|
|
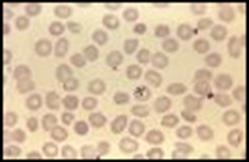
Figure 2

Figure 3
Figure 4
Figure 5
Table 1: Causes of Functional Asplenia
Congenital
Asplenia
Cyanotic heart disease
Hematological
Sickle-cell disorders
Essential thrombocytopenia
Hodgkin’s lymphoma
Non-Hodgkin’s lymphoma
Fanconi’s syndrome
Autoimmune
Systemic lupus erythematosus
Mixed connective tissue disease
Rheumatoid arthritis
Sjögren’s syndrome
Gastrointestinal
Celiac disease
Ulcerative colitis
Crohn’s disease
Tropical sprue
Whipple’s disease
Alcoholic liver disease
Circulatory compromise of the spleen
Miscellaneous
Irradiation
Amyloidosis
Sarcoidosis
AIDS
Allogeneic Bone Marrow Transplantation
Long-term intravenous nutrition
Selective IgA deficiency
|
Table 2: Pathogens associated with OPSI |
|
|
|
Definite Capnocytophaga canis (Dysgonic fermenter 2 [DF2]) Babesia microtis (cattle malaria) Plasmodia spp. (malaria)
|
|
Possible Haemophilus influenzae type b (Hib) Salmonella species |
|
|
|
Unlikely |
|
Table 3: Differential Diagnosis
|
|
Sepsis (infection) with severe sepsis/septic shock |
|
Painful crisis (sickle cell disease) |
|
Acute chest pain syndrome (sickle cell disease) |
|
Pneumonia (without severe sepsis/septic shock) |
|
Malignancies (lymphoma, leukemia and others) |
|
Infarction of lung and other cardiopulmonary compromise |
|
Collagen-vascular disorders |
|
Drug-associated fever |
|
Table 4: Clinical Manifestations |
|
Fever with rigors |
|
Arthralgias and myalgias |
|
Gastrointestinal symptoms (upper and lower GI tracts) |
|
Cardiovascular collapse |
|
Disseminated intravascular coagulopathy |
|
Seizures |
|
Coma |
|
Gangrene (Purpura fulminans) |
Table 5: Laboratory and Radiological Investigations
|
Routine |
|
|
|
|
|
|
|
Complete chemistry profile |
|
|
|
Complete blood count and differential |
|
|
|
Coagulation assays |
|
|
|
Arterial blood gases |
|
|
|
Peripheral smear |
|
|
|
Fibrin, fibrin split products |
|
|
|
Cortisol level |
Cosyntropin stimulation test, if required |
|
|
At least two sets, two separate sites |
|
|
|
Urinalysis |
Urine culture, if indicated |
|
|
Sputum specimen |
Culture and Gram’s stain |
|
|
Cerebrospinal fluid |
Cell count, protein, glucose |
Gram’s stain, culture |
|
S. pneumoniae urine antigen |
|
|
|
|
|
|
|
Specialized |
|
|
|
|
|
|
|
Buffy coat |
if neutropenic |
|
|
Plasmodia spp. |
Thin blood smear |
ParaSight F and OptiMal rapid assays |
|
Thin blood smear |
IgG IFA assay (CDC) |
|
|
|
|
|
|
Radiology |
|
|
|
|
|
|
|
Chest radiography |
|
|
|
Ultrasonography |
As indicated by clinical or laboratory findings |
|
|
CT and MRI scans |
As indicated by clinical or laboratory findings |
|
|
Nuclear scans |
As indicated by clinical or laboratory findings |
|
Table 6a: Empiric Antibiotic Therapy, Adults
|
Antibiotic (trade) |
Usual dosage |
Meningitis dosage |
Renal adjustment
|
|
Cefotaxime (Claforan) |
1-2 gr IV every 8 hrs |
2 gr IV every 4-6 hrs |
Increase interval to 12-24 hrs |
|
Ceftriaxone (Rocephin)
|
1 gr IV once daily |
2 gr IV every 12 hrs |
Not applicable |
|
|
1 gr IV every 12 hrs, Pharmacokinetics recommended |
Same; pharmacokinetics recommended |
Reduction required; antibiotic levels require monitoring |
|
Ciprofloxacin (Cipro) |
400 mg IV every 12 hrs or 500-750 mg PO every 12 hrs
|
400 mg IV every 12 hrs or 750 mg PO every 12 hrs |
50% reduction |
|
Levofloxacin (Levaquin) |
750 mg IV/PO daily |
Same |
750 mg IV/PO once, then 500 mg IV/PO every 48 hrs
|
|
Moxifloxacin (Avelox) |
400 mg IV/PO every 24 hours |
Same |
Clinical data lacking for CNS infections
|
|
|
|
|
|
|
Imipenem (Primaxin) |
500 mg IV every 6 hrs |
Same |
125-250 mg IV every 12 hrs; beware of inducing seizures if dosage is exceeded
|
|
Meropenem (Merrem) |
1 gr IV every 8 hrs |
Same |
0.5-1 gr IV every 12-24 hrs |
Table 6b: Empiric Antibiotics Therapy, Pediatric
|
Antibiotic (trade name) |
Usual dosage |
Meningitis dosage
|
|
Cefotaxime (Claforan) |
50 mg/kg IV every 8 hrs |
75 mg/kg IV every 6 hrs
|
|
Ceftriaxone (Rocephin) |
50 mg/kg IV every 24 hrs |
100 mg/kg IV every 24 hrs
|
|
Imipenem (Primaxin) |
15-25 mg/kg every 6 hrs (maximum dosage 2-4 gr/day)
|
Not recommended due to seizure potential |
|
Meropenem (Merrem) |
60-120 mg/kg IV divided every 8 hrs |
120 mg/kg IV divided every 8 hrs
|
|
Rifampin (Rifadin) |
10 mg/kg PO/IV daily |
Same |
|
40 mg/kg IV divided every 6-8 hrs |
60 mg/kg IV divided every 6-8 hrs
|
|
|
Fluoroquinolones |
not approved for this population, in this setting |
not approved for this population, in this setting
|
Table 7a: Organism-Directed Antibiotic Therapy
|
Organism |
Recommended Antibiotic(s)
|
Alternative(s) |
Comment(s) |
|
|
|
|
|
|
Penicillin (PCN) MIC<0.1 mg/L |
PCN G or ampicillin |
|
|
|
|
|
|
|
|
PCN MIC 0.1-1.0 mg/L |
cefotaxime or ceftriaxone |
|
|
|
|
|
|
|
|
PCN MIC ≥2.0mg/L |
vancomycin plus ceftriaxone/cefotaxime (plus rifampin if dexamethasone is used) |
Regimen for meningitis; clinical data unavailable for fluoroquinolones
|
|
|
Cefotaxime or ceftriaxone MIC ≥1.0mg/L |
vancomycin plus ceftriaxone/cefotaxime ± rifampin |
moxifloxacin, levofloxacin |
Regimen for meningitis; clinical data unavailable for fluoroquinolones |
|
|
|
|
|
|
H. influenzae (type b and others) |
|
|
|
|
Beta-lactamase negative |
ampicillin |
cefotaxime, ceftriaxone, cefepime, chloramphenicol, moxifloxacin, levofloxacin, ciprofloxacin
|
|
|
Beta-lactamase positive |
ceftriaxone, cefotaxime |
cefepime, chloramphenicol, moxifloxacin, levofloxacin, ciprofloxacin |
|
|
|
|
|
|
|
|
|
|
|
|
PCN MIC <0.1 mg/L |
PCN G or ampicillin |
ceftriaxone, cefotaxime, chloramphenicol |
|
|
|
|
|
|
|
PCN MIC 0.1-1.0 mg/L |
ceftriaxone, cefotaxime |
Chloramphenicol, moxifloxacin, levofloxacin, ciprofloxacin, meropenem |
|
|
|
|
|
|
|
Salmonella species |
Ceftriaxone, cefotaxime, ciprofloxacin, levofloxacin |
Use ampicillin only once sensitivities are known. Meropenem is preferred agent for CNS infections |
|
|
|
|
|
|
|
Imipenem, ertapenem, meropenem, clindamycin, rifampin, doxycycline, erythromycin, vancomycin, cefotaxime, ceftriaxone, ciprofloxacin, levofloxacin |
Resistant to aztreonam. |
||
|
|
|
|
|
|
imipenem, carbapenem, ciprofloxacin, levofloxacin |
|
Beta-lactams are not advised. |
|
|
|
|
|
|
|
Atovaquone plus azithromycin |
Clindamycin plus oral quinine |
For dosages, see table 7b. |
|
|
|
|
|
|
|
Plasmodia spp. |
www.cdc.gov/ncdidod/dpd/parasites/malaria/default/htm
|
|
|
|
Severe, non-pregnant |
quinidine gluconate plus doxycycline or clindamycin |
and primaquine (for non-falciparum spp.)
|
For dosages, see table 7b. |
|
Pregnant, not severe |
quinine sulfate plus clindamycin |
Quinine sulfate plus doxycycline (if preferred regimen failing) |
primaquine, if necessary, after delivery to treat non-falciparum; avoid mefloquine; for dosages, see table 7b. |
Table 7b: Usual Dosages of Antibiotics
|
Antibiotic (trade name)
|
Adult dosage |
Pediatric dosage |
Renal adjustment |
Comments |
|
Amoxicillin-clavulanate (Augmentin) |
500/125-875/125 mg PO twice daily with food OR 1000/62.5 2 tabs PO twice daily with food [Augmentin XR] |
25-50 mg/kg PO divided every 8 hrs OR 600/42.9/5 ml 90 mg/kg divided PO every 12 hrs with food [ES-600] |
Reduce frequency to once or twice per day. Augmentin XR contraindicated with CrCl <30.
|
|
|
2 gr IV every 4-6 hrs |
50 mg/kg IV every 6 hours |
Reduce to every 8 to 24 hrs
|
|
|
|
Ampicillin-sulbactam (Unasyn) |
3 gr IV every 6 hrs |
100-300 mg/kg every 6 hrs |
Reduce to every 8-24 hrs
|
|
|
Atovaquone (Mepron) |
750 mg (5 ml) PO twice daily for 7-10 days |
|
|
Tx for Babesiosis
|
|
Azithromycin (Zithromax) |
600 mg PO daily for 7-10 days |
|
|
Tx for Babesiosis
|
|
Cefepime (Maxipime) |
2 gr IV every 8-12 hrs |
150 mg/kg IV div every 8 hrs |
Reduce frequency to 12-24 hrs
|
|
|
50-100 mg/kg IV div every 6 hrs |
12.5-50 mg/kg IV every 6 hrs (2-4 gr max) |
Not applicable |
|
|
|
Clindamycin (Cleocin) |
1.2 gr IV every 12 hr hrs for 7-10 days |
25 mg/kg IV every 12 hrs for 7-10 days |
Not applicable |
Tx for Babesiosis
|
|
Doxycycline (Vibramycin) |
100 mg PO/IV every 12 hrs |
2-4 mg/kg PO/IV div every 12 hrs (max 200 mg per day); avoid in children less than 8 y/o |
Not applicable |
|
|
Ertapenem (Invanz) |
1 gr IV daily |
30 mg/kg IV div every 12 hrs |
Decrease amount by 50% |
|
|
250-500 mg PO every 6 hrs |
10 mg/kg IV/PO every 6 hrs |
Not applicable |
|
|
|
4 million units IV every 4 hrs |
250,000-400,000 units/kg IV div every 4-6 hrs |
Adults: decrease frequency to 8-12 hrs Peds: decrease dose 25-50% |
|
|
|
30 mg PO daily for 14 days |
0.6 mg/kg daily for 14 days |
Not applicable |
Check G6PD level
|
|
|
Quinine (oral) |
650 mg PO every 6-8 hrs for 7-10 days |
25 mg/kg PO div every 6-8 hrs for 7-10 days |
|
Tx for Babesiosis and Plasmodia spp.
|
|
Quinidine gluconate |
10 mg/kg (salt) IV in NS over 1 hr, then 0.02 mg/kg IV continuous |
Same as adult |
Change to quinine sulfate when <1% parasite load |
|
|
Quinine sulfate |
648 mg po every 8 hrs for 3-7 days |
30 mg/kg PO div every 8 hrs for 3-7 days |
Load 648 mg, then 324 mg every 12 hrs |
|
Table 8: Recommended Vaccines
|
Vaccine |
Adult |
Pediatric |
Booster |
Comment |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pneumococcal conjugate vaccine (PCV-7) (Prevnar) |
See PPV |
Age ≤23 months: 4 doses at 2, 4, 6 and 12-15 months (0.5 ml IM thigh or deltoid) |
PPV-23 at age ≥ 2 y/o Give ≥2 mos after last PCV; 0.5 ml IM/SC; repeat 3-5 yrs later
|
PCV not for use in children >59 months old |
|
Pneumococcal polysaccharide vaccine (PPV-23) (Pneumovax) |
0.5 ml IM/SC |
See PCV |
Repeat ≥5 yrs If age ≥65 and ≥5 yrs since last dose |
Only two doses in lifetime are recommended |
|
|
|
|
|
|
|
|
|
|
Hib/DTaP (TriHIBit) and Hib/HepB (COMVAX) are also available
|
|
|
PRP-OMP (PedvaxHIB) |
0.5 ml IM |
Two doses two months apart beginning at 2 months old (0.5 ml IM) |
Age 12-15 months (may use TriHIBit also) (0.5 ml IM) |
No clinical data for adults, but appears well tolerated; only one dose is recommended
|
|
HbOC (HibTITER), PRP-T (ActHIB), |
0.5 ml IM |
6 weeks to 71 months: Three doses two months apart beginning at 2 months old (0.5 ml IM)
|
Age 12-15 months (may use TriHIBit also) (0.5 ml IM) |
No clinical data for adults, but appears well tolerated; only one dose is recommended |
|
|
|
|
|
|
|
|
|
|
CDC continues to recommend; please see comments in text.
|
|
|
Quadravalent polysaccharide vaccine (MPS4) (Meromune) |
0.5 ml SC |
Age ≥ 2 years; 0.5 ml SC |
Provides protection for 3-5 yrs ; revaccinate for high risk situations
|
Covers A,C, Y and W-135 |
|
Quadrivalent conjugate vaccine (MCV4) (Menactra)
|
Ages 11-55 ; 0.5 ml IM deltoid |
Age ≥ 1 ; 0.5 ml IM deltoid |
Unknown |
Covers A,C, Y and W-135 |
|
Monovalent MC type B |
|
|
|
Not available in United States |
|
|
|
|
|
|
|
|
|
|
|
|
|
Injectable (Fluvirin, Fluzone, Fluarix) |
0.5 ml IM deltoid |
Ages 6 months-8 yrs: 2 injections at least 4 weeks apart for first time recipients; ages 6-35 months: 0.25 ml IM, ant-lat thigh Ages 3-8 yrs: 0.5 ml IM ant-lat thigh or deltoid (older children) |
Yearly |
Fluvirin approved for ≥5 yrs; Fluarix approved for ≥18; optimally administer October- November |
|
Intranasal (LAIV) (Flumist) |
Age ≥ 12 years but ≤ 49 years: 0.5 ml intranasal |
Ages 5-8: two doses 0.5 ml intranasal 6-10 weeks apart; if first dose was injectable, wait 4 weeks. Ages ≥9 years: 0.5 ml intranasal |
Yearly |
Avoid in pts severely immuno- compromised or in those who will be exposed to severely immuno- compromised |
Table 9: Prevention
|
Immunization: S. pneumoniae, Influenza virus, Hib; possibly N. meningitidis |
|
Tick, mosquito and animal bite prevention |
|
Oral antibiotic prophylaxis |
|
Availability of medical and contact information, i.e, medical bracelet |
|
Early intervention with appropriate support and antibiotics |
Figure 1