 2010;16:300-7. [PubMed]
201. Schaefer S. Hepatitis B virus taxonomy and hepatitis B virus genotypes. World J Gastroenterol 2007;13:14-21. [PubMed]
202. Schiff E, Simsek H, Lee WM, Chao YC, Sette H, Jr., Janssen HL, Han SH, Goodman Z, Yang J, Brett-Smith H, Tamez R. Efficacy and safety of entecavir in patients with chronic hepatitis B and advanced hepatic fibrosis or cirrhosis. Am J Gastroenterol 2008;103:2776-83. [PubMed]
203. Sebestyen MG, Wong SC, Trubetskoy V, Lewis DL, Wooddell CI. Targeted in vivo delivery of siRNA and an endosome-releasing agent to hepatocytes. Methods Mol Biol 2015;1218:163-86. [PubMed]
204. Seo Y, Yano Y. Short- and long-term outcome of interferon therapy for chronic hepatitis B infection. World J Gastroenterol 2014;20:13284-92. [PubMed]
205. Shakil AO, Kramer D, Mazariegos GV, Fung JJ, Rakela J. Acute liver failure: clinical features, outcome analysis, and applicability of prognostic criteria. Liver Transpl 2000;6:163-9. [PubMed]
-
206. Sharma P, Lok A. Viral hepatitis and liver transplantation. Semin Liver Dis 2006;26:285-97. [PubMed]
207. Shouval D, Shibolet O. Immunosuppression and HBV reactivation. Semin Liver Dis 2013;33:167-77. [PubMed]
208. Singal AK, Salameh H, Kuo YF, Fontana RJ. Meta-analysis: the impact of oral anti-viral agents on the incidence of hepatocellular carcinoma in chronic hepatitis B. Aliment Pharmacol Ther 2013;38:98-106. [PubMed]
209. Stray SJ, Bourne CR, Punna S, Lewis WG, Finn MG, Zlotnick A. A heteroaryldihydropyrimidine activates and can misdirect hepatitis B virus capsid assembly. Proc Natl Acad Sci U S A 2005;102:8138-43. [PubMed]
210. Sugauchi F, Ohno T, Orito E, Sakugawa H, Ichida T, Komatsu M, Kuramitsu T, Ueda R, Miyakawa Y, Mizokami M. Influence of hepatitis B virus genotypes on the development of preS deletions and advanced liver disease. J Med Virol 2003;70:537-44. [PubMed]
211. Tanaka Y, Mukaide M, Orito E, Yuen MF, Ito K, Kurbanov F, Sugauchi F, Asahina Y, Izumi N, Kato M, Lai CL, Ueda R, Mizokami M. Specific mutations in enhancer II/core promoter of hepatitis B virus subgenotypes C1/C2 increase the risk of hepatocellular carcinoma. J Hepatol 2006;45:646-53. [PubMed]
212. Tenney DJ, Pokornowski KA, Rose RE, Baldick CJ, Eggers BJ, Fang J, Wichroski MJ, Diva UA, Xu D, Wilber RB, Brett-Smith H, Iloeje UH. Entecavir maintains a high genetic barrier to HBV resistance through 6 years in naive patients [abstract]. J Hepatol 2009;50:S10.
213. Tenney DJ, Rose RE, Baldick CJ, Pokornowski KA, Eggers BJ, Fang J, Wichroski MJ, Xu D, Yang J, Wilber RB, Colonno RJ. Long-term monitoring shows hepatitis B virus resistance to entecavir in nucleoside-naive patients is rare through 5 years of therapy. Hepatology 2009;49:1503-14. [PubMed]
214. ter Borg MJ, Leemans WF, de Man RA, Janssen HL. Exacerbation of chronic hepatitis B infection after delivery. J Viral Hepat 2008;15:37-41. [PubMed]
215. Terrault NA. Benefits and risks of combination therapy for hepatitis B. Hepatology 2009;49:S122-8. [PubMed]
216. Thimme R, Wieland S, Steiger C, Ghrayeb J, Reimann KA, Purcell RH, Chisari FV. CD8(+) T cells mediate viral clearance and disease pathogenesis during acute hepatitis B virus infection. J Virol 2003;77:68-76. [PubMed]
217. Thio CL, Seaberg EC, Skolasky R, Jr., Phair J, Visscher B, Munoz A, Thomas DL. HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet 2002;360:1921-6. [PubMed]
218. Thio CL. Hepatitis B and human immunodeficiency virus coinfection. Hepatology 2009;49:S138-45. [PubMed]
219. Tillmann HL, Hadem J, Leifeld L, Zachou K, Canbay A, Eisenbach C, Graziadei I, Encke J, Schmidt H, Vogel W, Schneider A, Spengler U, Gerken G, Dalekos GN, Wedemeyer H, Manns MP. Safety and efficacy of lamivudine in patients with severe acute or fulminant hepatitis B, a multicenter experience. J Viral Hepat 2006;13:256-63. [PubMed]
220. Tomai E, Butz K, Lohrey C, von Weizsacker F, Zentgraf H, Hoppe-Seyler F. Peptide aptamer-mediated inhibition of target proteins by sequestration into aggresomes. J Biol Chem 2006;281:21345-52. [PubMed]
221. Tong MJ, Blatt LM, Kao JH, Cheng JT, Corey WG. Basal core promoter T1762/A1764 and precore A1896 gene mutations in hepatitis B surface antigen-positive hepatocellular carcinoma: a comparison with chronic carriers. Liver Int 2007;27:1356-63. [PubMed]
222. Toyoda H, Kumada T, Tada T. Highly sensitive Lens culinaris agglutinin-reactive alpha-fetoprotein: a new tool for the management of hepatocellular carcinoma. Oncology 2011;81 Suppl 1:61-5. [PubMed]
223. van Bommel F, de Man RA, Wedemeyer H, Deterding K, Petersen J, Buggisch P, Erhardt A, Huppe D, Stein K, Trojan J, Sarrazin C, Bocher WO, Spengler U, Wasmuth HE, Reinders JG, Moller B, Rhode P, Feucht HH, Wiedenmann B, Berg T. Long-term efficacy of tenofovir monotherapy for hepatitis B virus-monoinfected patients after failure of nucleoside/nucleotide analogues. Hepatology 2010;51:73-80. [PubMed]
224. Villa E, Grottola A, Buttafoco P, Colantoni A, Bagni A, Ferretti I, Cremonini C, Bertani H, Manenti F. High doses of alpha-interferon are required in chronic hepatitis due to coinfection with hepatitis B virus and hepatitis C virus: long term results of a prospective randomized trial. Am J Gastroenterol 2001;96:2973-7. [PubMed]
225. Vincent IE, Zannetti C, Lucifora J, Norder H, Protzer U, Hainaut P, Zoulim F, Tommasino M, Trepo C, Hasan U, Chemin I. Hepatitis B virus impairs TLR9 expression and function in plasmacytoid dendritic cells. PLoS One 2011;6:e26315. [PubMed]
226. Visvanathan K, Skinner NA, Thompson AJ, Riordan SM, Sozzi V, Edwards R, Rodgers S, Kurtovic J, Chang J, Lewin S, Desmond P, Locarnini S. Regulation of Toll-like receptor-2 expression in chronic hepatitis B by the precore protein. Hepatology 2007;45:102-10. [PubMed]
227. Volz T, Allweiss L, Ben MM, Warlich M, Lohse AW, Pollok JM, Alexandrov A, Urban S, Petersen J, Lutgehetmann M, Dandri M. The entry inhibitor Myrcludex-B efficiently blocks intrahepatic virus spreading in humanized mice previously infected with hepatitis B virus. J Hepatol 2013;58:861-7. [PubMed]
228. Wachs ME, Amend WJ, Ascher NL, Bretan PN, Emond J, Lake JR, Melzer JS, Roberts JP, Tomlanovich SJ, Vincenti F, et al. The risk of transmission of hepatitis B from HBsAg(-), HBcAb(+), HBIgM(-) organ donors. Transplantation 1995;59:230-4. [PubMed]
229. Wai CT, Fontana RJ, Polson J, Hussain M, Shakil AO, Han SH, Davern TJ, Lee WM, Lok AS. Clinical outcome and virological characteristics of hepatitis B-related acute liver failure in the United States. J Viral Hepat 2005;12:192-8. [PubMed]
230. Wang H, Ryu WS. Hepatitis B virus polymerase blocks pattern recognition receptor signaling via interaction with DDX3: implications for immune evasion. PLoS Pathog 2010;6:e1000986.[PubMed]
231. Wang HC, Huang W, Lai MD, Su IJ. Hepatitis B virus pre-S mutants, endoplasmic reticulum stress and hepatocarcinogenesis. Cancer Sci 2006;97:683-8. [PubMed]
232. Wang L, Kourtis AP, Ellington S, Legardy-Williams J, Bulterys M. Safety of tenofovir during pregnancy for the mother and fetus: a systematic review. Clin Infect Dis 2013;57:1773-81. [PubMed]
233. Wang P, Tam N, Wang H, Zheng H, Chen P, Wu L, He X. Is hepatitis B immunoglobulin necessary in prophylaxis of hepatitis B recurrence after liver transplantation? A meta-analysis. PLoS One 2014;9:e104480. [PubMed]
234. Wang X, Li Y, Mao A, Li C, Li Y, Tien P. Hepatitis B virus X protein suppresses virus-triggered IRF3 activation and IFN-beta induction by disrupting the VISA-associated complex. Cell Mol Immunol 2010;7:341-8. [PubMed]
235. Wang Z, Ni J, Li J, Shi B, Xu Y, Yuan Z. Inhibition of hepatitis B virus replication by cIAP2 involves accelerating the ubiquitin-proteasome-mediated destruction of polymerase. J Virol 2011;85:11457-67. [PubMed]
236. Weber O, Schlemmer KH, Hartmann E, Hagelschuer I, Paessens A, Graef E, Deres K, Goldmann S, Niewoehner U, Stoltefuss J, Haebich D, Ruebsamen-Waigmann H, Wohlfeil S. Inhibition of human hepatitis B virus (HBV) by a novel non-nucleosidic compound in a transgenic mouse model. Antiviral Res 2002;54:69-78. [PubMed]
237. Webster GJ, Reignat S, Maini MK, Whalley SA, Ogg GS, King A, Brown D, Amlot PL, Williams R, Vergani D, Dusheiko GM, Bertoletti A. Incubation phase of acute hepatitis B in man: dynamic of cellular immune mechanisms. Hepatology 2000;32:1117-24. [PubMed]
238. Webster GJ, Reignat S, Brown D, Ogg GS, Jones L, Seneviratne SL, Williams R, Dusheiko G, Bertoletti A. Longitudinal analysis of CD8+ T cells specific for structural and nonstructural hepatitis B virus proteins in patients with chronic hepatitis B: implications for immunotherapy. J Virol 2004;78:5707-19. [PubMed]
239. Wei C, Ni C, Song T, Liu Y, Yang X, Zheng Z, Jia Y, Yuan Y, Guan K, Xu Y, Cheng X, Zhang Y, Yang X, Wang Y, Wen C, Wu Q, Shi W, Zhong H. The hepatitis B virus X protein disrupts innate immunity by downregulating mitochondrial antiviral signaling protein. J Immunol 2010;185:1158-68. [PubMed]
240. Weinbaum CM, Williams I, Mast EE, Wang SA, Finelli L, Wasley A, Neitzel SM, Ward JW, Centers for Disease Control and Prevention. Recommendations for identification and public health management of persons with chronic hepatitis B virus infection. MMWR Recomm Rep 2008;57:1-20. [PubMed]
241. Werle-Lapostolle B, Bowden S, Locarnini S, Wursthorn K, Petersen J, Lau G, Trepo C, Marcellin P, Goodman Z, Delaney WEt, Xiong S, Brosgart CL, Chen SS, Gibbs CS, Zoulim F. Persistence of cccDNA during the natural history of chronic hepatitis B and decline during adefovir dipivoxil therapy. Gastroenterology 2004;126:1750-8. [PubMed]
242. Wi CI, Loo NM, Larson JJ, Moynihan TJ, Madde NR, Grendahl DC, Alberts SR, Kim WR. Low Level of HBV Screening Among Patients Receiving Chemotherapy. Clin Gastroenterol Hepatol 2014;pii: S1542-3565(14)01583-3. [PubMed]
243. Wieland S, Thimme R, Purcell RH, Chisari FV. Genomic analysis of the host response to hepatitis B virus infection. Proc Natl Acad Sci U S A 2004;101:6669-74. [PubMed]
244. Wieland SF, Guidotti LG, Chisari FV. Intrahepatic induction of alpha/beta interferon eliminates viral RNA- containing capsids in hepatitis B virus transgenic mice. J Virol 2000;74:4165-73. [PubMed]
245. Wieland SF, Eustaquio A, Whitten-Bauer C, Boyd B, Chisari FV. Interferon prevents formation of replication-competent hepatitis B virus RNA-containing nucleocapsids. Proc Natl Acad Sci U S A 2005;102:9913-7. [PubMed]
246. Wong VW, Chan SL, Mo F, Chan TC, Loong HH, Wong GL, Lui YY, Chan AT, Sung JJ, Yeo W, Chan HL, Mok TS. Clinical scoring system to predict hepatocellular carcinoma in chronic hepatitis B carriers. J Clin Oncol 2010;28:1660-5. [PubMed]
247. Wong VW, Wong GL, Yan KK, Chim AM, Chan HY, Tse CH, Choi PC, Chan AW, Sung JJ, Chan HL. Durability of peginterferon alfa-2b treatment at 5 years in patients with hepatitis B e antigen-positive chronic hepatitis B. Hepatology 2010;51:1945-53. [PubMed]
248. Wu CF, Yu MW, Lin CL, Liu CJ, Shih WL, Tsai KS, Chen CJ. Long-term tracking of hepatitis B viral load and the relationship with risk for hepatocellular carcinoma in men. Carcinogenesis 2008;29:106-12. [PubMed]
249. Wu G, Liu B, Zhang Y, Li J, Arzumanyan A, Clayton MM, Schinazi RF, Wang Z, Goldmann S, Ren Q, Zhang F, Feitelson MA. Preclinical characterization of GLS4, an inhibitor of hepatitis B virus core particle assembly. Antimicrob Agents Chemother 2013;57:5344-54. [PubMed]
250. Wursthorn K, Jung M, Riva A, Goodman ZD, Lopez P, Bao W, Manns MP, Wedemeyer H, Naoumov NV. Kinetics of hepatitis B surface antigen decline during 3 years of telbivudine treatment in hepatitis B e antigen-positive patients. Hepatology 2010;52:1611-20. [PubMed]
251. Xu Y, Hu Y, Shi B, Zhang X, Wang J, Zhang Z, Shen F, Zhang Q, Sun S, Yuan Z. HBsAg inhibits TLR9-mediated activation and IFN-alpha production in plasmacytoid dendritic cells. Mol Immunol 2009;46:2640-6. [PubMed]
252. Yan H, Zhong G, Xu G, He W, Jing Z, Gao Z, Huang Y, Qi Y, Peng B, Wang H, Fu L, Song M, Chen P, Gao W, Ren B, Sun Y, Cai T, Feng X, Sui J, Li W. Sodium taurocholate cotransporting polypeptide is a functional receptor for human hepatitis B and D virus. Elife 2012;1:e00049. [PubMed]
253. Yang HI, Lu SN, Liaw YF, You SL, Sun CA, Wang LY, Hsiao CK, Chen PJ, Chen DS, Chen CJ. Hepatitis B e antigen and the risk of hepatocellular carcinoma. N Engl J Med 2002;347:168-74. [PubMed]
254. Yang HI, Yeh SH, Chen PJ, Iloeje UH, Jen CL, Su J, Wang LY, Lu SN, You SL, Chen DS, Liaw YF, Chen CJ. Associations between hepatitis B virus genotype and mutants and the risk of hepatocellular carcinoma. J Natl Cancer Inst 2008;100:1134-43. [PubMed]
255. Yang HI, Sherman M, Su J, Chen PJ, Liaw YF, Iloeje UH, Chen CJ. Nomograms for risk of hepatocellular carcinoma in patients with chronic hepatitis B virus infection. J Clin Oncol 2010;28:2437-44. [PubMed]
256. Yang HI, Yuen MF, Chan HL, Han KH, Chen PJ, Kim DY, Ahn SH, Chen CJ, Wong VW, and Seto WK. Risk estimation for hepatocellular carcinoma in chronic hepatitis B (REACH-B): development and validation of a predictive score. Lancet Oncol 2011;12:568-574. [PubMed]
257. Yang PL, Althage A, Chung J, Maier H, Wieland S, Isogawa M, Chisari FV. Immune effectors required for hepatitis B virus clearance. Proc Natl Acad Sci U S A 2010;107:798-802. [PubMed]
258. Yim HJ, Lok AS. Natural history of chronic hepatitis B virus infection: what we knew in 1981 and what we know in 2005. Hepatology 2006;43:S173-81. [PubMed]
259. Ying C, Tan S, Cheng YC. Helioxanthin analogue 8-1 inhibits duck hepatitis B virus replication in cell culture. Antivir Chem Chemother 2010;21:97-103.[PubMed]
260. Yu MW, Chang HC, Liaw YF, Lin SM, Lee SD, Liu CJ, Chen PJ, Hsiao TJ, Lee PH, Chen CJ. Familial risk of hepatocellular carcinoma among chronic hepatitis B carriers and their relatives. J Natl Cancer Inst 2000;92:1159-64. [PubMed]
261. Yu MW, Chang HC, Chen PJ, Liu CJ, Liaw YF, Lin SM, Lee SD, Lin SC, Lin CL, Chen CJ. Increased risk for hepatitis B-related liver cirrhosis in relatives of patients with hepatocellular carcinoma in northern Taiwan. Int J Epidemiol 2002;31:1008-15. [PubMed]
262. Yu MW, Yeh SH, Chen PJ, Liaw YF, Lin CL, Liu CJ, Shih WL, Kao JH, Chen DS, Chen CJ. Hepatitis B virus genotype and DNA level and hepatocellular carcinoma: a prospective study in men. J Natl Cancer Inst 2005;97:265-72. [PubMed]
263. Yu S, Chen J, Wu M, Chen H, Kato N, Yuan Z. Hepatitis B virus polymerase inhibits RIG-I- and Toll-like receptor 3-mediated beta interferon induction in human hepatocytes through interference with interferon regulatory factor 3 activation and dampening of the interaction between TBK1/IKKepsilon and DDX3. J Gen Virol 2010;91:2080-90. [PubMed]
264. Yu S, Jianqin H, Wei W, Jianrong H, Yida Y, Jifang S, Liang Y, Zhi C, Hongyu J. The efficacy and safety of nucleos(t)ide analogues in the treatment of HBV-related acute-on-chronic liver failure: a meta-analysis. Ann Hepatol 2013;12:364-72. [PubMed]
265. Yu W, Goddard C, Clearfield E, Mills C, Xiao T, Guo H, Morrey JD, Motter NE, Zhao K, Block TM, Cuconati A, Xu X. Design, synthesis, and biological evaluation of triazolo-pyrimidine derivatives as novel inhibitors of hepatitis B virus surface antigen (HBsAg) secretion. J Med Chem 2011;54:5660-70. [PubMed]
266. Yuan HJ, Yuen MF, Ka-Ho Wong D, Sablon E, Lai CL. The relationship between HBV-DNA levels and cirrhosis-related complications in Chinese with chronic hepatitis B. J Viral Hepat 2005;12:373-9. [PubMed]
267. Yuen MF, Tanaka Y, Mizokami M, Yuen JC, Wong DK, Yuan HJ, Sum SM, Chan AO, Wong BC, and Lai CL. Role of hepatitis B virus genotypes Ba and C, core promoter and precore mutations on hepatocellular carcinoma: a case control study. Carcinogenesis 2004;25:1593-8. [PubMed]
268. Yuen MF, Yuan HJ, Wong DK, Yuen JC, Wong WM, Chan AO, Wong BC, Lai KC, Lai CL. Prognostic determinants for chronic hepatitis B in Asians: therapeutic implications. Gut 2005;54:1610-4. [PubMed]
269. Yuen MF, Fong DY, Wong DK, Yuen JC, Fung J, Lai CL. Hepatitis B virus DNA levels at week 4 of lamivudine treatment predict the 5-year ideal response. Hepatology 2007;46:1695-703. [PubMed]
270. Yuen MF, Wong DK, Fung J, Ip P, But D, Hung I, Lau K, Yuen JC, Lai CL. HBsAg Seroclearance in chronic hepatitis B in Asian patients: replicative level and risk of hepatocellular carcinoma. Gastroenterology 2008;135:1192-9. [PubMed]
271. Yuen MF, Tanaka Y, Fong DY, Fung J, Wong DK, Yuen JC, But DY, Chan AO, Wong BC, Mizokami M, Lai CL. Independent risk factors and predictive score for the development of hepatocellular carcinoma in chronic hepatitis B. J Hepatol 2009;50:80-8. [PubMed]
272. Yurdaydin C, Bozkaya H, Onder FO, Senturk H, Karaaslan H, Akdogan M, Cetinkaya H, Erden E, Erkan-Esin O, Yalcin K, Bozdayi AM, Schinazi RF, Gerin JL, Uzunalimoglu O, Ozden A. Treatment of chronic delta hepatitis with lamivudine vs lamivudine + interferon vs interferon. J Viral Hepat 2008;15:314-21. [PubMed]
273. Zeuzem S, Gane E, Liaw YF, Lim SG, DiBisceglie A, Buti M, Chutaputti A, Rasenack J, Hou J, O'Brien C, Nguyen TT, Jia J, Poynard T, Belanger B, Bao W, Naoumov NV. Baseline characteristics and early on-treatment response predict the outcomes of 2 years of telbivudine treatment of chronic hepatitis B. J Hepatol 2009;51:11-20. [PubMed]
274. Zhang BH, Yang BH, and Tang ZY. Randomized controlled trial of screening for hepatocellular carcinoma. J Cancer Res Clin Oncol 2004;130:417-22. [PubMed]
275. Zhang KY, Imazeki F, Fukai K, Arai M, Kanda T, Mikata R, Yokosuka O. Analysis of the complete hepatitis B virus genome in patients with genotype C chronic hepatitis and hepatocellular carcinoma. Cancer Sci 2007;98:1921-9. [PubMed]
276. Zhang W, Ke W, Wu SS, Gan L, Zhou R, Sun CY, Long QS, Jiang W, Xin HB. An adenovirus-delivered peptide aptamer C1-1 targeting the core protein of hepatitis B virus inhibits viral DNA replication and production in vitro and in vivo. Peptides 2009;30:1816-21. [PubMed]
277. Zoulim F, Carosi G, Greenbloom S, Mazur W, Nguyen T, Jeffers L, Brunetto M, Yu S, Llamoso C. Quantification of HBsAg in nucleos(t)ide-naive patients treated for chronic hepatitis B with entecavir with or without tenofovir in the BE-LOW study. J Hepatol 2014;Epub ahead of print. [PubMed]
Tables
Table 1: Guidelines for hepatocellular carcinoma surveillance in HBsAg carriers
Guideline |
Recommended surveillance population |
|---|---|
AASLD, 2010 (20) |
Africans and African Americans |
U.S. Algorithm, 2008 (107) |
Africans >20 years old |
WGO, 2010 (71) |
African males >20 years old |
APASL, 2010 (177) |
Cirrhosis |
Abbreviations: AASLD, American Association for the Study of Liver Diseases; ALT, alanine aminotransferase; APASL, Asia Pacific Association for the Study of the Liver; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; WGO, World Gastroenterology Association.
Table 2: Phases of chronic hepatitis B infection
| Phase of infection | Serum ALT | HBeAg | Anti-HBe | Serum HBV DNA | Liver Histology |
|---|---|---|---|---|---|
| Immune tolerance | Normal | Positive | Negative | Very high | Minimal to no activity |
| Immune clearance (HBeAg-positive) | Elevated | Positive | Negative | Variable; high or fluctuating | Significant activity |
| Inactive HBsAg carrier | Normal | Negative | Positive | Very low or undetectable | Minimal to no activity |
| Reactivation (HBeAg-negative) | Elevated, fluctuating | Negative | Positive | Variable; lower than HBeAg-positive infection | Significant activity |
Abbreviations: ALT, alanine aminotransferase; HBeAg, hepatitis B e antigen; Anti-HBe, antibody against hepatitis B e antigen; HBV, hepatitis B virus.
Table 3: Guidelines for initiation of antiviral therapy in chronic hepatitis B
|
EASL Guidelines (3) |
APASL Guidelines (133) |
AASLD Guidelines (148) |
U.S. Algorithm (107)* |
|---|---|---|---|---|
HBeAg-Positive |
HBV DNA >2,000 IU/mL and ALT >ULN |
HBV DNA >20,000 IU/mL and ALT >2x ULN |
HBV DNA >20,000 IU/mL and ALT >2x ULN |
HBV DNA ≥20,000 IU/mL and ALT >ULN |
HBeAg-Negative |
HBV DNA >2,000 IU/mL and ALT >ULN |
HBV DNA >2,000 IU/mL and ALT >2x ULN |
HBV DNA >20,000 IU/mL and ALT >2x ULN |
HBV DNA ≥2,000 IU/mL and ALT >ULN |
Cirrhosis |
Decompensated or compensated: Any detectable HBV DNA |
Decompensated: Any detectable HBV DNA |
Decompensated: Any detectable HBV DNA |
Decompensated: Any detectable HBV DNA |
Immunosuppression or Chemotherapy |
HBsAg-positive HBsAg-negative, anti-HBc-positive |
HBsAg positive HBsAg-negative, anti-HBc-positive |
HBsAg-positive |
HBsAg-positive |
Adapted from European Association for the Study of the Liver (3), Liaw et al. (133), Lok and McMahon (148), and Keeffe et al. (107).
*ULN of ALT in the U.S. Algorithm defined by 30 IU/mL in men and 19 IU/mL in women.
Abbreviations: AASLD, American Association for the Study of Liver Diseases; ALT, alanine aminotransferase; anti-HBc, antibody to hepatitis B core antigen; APASL, Asian Pacific Association for the Study of the Liver; EASL, European Association for the Study of the Liver; HBeAg, hepatitis B e antigen; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; ULN, upper limit of normal
Table 4: Serologic assessment of hepatitis B infection.
| Serologic marker | ||||
|---|---|---|---|---|
| HBsAg | Anti-HBs | Anti-HBc (IgM) | Total Anti-HBc | |
| Acute infection | + | – | + | + |
| Chronic infection | + | – | – | + |
| Resolved infection, immune | – | + | – | + |
| Previous vaccination, immune | – | + | – | – |
| Unexposed, susceptible | – | – | – | – |
Abbreviations: HBsAg, hepatitis B surface antigen; Anti-HBs, antibody against hepatitis B surface antigen; Anti-HBc, antibody against hepatitis B core antigen.
Table 5: Antiviral agents approved for treatment of chronic hepatitis B infection
| Antiviral agent | Drug class | Dose | Duration |
|---|---|---|---|
| Entecavir* | Nucleoside analogue | 0.5 mg daily | Variable |
| Tenofovir* | Nucleotide analogue | 300 mg daily | Variable |
| Lamivudine | Nucleoside analogue | 100 mg daily | Variable |
| Adefovir | Nucleotide analogue | 10 mg daily | Variable |
| Telbivudine | Nucleoside analogue | 600 mg daily | Variable |
| Interferon alfa-2b | Immune modulator | 5 million IU daily or 10 million IU three times weekly | 48 weeks |
| Pegylated interferon alfa* | Immune modulator | 1.5 mcg/kg weekly** (or) 180 mcg weekly*** | 48 weeks |
* Preferred agent
** Pegylated interferon alfa-2b is given at a dose of 1.5 mcg/kg weekly
*** Pegylated interferon alfa-2a is given at a dose of 180 mcg weekly
Table 6: Efficacy of antiviral therapy for HBeAg-positive chronic hepatitis B
| Antiviral Agent | HBV DNA negative | HBeAg loss | HBeAg seroconversion | HBsAg loss |
|---|---|---|---|---|
| Entecavir* | 67 | 22 | 21 | 2 |
| Tenofovir* | 76 | 22 | 21 | 3 |
| Pegylated Interferon Alfa* | 10-25 | 29-30 | 22-27 | 3-5 |
| Lamivudine | 36-44 | 17-32 | 16-21 | 0 |
| Adefovir | 13-21 | 24 | 12 | 0 |
| Telbivudine | 60 | 26 | 22-23 | 0 |
| Emtricitabine | 39 | 14 | 12 | 0 |
Data shown as percent patients based on achievement of virologic parameters at one year of therapy (63, 101, 121, 155)
*Preferred antiviral agents
Table 7: Efficacy of antiviral therapy for HBeAg-negative chronic hepatitis B
| Antiviral Agent | HBV DNA negative | HBsAg loss |
|---|---|---|
| Entecavir* | 90 | 0 |
| Tenofovir* | 93 | 0 |
| Pegylated Interferon Alfa* | 52-63 | 4 |
| Lamivudine | 60-73 | 0 |
| Adefovir | 51-64 | 0 |
| Telbivudine | 88 | 0 |
| Emtricitabine | 79 | 0 |
Data shown as percent patients based on achievement of virologic parameters at one year of therapy (63, 154, 155, 197)
*Preferred antiviral agents
Table 8: Management of drug resistance associated with hepatitis B therapy
Antiviral drug resistance |
Management |
|---|---|
Lamivudine
|
Continue lamivudine and add adefovir or tenofovir |
Adefovir |
Continue adefovir and add lamivudine or telbivudine |
Telbivudine |
Continue telbivudine and add adefovir or tenofovir |
Entecavir |
Switch to or add adefovir or tenofovir |
Adapted from Lok and McMahon (148), and Keeffe et al.(107).
Table 9: Hepatitis B vaccines
| Patient Group | Recombivax HB | Engerix-B | Twinrix*** | Pediarix**** |
|---|---|---|---|---|
| Children | 5mcg* | 10mcg | – | 10mcg |
| Adults (≥20 yrs) | 10mcg | 20mcg | 20mcg | – |
| Immunocompromised or dialysis patients | 40mcg | 40mcg** | – | – |
Adapted from Mast et al.(160) All hepatitis vaccines are administered as an intramuscular injection given in 3 doses at 0, 1, and 6 months, unless otherwise specified.
*Adolescents ages 10-15 yrs can receive an alternate regimen of 10mcg given in 2 doses at months 0 and 4-6.
**Dosing regimen of 40mcg given in 4 doses at months 0, 1, 2, and 6.
***Combined hepatitis A and hepatitis B vaccine. Approved for adults (>18 yrs). Alternate accelerated regimen involves 20mcg given in 4 doses at days 0, 7, 21 to 30, and at one year.
****Combined hepatitis B vaccine with diphtheria, tetanus, pertussis, and poliomyelitis vaccines; approved for ages 0-6 yrs given in 3 doses at 0, 2, and 4 months.
Table 10: Candidates for hepatitis B vaccination (2, 160)
Patient Group |
|---|
All infants within 24 hours of birth |
Abbreviations: HBV, hepatitis B virus; HIV, human immunodeficiency virus
What's New
Kubo A, et al. Prevention of vertical transmission of hepatitis B: An observational study. Ann Intern Med 2014;160:828-35
Woo G, et al. Tenofovir and Entecavir are the Most Effective Antiviral Agents for Chronic Hepatitis B: a Systematic Review and Bayesian Meta-Analyses. Gastroenterology. 2010 Oct;139:1218-29.
Hoa PT, Huy NT, et al. Randomized Controlled Study Investigating Viral Suppression and Serological Response Following Pre-S1/Pre-S2/S Vaccine Therapy Combined with Lamivudine Treatment in HBeAg-Positive Patients with Chronic Hepatitis B.Antimicrob Agents Chemother. 2009 Dec;53:5134-40.
Thompson ND, et al. Nonhospital Health Care-associated Hepatitis B and C Virus Transmission: United States, 1998-2008.Ann Intern Med. 2009. Jan 6;150(1):33-9.
FDA: FDA Approves First Nucleic Acid Test to Screen for Additional Types of HIV In Donated Blood and Tissues. December, 2008.http://www.fda.gov/bbs/topics/NEWS/2008/NEW01936.html
Carroll MB, Bond MI. Use of Tumor Necrosis Factor-alpha Inhibitors in Patients with Chronic Hepatitis B Infection. Semin Arthritis Rheum 2008 Jan 24 [Epub ahead of print].
Guided Medline Search For:
Reviews
Adhikari P, Mietzner T. Cell Mediated Immunity.
Hoffman C, Thio C. Clinical Implications of HIV and Hepatitis B Co-infection in Asia and Africa. The LANCET Infectious Diseases 2007; Vol.7, Issue 6, 402-409.
Keeffe EB, et al. A Treatment Algorithm for the Management of Chronic Hepatitis B Virus Infection in the United States: 2008 Update. Clin Gastroenterol Hepatol. 2008;6:1315-1341.
Lok ASF, McMahon BJ. Chronic Hepatitis B: Update 2009. AASLD Practice Guidelines. Hepatology 2009:50;1-36.
Sorrell MF, et al. National Institutes of Health Consensus Development Conference Statement: Management of Hepatitis B. Ann Intern Med 2009;150(2):104-10.
Guided Medline Search For Recent Reviews
Guided Medline Search For Historical Aspects
Table of Contents
- Virology
- Epidemiology
- Clinical Manifestations
- Laboratory Diagnosis
- Pathogenesis
- Susceptibility In Vitro and In Vivo
- Antiviral Therapy
- Adjunctive Therapy
- Endpoints for Monitoring Therapy
- Vaccines
- Prevention or Infection Control Measures
- Controversies, Caveats, or Comments