
Thrombocytopenia - Diagnosis and Management
Clinical Manifestations
There is no strong correlation between the severity of bleeding and the number
of platelets. Multiple factors play a role. A patient with immune
thrombocytopenic purpura may not bleed even if the platelet count is < 10,000/mcl
due to very functional platelets. On the other hand, a patient with mild
thrombocytopenia may develop significant bleeding if he/she is on medications
like heparin, aspirin or pentoxyfilline. Renal failure sepsis, coagulopathy from
any cause can be contributory as well. The common clinical presentations of
thrombocytopenia are listed in Table 5. Serious bleeding such as spontaneous
intracranial bleeding is very rare unless the platelet count is less than
10,000/mcL
Table 5. Common clinical
presentations of thrombocytopenia
|
Petichial hemorrhages |
|
Echymoses or bruising |
|
Wet purpura, bleeding from mucus membranes of the mouth |
|
Bleeding from nose, gums, hematuria, or heavy menstrual
flow in females, etc. |
Diagnosis
Step 1:
Review complete blood count (CBC) carefully. High mean platelet volume or
mean platelet volume
(MPV)
(like mean corpuscular volume (MCV) for red blood cells) indicates large platelets, which occurs in pseudo
thrombocytopenia, peripheral destruction of platelets or splenic sequestration.
Isolated thrombocytopenia is usually a sign of immune thrombocytopenic purpura.
Presence of simultaneous leucopenia and anemia indicate a generalized process
such as bone marrow problems, cyanocobalmine or folate deficiency or
hypersplenism. High MCV may suggest B12 or folate deficiency, alcohol abuse, or
myelodysplastic syndromes. High white blood cell count or blasts may be present
in acute or chronic leukemia.
Step 2:
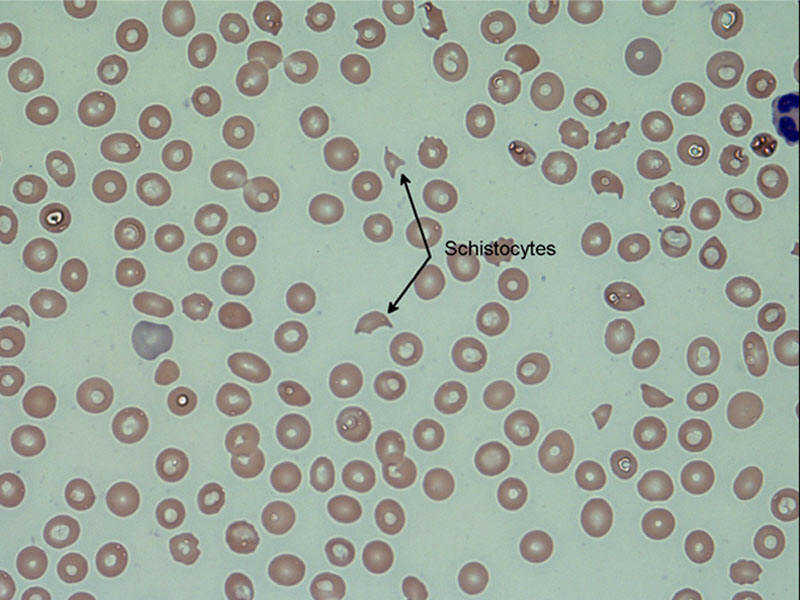
Review peripheral smear. Make sure that it is not due to platelet clumping, also
known as spurious or psuedothrombocytopenia. Attention should be made to the
smear with regards to large platelets, schistocytes
 , hypersegmented as well as
hyposegmented neutrophils, blasts, etc.
, hypersegmented as well as
hyposegmented neutrophils, blasts, etc.
|
Blood
smear with schistocytes. |
|
 |
Step 3:
History and physical examination can give clues as well. The following questions
should be asked:
1. Previous history of thrombocytopenia or other blood related problems
2. Recent infections or illnesses
3. New medications
4. Previous blood transfusions
5. Risk factors for HIV
6. Alcohol abuse, etc.
7. Dietary habits Common tests in the diagnosis of thrombocytopenia are shown in
Table 6. Anti-platelet or platelet associated antibodies are neither sensitive
nor specific. The role of these tests is not well defined. If there is suspicion
for TTP/ HUS ordering reticulocyte count, LDH and haptoglobin is highly
recommended. HIV and hepatitis tests should be done only if the patient has risk
factors.
Table 6. Common tests in the
evaluation of thrombocytopenia
|
Complete blood count with differential |
|
Reticulocyte count |
|
LDH |
|
Haptoglobin |
|
B12, folate and iron levels |
|
Anti-nuclear antibodies |
|
HIV test |
|
Hepatitis B and C antibodies |
|
Platelet associated antibodies |
Role of Bone Marrow Biopsy
Bone marrow aspiration/biopsy is minimally invasive, but usually is associated
with pain/ pressure. This should be reserved for patients in whom the above
work-up is unrevealing or if there is any suspicion for
myelodysplastic syndrome or leukemia. It
serves as a confirmatory test in immune thrombocytopenia (increased or adequate
number of megakaryocytes),
myelodysplastic syndrome (dysmegakaryopoiesis, etc.) or leukemia
(increased number of blasts- >20%). Please refer to Figure1 and
Figure 2.
Management
Treating the underlying cause is the most important intervention. If it is
immune thrombocytopenic purpura, start appropriate treatment such as steroids or
intravenous immunoglobulin (IVIG). If a drug is a suspect, discontinue the drug
and observe. Drug-induced thrombocytopenia is usually immune mediated and is
treated as immune thrombocytopenic purpura with steroids and IVIG. Heparin
Induced thrombocytopenia (HIT) is potentially life threatening condition. If
there is clinical suspicion all heparin must be discontinued and direct thrombin
inhibitor (egg. Lepirudin) must be initiated. Plasma exchange must be initiated
immediately if TTP is suspected. In HEELP syndrome, often delivery is indicated.
HIV related thrombocytopenia often responds to Zidovidine.
Platelet transfusions are generally reserved for patients who are bleeding or
have a platelet counts of <10,000/mcL. The main goal of transfusion is to
prevent bleeding. If a patient is undergoing surgery or procedure, the target
platelet count should be more than 75,000/mcL. Oprelvekin (Neumega) is an
interleukin- 11, which has been shown to reduce the severity of thrombocytopenia
due to chemotherapy and the need for platelet transfusions. It is not as widely
used as other growth factors (filgastrim, erythropoietin) due to slow response,
serious adverse reactions such as hypersensitivity reactions or anaphylaxis,
significant fluid retention. The approach for outpatient and in-patient is quite
different and is illustrated in Figure1 and
Figure 2.