
Acute, Subacute and Chronic Cough in Adults
Authors: J. Mark Madison M.D. , Richard S. Irwin, M.D.
INTRODUCTION
The diagnostic and therapeutic approach to cough in adults has evolved significantly in the last decade and has recently been summarized in consensus guidelines (17,18). Because of the high success rates of therapies directed at specific underlying causes, nonspecific therapy for cough has only a limited role (3, 18). While the format of this article is similar to that of an article published in the New England Journal of Medicine in 2000, the content has been substantially updated (19).
CATEGORIZE COUGH BY DURATION
Determining the duration of the symptom is the first step in narrowing the differential diagnosis of cough. Cough is divided into three categories: acute, defined as lasting less than three weeks; subacute, lasting three to eight weeks; and chronic, lasting more than eight weeks (18). It is the duration of the cough at the time of presentation that is important in defining the spectrum of likely causes.
Evaluating the Patient with Acute Cough
The physician should perform a history and physical examination, considering the estimated frequency of conditions and looking for evidence of potentially life-threatening conditions known to cause cough. There have been no studies of the spectrum and frequency of causes of acute cough, but clinical experience suggests that the most common causes are upper respiratory tract infections such as the common cold, acute bacterial sinusitis, pertussis in some communities,exacerbations of chronic obstructive pulmonary disease, allergic rhinitis, and rhinitis due to environmental irritants (19, 43). However, acute cough also can be the presenting manifestation of infectious pneumonias, left ventricular failure, and diseases of the airways and lung parenchyma (e.g., hypersensitivity pneumonitis, aspiration) (17, 18, 54). It is important to consider and look for evidence of these potentially life-threatening or debilitating disorders in all patients who present with acute cough.
Viral infections of the upper respiratory tract are the most common causes of acute cough (43). Without treatment, the prevalence of cough due to the common cold ranges from 83 percent within the first 48 hours of the cold to 26 percent on day 14 (6). During the common cold, cough is due to stimulation of the cough reflex in the upper respiratory tract by upper airway secretions, clearing of the throat, or both (6). The common cold is diagnosed when patients present with an acute respiratory illness characterized by symptoms and signs related primarily to the nasal passages (e.g., rhinorrhea, sneezing, nasal obstruction, and postnasal drip), with or without fever, lacrimation, and irritation of the throat, and when a chest examination is normal. In such cases, and if the patient is immunocompetent, radiographic testing is not indicated, because it has a low yield (9).
For treating acute cough due to the common cold, there are medications that have been shown to be effective in some randomized, double-blind, placebo-controlled studies (Table 1). These include dexbrompheniramine plus pseudoephedrine (54) and naproxen (53). Although the effect on cough was not specifically assessed in a study that showed that intranasal ipratropium provided relief of rhinorrhea and sneezing due to the common cold (41), the drug may be helpful for patients who cannot take or tolerate the older-generation antihistamines or naproxen. There is no convincing evidence of efficacy for intranasal or systemic corticosteroids (12, 47), zinc lozenges (31, 34, 41) or non-sedating histamine H1 antagonists (17, 26).
The common cold is a viral rhinosinusitis that often cannot be distinguished clinically from bacterial sinusitis (13, 43, 55). Because viral rhinosinusitis is the much more common of the two during the first week of illness, it is recommended that antibiotics be prescribed when there are findings suggestive of acute sinusitis only if symptoms fail to show progressive improvement during the first week, if patients have at least two of the following signs and symptoms: a maxillary toothache, purulent nasal secretions, abnormal findings on transillumination of any sinus, and a history of discolored nasal discharge (Table 1), and/or if there is a biphasic course to the cough (i.e., cough worsens after initially improving). Imaging studies of the sinuses are usually not required in order to begin antibiotic therapy (56).
It is generally not recognized that the common cold can present as a syndrome of cough and phlegm (37, 51) and, consequently, physicians over diagnose bacterial bronchitis and over prescribe antibiotics (11). For acute cough, antibiotics are recommended when 1) the history and physical examination suggest acute bacterial pneumonia, 2) there is an exacerbation of chronic obstructive pulmonary disease, and 3) patients have had close contact with a known case of pertussis or have a cough-vomit syndrome suggestive of pertussis (17, 18) (Table 1).

Evaluating the Patient with Subacute Cough
When cough is subacute and not associated with an obvious respiratory infection, the evaluation of patients is similar to that for chronic cough (see below). For a cough that began with an upper respiratory tract infection and has lasted for three to eight weeks, the most common conditions to consider are postinfectious cough, bacterial sinusitis, and asthma (1, 18).
Postinfectious cough is a subacute cough that begins with an acute respiratory tract infection not complicated by pneumonia (i.e., the chest radiograph is normal) and then resolves without treatment (1,17, 18). The cough may be a consequence of upper airway irritation from inflammation, postnasal drip or clearing of the throat due to rhinitis, tracheobronchitis, or both, with or without transient bronchial hyperresponsiveness. If the patient reports postnasal drip, frequent clearing of the throat, or if mucus is seen in the oropharynx, initial treatment is similar to that for the common cold (Table 2). If the cough has not resolved after one week of this therapy, perform imaging studies of the sinuses to determine whether there is bacterial sinusitis as evidenced by mucosal thickening of more than 5 mm, air-fluid levels, or opacification. Treatment of bacterial sinusitis is a decongestant for five days, antibiotics for 2-3 weeks (Table 2), and then a reassessment of the patient (14).
Obtain a chest radiograph when a patient with subacute cough presents with wheezes, rhonchi, or crackles on physical examination. If it is normal, prescribe inhaled bronchodilators and corticosteroids and consider antibiotics only if there is suspicion of a recent B. pertussis infection. Improvement on bronchodilators and corticosteroids does not confirm a diagnosis of asthma because these drugs may alleviate cough by increasing mucociliary clearance, decreasing the production of mucus, or decreasing transient bronchial hyperresponsiveness after a viral infection. However, it is also true that cough may be the sole presenting manifestation of asthma (so-called cough variant asthma). This diagnosis is suggested by the presence of bronchial hyperresponsiveness (e.g., a positive methacholine inhalational challenge) and is confirmed only if the cough resolves during asthma therapy (Table 2) and follow-up is consistent with asthma (1,7, 18).
If B. pertussis infections have been reported in the community recently, if there is a history of contact with a patient who has a known case, or if the patient presents with the characteristic, but infrequently heard, whoop or with a cough-vomit syndrome, then empirical therapy for pertussis should be considered for any patient presenting with subacute cough (Tables 1 and 2) (1,17, 18). The later in the illness antibiotics are prescribed, the less likely the antibiotics are to be effective. The laboratory diagnosis of pertussis is difficult because there is often a delay between the onset of cough and the suspicion of the disease, there is no readily available, reliable serologic test for B. pertussis, and cultures of nasopharyngeal secretions are usually negative after two weeks of infection (57, 58).
Evaluating the Patient with Chronic Cough
Although cough that lasts longer than eight weeks can be caused by many different diseases, most cases are attributable to only a relatively few diagnoses (18,19, 30). Therefore, the management approach is to use focused laboratory testing (e.g., chest radiograph, methacholine inhalational challenge, or induced sputum to assess the airway inflammatory response), avoidance of drugs and irritants that cause cough, and empirical therapeutic trials aimed at the most common causes of chronic cough. If cough does not resolve completely, these initial evaluations and empirical treatments are followed by additional testing and consultation with a specialist or by referral to a cough clinic, if necessary. The definitive diagnosis of the cause of chronic cough is established only if specific therapy eliminates the cough. Because chronic cough can result simultaneously from more than one condition, partially successful therapy should not be stopped but should instead be sequentially supplemented (17, 18).
In approximately 95 percent of cases, chronic cough in the immunocompetent adult results from upper airway cough syndrome (UACS) caused by conditions of the nose and sinuses, asthma, gastroesophageal reflux disease (GERD), chronic bronchitis due to cigarette smoking or other irritants, bronchiectasis, non-asthmatic eosinophilic bronchitis (NAEB), or the use of an angiotensin-converting-enzyme inhibitor (ACEI) (4, 7, 16, 17, 18, 28, 37, 52, 35, 39). In the remaining 5 percent of cases, chronic cough results from other diseases, such as bronchogenic carcinoma, carcinomatosis, sarcoidosis, tuberculosis, left ventricular heart failure, and aspiration due to pharyngeal dysfunction. Psychogenic, or "habit", coughs are rare conditions that should only be diagnosed by exclusion (17, 18, 30, 29). Upper airway cough syndrome (UACS) with continual clearing of the throat is frequently misdiagnosed as a habit cough.
DIAGNOSIS
Clinical Evaluation
If the patient has a history of smoking or exposure to other environmental irritants or is currently being treated with an ACE inhibitors (7, 17, 18), the first step in management is to eliminate the irritant or discontinue the drug for four weeks. Cough due to these factors should improve or resolve within this interval (Table 3) (17, 18, 46).
Next, review the patient's history and physical examination and focus on the most common causes of chronic cough (i.e., UACS, asthma, and GERD). Obtain a chest radiograph and determine whether the symptoms conform to the clinical profile (see below) that is usually associated with a diagnosis of upper airway cough syndrome (UACS), asthma, gastroesophageal reflux disease (GERD), or non-asthmatic eosinophilic bronchitis (NAEB), alone or in combination. The character of the cough (e.g., paroxysmal, loose and self-propagating, productive, or dry), the quality of the sound (e.g., barking, honking, or brassy), and the timing of the cough (e.g., at night or with meals) have not been shown to be diagnostically useful (37). If the cough is productive of blood, the patient should be evaluated according to guidelines for hemoptysis (25, 27).
In evaluating patients with chronic cough, it is important to understand that the underlying cause of cough may be "silent" except for the cough itself. For example, although a history of postnasal drip or clearing of the throat and physical findings of mucus, a cobblestone appearance to the mucosa of the oropharynx, or both suggest UACS, these symptoms and signs are neither sensitive nor specific (28). A minority of patients may have no upper respiratory symptoms or signs yet may have a favorable response to combination therapy with a first-generation antihistamine H1 antagonist and a decongestant (so-called "silent" UACS) (7). Similarly, although frequent heartburn and regurgitation suggest that GERD is the cause of cough, these symptoms are absent in up to 75 percent of cases (so-called "silent" GERD) (23). Finally, cough can be the sole manifestation of asthma in up to 57 percent of cases (so-called cough variant asthma or "silent" asthma). Because a clinical diagnosis of asthma is unreliable even when there is wheezing, asthma should not be diagnosed on clinical grounds alone (24, 44). Always, a definitive diagnosis is made only if cough responds to specific therapy.
Imaging Studies
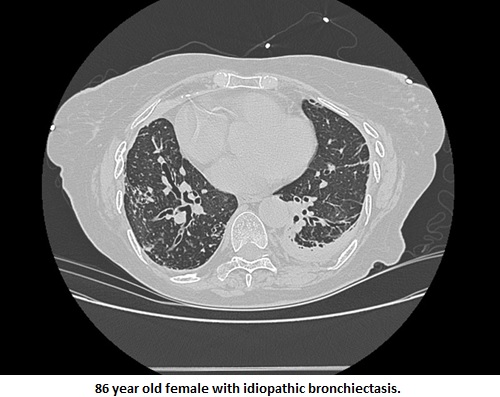
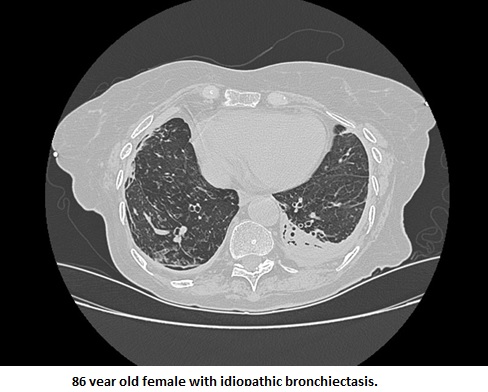
The chest radiograph is useful for the initial ranking of possible diagnoses and for guiding laboratory testing and trials of empirical therapies (17, 18). In an immunocompetent adult, a normal, or nearly normal, radiograph, makes UACS, asthma, GERD, and NAEB likely, but makes bronchogenic carcinoma, sarcoidosis, tuberculosis, and bronchiectasis ![]() unlikely. If the chest radiograph is abnormal, the physician should pursue those radiographic findings as potential, underlying causes of cough.
unlikely. If the chest radiograph is abnormal, the physician should pursue those radiographic findings as potential, underlying causes of cough.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
TREATMENT
Empirical Integrative Approach to Chronic Cough
The clinical profile of chronic cough associated with UACS, asthma, NAEB, GERD, or some combination of these conditions is that of a nonsmoking patient who is not taking an angiotensin-converting-enzyme inhibitor (ACEI) and has a stable and normal, or near-normal, chest radiograph (Table 3). When a patient fits this profile, the physician should proceed further using an empirical integrative approach to diagnosis and treatment (17, 18, 46). Empirical therapy should be directed first at the most common causes of cough in the community in which the clinician practices. In the United States, depending on the response to therapy at each step, empirical trials are directed at UACS, asthma/NAEB, and then GERD, in that order.
Upper Airway Cough Syndrome (UACS)
In the United States, a trial of empirical therapy focuses on UACS first because that diagnosis is the most common cause of chronic cough in adults in the United States (Table 3)(17, 18, 45). The differential diagnosis of UACS includes sinusitis and the following types of rhinitis, alone or in combination: nonallergic, allergic, postinfectious, vasomotor, drug-induced, and environmental irritant-induced. An empirical trial begins with a first-generation antihistamine-decongestant unless contraindicated by the presence of benign prostatic hypertrophy, hypertension, or glaucoma. Intranasal ipratropium bromide may also be effective. Because they do not have the anticholinergic effects of first-generation antihistamines, nonsedating antihistamines are not effective in this setting, unless the patient has allergic rhinitis or some other histamine-mediated rhinosinus condition. If the patient experiences resolution or partial resolution of cough in response to empiric therapy for UACS (noticeable improvement should occur within 2-4 days), then UACS is a cause, or contributing cause, of the cough and the antihistamine-decongestant is continued.
If empirical therapy is only partially effective and the patient still has nasal symptoms suggestive of rhinosinus disease, then consider the addition of a topical nasal steroid, nasal anticholinergic, or nasal antihistamine (45). Persistent UACS symptoms despite topical therapy are an indication for sinus imaging to look for evidence of occult sinusitis. The presence of air-fluid levels suggests that antibiotics for 2-3 weeks may be effective. Additional decongestant nasal spray with an alpha-adrenergic agonist (e.g., oxymetazoline hydrochloride for a maximum of 5 days) may be beneficial. If sinusitis fails to respond to treatment, a complete otolaryngologic evaluation is indicated and the physician should consider assessing for hypogammaglobulinemia, allergic hypersensitivity, or air-borne irritants in the home and work environment.
Asthma/Non-asthmatic eosinophilic bronchitis (NAEB)
Because a negative result of methacholine challenge rules out asthma as a cause of chronic cough (except early on after an exposure to toluene diisocyanate), many suggest that this test be routinely performed when considering asthma as a cause of chronic cough (17, 18). Although the positive predictive value of the test ranges from 60 to 88 percent, its negative predictive value is 100 percent (23, 28, 38, 52). Cough variant asthma should be treated the same way as asthma in general (17, 18). If a patient with chronic cough and a positive methacholine challenge test does not improve with standard asthma treatment (Table 3), the result of the methacholine challenge test can be considered to have been falsely positive. Alternatively, if the methacholine challenge test is positive and the patient responds, or partially responds, to empirical therapy for asthma using inhaled beta-adrenergic agonists and inhaled corticosteroids, then asthma is considered to have been a contributing cause of the chronic cough. On average, a chronic cough from asthma resolves after 67 days of treatment (8, 22). When treatment for asthma yields a partial response, concomitant conditions that make asthma difficult to control should be sought (e.g., sinusitis or GERD). If none are identified, adding an oral leukotriene inhibitor may be efficacious. If cough still does not respond, it is reasonable to give a 5-10 day trial of oral corticosteroids (e.g., 40 mg/day prednisone), provided the patient has no significant contraindications.
In patients with a negative bronchial provocation test, NAEB is suggested when examination of induced sputum shows eosinophilia (i.e., eosinophils constitute more than 3% of nonsquamous cells)(5, 10). If sputum examination is consistent with a diagnosis of NAEB, or if the test is unavailable, patients should have an empirical trial of inhaled corticosteroids. In most patients with NAEB, chronic cough resolves within 4 weeks of starting inhaled corticosteroids. A minority of patients may require a short course of oral corticosteroids. For all patients with NAEB, the possibility of occupational sensitizers and inhaled allergens as causes of NAEB should be considered and suspected exposures eliminated (5).
Gastroesophageal reflux disease (GERD)
If a patient has upper gastrointestinal symptoms consistent with GERD and chronic cough, the clinician should institute therapy for GERD by prescribing an antireflux diet, lifestyle modifications, and a proton pump inhibitor (20). If there is no response to this empirical therapy, a prokinetic agent should be added to the regimen.
In the absence of gastrointestinal symptoms, chronic cough is most likely to be due to GERD if the patient is a nonsmoker, is not taking an ACE inhibitor, has a normal or near-normal chest radiograph, and UACS, asthma, and NAEB each have been ruled out; 92% of patients with silent GERD fit this clinical profile (20, 21). Because 24 hour esophageal pH monitoring may not be available, and because interpretation of these results can be controversial, it is reasonable to begin an empirical trial of therapy for GERD without confirmatory testing when the patient fits the clinical profile for cough from GERD (17, 18, 20, 21, 28).
Confirmation of GERD as the cause of chronic cough requires that the cough disappear when the patient starts on antireflux therapy. Nevertheless, if treatment with proton pump inhibitors fails to eliminate cough in a patient who fits the clinical profile for GERD-induced chronic cough, GERD may nevertheless be causing the cough, but through a nonacid mechanism. Therefore, the term “acid reflux” can be misleading when describing chronic cough caused by GERD (20). Increasing evidence indicates that chronic cough can be caused by nonacid reflux as well as by acid reflux. Evidence is mounting that esophageal monitoring of pH and impedance rather than just monitoring pH is the best way of assessing for nonacid GERD.
Response to medical therapy is variable in cough from GERD, taking from less than 2 weeks to more than several months, and sometimes occurring only after a prokinetic agent is added. Some patients never respond to medical therapy. When medical therapy appears to be failing, the clinician should review patient adherence and consider whether a comorbid disease (e.g., obstructive sleep apnea) (32, 50) or drugs being used to treat a comorbid condition (e.g., progesterone, theophylline, nitrates, or calcium channel antagonists) may be exacerbating GERD. If cough still persists, perform 24-hour esophageal pH and impedance monitoring off of all medications, if it has not been done, to confirm an impression that GERD is potentially causing cough. It may be necessary to repeat the study while the patient is receiving the medical therapy for GERD to determine if therapy needs to be further intensified. In selected cases, upper gastrointestinal endoscopy or barium swallow testing may be indicated. On occasion, even maximal medical therapy will fail to alter pathologic reflux and, in such cases, patients should be evaluated for reflux surgery (17, 18, 20, 21).
COUGH THAT PERSISTS
Failure of the physician to avoid several common pitfalls often explains difficult to manage chronic cough (Table 4) (19,24). Once these potential errors in management have been addressed, additional laboratory studies (e.g., modified barium esophagography (51), 24-hour monitoring of esophageal pH and impedance, esophagoscopy, a study of gastric emptying with solids, high-resolution computed tomography of the chest (48), bronchoscopy (2, 22, 36, 49), or noninvasive cardiac studies) and referral to a cough specialist are indicated (18, 19, 42).
REFERENCES
1. Braman SS. Postinfectious cough. Chest 2006;129:138S-146S. [PubMed]
2. Brown KK. Chronic cough due to nonbronchiectatic suppurative airway disease (bronchiolitis). Chest 2006;129:132S-137S. [PubMed]
3. Bolser DC. Cough suppressant and pharmacologic protussive therapy. Chest 2006; 129: 238S-249S. [PubMed]
4. Brightling CE, Ward R, Goh KL, Wardlaw AJ, Pavord ID. Eosinophilic bronchitis is an important cause of chronic cough. Am J Respir Crit Care Med 1999;160:406-10. [PubMed]
5. Brightling CE. Chronic cough due to nonasthmatic eosinophilic bronchitis. Chest 2006;129:116S-121S. [PubMed]
6. Curley FJ, Irwin RS, Pratter MR, et al. Cough and the common cold. Am Rev Respir Dis 1988;138:305-11. [PubMed]
7. Dicpinigaitis PV. Angiotensin-converting enzyme inhibitor-induced cough. Chest 2006;129:169S-173S. [PubMed]
8. Dicpinigaitis PV. Chronic cough due to asthma. Chest 2006;129:75S-79S. [PubMed]
9. Diehr P, Wood RW, Bushyhead JB, Krueger L, Wolcott B, Tompkins RK. Prediction of pneumonia in outpatients with acute cough-- a statistical approach. J Chronic Dis 1984;37:215-25. [PubMed]
10. Gibson PG, Dolovich J, Denburg J, Ramsdale EH, Hargreave FE. Chronic cough: eosinophilic bronchitis without asthma. Lancet 1989;1: 1346-8. [PubMed]
11. Gonzales R, Steiner JF, Sande MA. Antibiotic prescribing for adults with colds, upper respiratory tract infections, and bronchitis by ambulatory care physicians. JAMA 1997;278:901-4. [PubMed]
12. Gustafson LM, Proud D, Hendley JO, Hayden FG, Gwaltney JM Jr. Oral prednisone therapy in experimental rhinovirus infections. J Allergy Clin Immunol 1996;97:1009-14. [PubMed]
13. Gwaltney JM Jr, Phillips CD, Miller RD, Riker DK. Computed tomographic study of the common cold. N Engl J Med 1994;330:25-30. [PubMed]
14. Hamory BH, Sande MA, Sydnor A Jr, Seale DL, Gwaltney JM Jr. Etiology and antimicrobial therapy of acute maxillary sinusitis. J Infect Dis 1979;139:197-202. [PubMed]
15. Hayden FG, Diamond L, Wood PB, Korts DC, Wecker MT. Effectiveness and safety of intranasal ipratropium bromide in common colds: a randomized, double-blind, placebo-controlled trial. Ann Intern Med 1996; 125:89-97. [PubMed]
16. Hoffstein V. Persistent cough in nonsmokers. Can Respir J 1994;1:40-7.
17. Irwin RS, Boulet L-P, Cloutier MM, et al. Managing cough as a defense mechanism and as a symptom: a consensus panel report of the American College of Chest Physicians. Chest 1998;114:Suppl:133S-181S. [PubMed]
18. Irwin RS, Baumann MH, Bolser DC, et al. Diagnosis and management of cough executive summary: ACCP evidence-based clinical practice guidelines. Chest 2006; 129: 1S-23S. [PubMed]
19. Irwin RS, Madison JM. The diagnosis and treatment of cough. N Engl J Med 2000; 343:1715-1721. [PubMed]
20. Irwin RS. Chronic cough due to gastroesopageal reflux disease. Chest 2006;129:80S-94S. [PubMed]
21. Irwin RS, Zawacki JK. Accurately diagnosing and successfully treating chronic cough due to gastroesophageal reflux disease can be difficult. Am J Gastroenterol 1999;94:3095-8. [PubMed]
22. Irwin RS, French CL, Smyrnios NA, Curley FJ. Interpretation of positive results of a methacholine inhalation challenge and 1 week of inhaled bronchodilator use in diagnosing and treating cough-variant asthma. Arch Intern Med 1997;157:1981-7.[PubMed]
23. Irwin RS, French CL, Curley FJ, Zawacki JK, Bennett FM. Chronic cough due to gastroesophageal reflux: clinical, diagnostic, and pathogenetic aspects. Chest 1993;104:1511-7. [PubMed]
24. Irwin RS, Corrao WM, Pratter MR. Chronic persistent cough in the adult: the spectrum and frequency of causes and successful outcome of specific therapy. Am Rev Respir Dis 1981;123:413-7. [PubMed]
25. Irwin RS, Curley FJ, Robinson KA. Managing Hemoptysis. In Intensive Care Medicine, sixth edition, edited by RS Irwin and JM Rippe. Lippincott Williams and Wilkins, Philadelphia, 2008, pp. 588-598.
26. Irwin RS, Curley FJ, Bennett FM. Appropriate use of antitussives and protussives: a practical review. Drugs 1993;46:80-91. [PubMed]
27. Irwin RS. Symptoms of Respiratory Disease. In ACCP Pulmonary Board Review: Course Syllabus, 2007. American College of Chest Physicians, Northbrook, IL, 2007, pp. 397-436.
28. Irwin RS, Curley FJ, French CL. Chronic cough: the spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Am Rev Respir Dis 1990;141:640-7. [PubMed]
29. Irwin RS, Glomb WB, Chang AB. Habit cough. Chest 2006;129:174S-179S. [PubMed]
30. Irwin RS. Cough. In: Irwin RS, Curley FJ, Grossman RF, eds. Diagnosis and treatment of symptoms of the respiratory tract. Armonk, N.Y.: Futura Publishing, 1997:1-54.
31. Jackson JL, Peterson C, Lesho E. A meta-analysis of zinc salts lozenges and the common cold. Arch Intern Med 1997;157:2373-6. [PubMed]
32. Kerr P, Shoenut JP, Millar T, Buckle P, Kryger MH. Nasal CPAP reduces gastroesophageal reflux in obstructive sleep apnea syndrome. Chest 1992;101:1539-44. [PubMed]
33. Kvale PA. Chronic cough due to lung tumors. Chest 2006;129:147S153S. [PubMed]
34. Macknin ML, Piedmonte M, Calendine C, Janosky J, Wald E. Zinc gluconate lozenges for treating the common cold in children: a randomized controlled trial. JAMA 1998;279:1962-7. [PubMed]
35. Marchesani F, Cecarini L, Pela R, Sanguinetti CM. Causes of chronic persistent cough in adult patients: the results of a systematic management protocol. Monaldi Arch Chest Dis 1998;53:510-4. [PubMed]
36. Markowitz DH, Irwin RS. Is bronchoscopy overused in the evaluation of chronic cough? Bronchoscopy is overused. J Bronchol 1997;4:332-6.
37. Mello CJ, Irwin RS, Curley FJ. Predictive values of the character, timing, and complications of chronic cough in diagnosing its cause. Arch Intern Med 1996;156:997-1003. [PubMed]
38. McGarvey LPA, Heaney LG, Lawson JT, et al. Evaluation and outcome of patients with chronic non-productive cough using a comprehensive diagnostic protocol. Thorax 1998;53:738-43. [PubMed]
39. Palombini BC, Villanova AC, Araujo E, et al. A pathogenic triad in chronic cough: asthma, postnasal drip syndrome, and gastroesophageal reflux disease. Chest 1999;116:279-84. [PubMed]
40. Prakash UBS. Uncommon causes of cough. Chest 2006; 129: 206S-219S.
41. Prasad AS, Fitzgerald JT, Bao B, Beck FW, Chandrasekar PH. Duration of symptoms and plasma cytokine levels in patients with the common cold treated with zinc acetate. Ann Intern Med 2000;133:245-52. [PubMed]
42. Pratter MR. Unexplained (idiopathic) cough. Chest 2006;129:220S-221S. [PubMed]
43. Pratter MR. Cough and the common cold. Chest 2006; 129: 72S-74S. [PubMed]
44. Pratter MR, Hingston DM, Irwin RS. Diagnosis of bronchial asthma by clinical evaluation: an unreliable method. Chest 1983;84:42-7. [PubMed]
45. Pratter MR. Chronic upper airway cough syndrome secondary to rhinosinus diseases (previously referred to as postnasal drip syndrome). Chest 2006;129:63S-71S. [PubMed]
46. Pratter MR, Brightling CE, Boulet LP, Irwin RS. An empiric integrative approach to the management of cough. Chest 2006;129:222S-231S. [PubMed]
47. Puhakka T, Makela MJ, Malmstrom K, et al. The common cold: effects of intranasal fluticasone propionate treatment. J Allergy Clin Immunol 1998;101:726-31. [PubMed]
48. Rosen MJ. Chronic cough due to bronchiectasis. Chest 2006; 129:122S-131S. [PubMed]
49. Schaefer OP, Irwin RS. Chronic cough due to clinically "silent" suppurative disease of the airways: a new clinical entity. Am J Respir Crit Care Med 1999;159:Suppl:A830.
50. Shoenut JP, Kerr P, Micflikier AB, Yamashiro Y, Kryger MH. The effect of nasal CPAP on nocturnal reflux in patients with aperistaltic esophagus. Chest 1994;106:738-41. [PubMed]
51. Smith Hammond CA, Goldstein LB. Cough and aspiration of food and liquids due to oral-pharyngeal dysphagia. Chest 2006;129:154S-168S. [PubMed]
52. Smyrnios NA, Irwin RS, Curley FJ. Chronic cough with a history of excessive sputum production: the spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Chest 1995;108:991-7.[PubMed]
53. Sperber SJ, Hendley JO, Hayden FG, Riker DK, Sorrentino JV, Gwaltney JM Jr. Effects of naproxen on experimental rhinovirus colds: a randomized, double-blind, controlled trial. Ann Intern Med 1992;117:37-41. [PubMed]
54. Teramoto S, Matsuse T, Ouchi Y. Clinical significance of cough as a defense mechanism or a symptom in elderly patients with aspiration and diffuse aspiration bronchiolitis. Chest 1999;115:602-3. [PubMed]
55. van Buchem FL, Knottnerus JA, Schrijnemaekers VJJ, Peeters MF. Primary-care-based randomised placebo-controlled trial of antibiotic treatment in acute maxillary sinusitis. Lancet 1997;349:683-7. [PubMed]
56. Williams JW Jr, Simel DL, Roberts L, Samsa GP. Clinical evaluation for sinusitis: making the diagnosis by history and physical examination. Ann Intern Med 1992;117:705-10. [PubMed]
57. Wright SW, Edwards KM, Decker MD, Zeldin MH. Pertussis infection in adults with persistent cough. JAMA 1995;273:1044-6. [PubMed]
58. Yaari E, Yafe-Zimerman Y, Schwartz SB, et al. Clinical manifestations of Bordetella pertussis infection in immunized children and young adults. Chest 1999;115:1254-8. [PubMed]
Tables
Table 1. Treating Common Causes of Acute Cough in Adults.*
| Cause of cough | Treatment | Comments |
|---|---|---|
| Common cold |
|
|
|
|
|
Allergic rhinitis |
|
|
Exacerbation of COPD |
|
|
|
|
|
|
* When supported by double-blind, randomized, placebo-controlled studies, specific drugs and doses are shown. COPD denotes chronic obstructive pulmonary disease. CHF denotes congestive heart failure. NSAIDs denote non-steroidal anti-inflammatory drugs. PaO2 denotes partial pressure of arterial oxygen. Table modified from reference 19.
Table 2. Treating Common Causes of Subacute Cough in Adults.*
| Cause of cough | Treatment | Comments |
|---|---|---|
| Postinfectious |
|
|
|
|
|
Asthma |
|
|
|
|
*When supported by double-blind, randomized, placebo-controlled studies, specific drugs and doses are shown. UACS denotes upper airway cough syndrome. Table modified from reference 19.
Table 3. Treating Common Causes of Chronic Cough in Adults.*
| Cause of cough | Treatment | Comments |
|---|---|---|
| Chronic bronchitis |
|
|
Angiotensin-converting-enzyme inhibitor |
|
|
Upper airway cough syndrome (UACS) |
||
| Nonallergic rhinitis |
|
|
| Allergic rhinitis |
|
|
| Vasomotor rhinitis |
|
|
| Chronic bacterial sinusitis |
|
|
Asthma |
|
|
Non-asthmatic eosinophilic bronchitis (NAEB)
|
|
|
| Gastroesophageal reflux disease (GERD) |
|
|
*Specific drugs and doses are mentioned when their use is supported by double-blind, randomized, placebo-controlled studies. Table modified from reference 19.
Table 4. Common Difficulties Encountered When Managing Causes of Chronic Cough.
| Cause | Difficulty |
|---|---|
Upper airway cough syndrome (UACS) |
o Failure to recognize that it can present as a syndrome of cough and phlegm. o Assumption that all H1 antagonists are the same. o Failure to consider sinusitis because it is not obvious. o Failure to consider allergic rhinitis because symptoms are perennial. |
Asthma |
o Failure to recognize that it can present as a syndrome of cough and phlegm. o Failure to recognize that inhaled medications may exacerbate cough. o Assumption that a positive methacholine challenge test alone is diagnostic of asthma. |
Gastroesophageal reflux disease (GERD) |
o Failure to recognize that it can present as a syndrome of cough and phlegm. o Failure to recognize that "silent" reflux disease can cause of cough and that it may take 2-3 months of medical therapy before cough starts to improve and, on average, 5-6 months before cough resolves. o Assumption that cough cannot be due to gastroesophageal reflux disease because cough remains unchanged when gastrointestinal symptoms improve. o Failure to recognize that cough may fail to improve with the most intensive medical therapy and that the adequacy of therapy and the need for surgery can be assessed by means of 24-hour monitoring of esophageal pH and impedance. o Failure to recognize the effects of coexisting diseases (e.g., sleep apnea or coronary artery disease) or their treatment (e.g., nitrates). o Failure to treat coexisting causes of cough that perpetuate the cycle of cough and reflux. |
UACS, asthma, GERD |
o Failure to recognize that the typical profile for a patient with UACS, asthma, GERD is that of a nonsmoking patient who is not taking an ACEI and has stable and normal, or near-normal, chest radiograph. o Failure to consider that more than one of these conditions may be contributing simultaneously to cough. o Failure to consider these common conditions because of a seemingly more "obvious" cause (e.g., chronic interstitial pneumonia). |
* Table modified from reference 4. Angiotensin-converting-enzyme inhibitor (ACEI) denotes angiotensin converting enzyme inhibitor.