
Infections Associated with Specific Immunosuppressive Agents in Transplant Recipients
Authors: Steven D. Burdette and Hsin-Yun Sun
INTRODUCTION
The incidence of infection following solid-organ transplantation varies due to numerous factors. The type of organ transplanted, the degree of immunosuppression, the need for anti-rejection therapy, and the occurrence of surgical complications all affect the incidence of infection after transplantation. Furthermore, investigators have demonstrated that viral infections, such as Epstein-Barr virus (EBV), cytomegalovirus (CMV) and hepatitis C (HCV), influence the likelihood of opportunistic infections occurring. These infections presumably contribute to the net state of immunosuppression and weaken host defenses. A major risk factor for infectious complications after solid organ transplantation is medications, including both maintenance therapy and agents used for induction or rejection.
Agents Commonly Used for Induction During Solid Organ Transplantation
Alemtuzumab, IL-2 receptor antagonists (basiliximab or daclizumab), rituximab and anti-thymocyte globulin. OKT3 is of historic interest but is no longer in production and will not be discussed. While these agents are often used for induction, they may also be utilized for rejection therapy or, in the case of rituximab, for post-transplant malignancy. Determining the actual risk of infection for each of these medications is challenging as there are many overlapping factors. Studies to assess the various complications of these medications have different patient populations with different baseline immunosuppressing medications thus often times comparing various studies can be quite challenging. Factors from these numerous studies that will determine a recipient’s risk for infection include but are not limited to:
- Medication administration for induction or rejection
- Donor and recipient CMV status
- Dosage administered
- Cumulative effect of other immunosuppressant medications
- Organ transplanted
- Prophylactic regimens
- Pediatric or adult recipients and their underlying comorbidities
- Screening protocols utilized
- Sensitive of screening tests and assays
- Environmental exposures
- Presence of immunomodulating viral infections such as EBV, HCV or CMV
The goal of this monograph is to provide an overview of the infectious and non-infectious complications of these select medications.
T-CELL DEPLETING AGENTS
Alemtuzumab
Mechanism of Action
Alemtuzumab (Campath) is a humanized monoclonal antibody directed against the membrane glycoprotein CD52 on B and T lymphocytes, monocytes, macrophages and NK cells. CD52 is an antigen whose function is unknown. Lymphoid depletion, including pan T-cell depletion, associated with alemtuzumab administration decreases global immune activity, leading to a lower anti-donor response (24, 40). The goal when administered at the time of transplantation is a lower incidence of rejection and reduced dependence on maintenance immunosuppression. It is commonly used for transplant induction therapy, rejection and for hematologic malignancies (not associated with transplant).
Side Effects
Alemtuzumab infusions may be associated with cytokine storm which can be blocked with 1 gram of methylprednisolone prior to administration (41). This infusion-related reaction typically occurs within the first 30-60 minutes after the start of the infusion. Other drug related side effects include: fever, chills, gastrointestinal symptoms (nausea, vomiting, diarrhea), rash, neurologic symptoms (dizziness, numbness, headache), respiratory symptoms (cough, dyspnea, wheezing), and/or hypotension (40, 41). The FDA black box warnings include hematologic toxicities (pancytopenia, marrow hypoplasia, autoimmune ITP, autoimmune hemolytic anemia), opportunistic infections as well as infusion reactions such as cytokine storm.
Duration of Effect
The clinically desired effects of alemtuzumab reach a nadir within 4 weeks of therapy. B lymphocytes return to normal within 3-12 months but CD4 and CD8 cells can remain significantly suppressed for up to 3 years. Many patient have total lymphocytes counts less than 25% of baseline for 9 months after therapy and may have CD4 counts lower than 100/mm3 for as long as 18-24 months (24, 41).
Malignancy
There are numerous reports of increased rates of PTLD after receipt of alemtuzumab, but recent induction studies with kidney and kidney-pancreas transplant recipients has not demonstrated an increased incidence of PTLD compared with other induction regimens (30). Studies have demonstrated an incidence of EBV viremia of 5% after induction with alemtuzumab. Long term data regarding PTLD from those studies is lacking however and ongoing studies are currently underway.
General Infectious Disease Issues
A summary of these is presented in Table 2.When alemtuzumab is used for treatment of lymphoma, observations have noted no difference in the overall number of infectious complications, but there was an increased incidence of CMV infection. Infectious complications have been evaluated when it is administered for lymphoproliferative disorders (CLL and plasma cell disorders). A 66.7% incidence in CMV reactivation was observed in this population compared with 37% in control groups. In addition, a 44.4% incidence of opportunistic infections was noted compared to control groups at 29.6%. Neither was statistically significant. Opportunistic infections included CMV, progressive multifocal leukoencephalopathy (due to JC virus), adenovirus, toxoplasmosis and acanthamaebiasis. Non-opportunistic infections included upper and lower respiratory tract infections, bacteremia, cellulitis and various nosocomial infections (32). Other studies in the hematologic-oncologic population have demonstrated infection rates of 23-79%, however, patients tend to have more prolonged exposure to alemtuzumab and have been more heavily pretreated with other immune-modulating medications. Comparing the incidence of infection in the hematologic and oncologic patient population with the transplant population must be done with great caution. Pancreas and kidney-pancreas transplant recipients who receive alemtuzumab have been shown to be infected with CMV most frequently followed by BKV, fungal infections, varicella (or herpes) zoster and EBV (including PTLD) respectively (40).
The risk for infection typically starts 3-4 weeks after the initial administration and likely has a similar risk as anti-thymocyte globulin regimens. A recent study evaluated 547 transplant patients who received alemtuzumab and identified 62 opportunistic infections in 56 patients (Table 1) (48). The median time to infection was 84 days after the last dose and 194 days after transplant. There was a shorter time to infection when alemtuzumab was used for rejection (72.5 days) as compared to induction (120 days). The mortality rate was 21% with 12.5% attributable to infection. The median CD4 count at the time of the infectious diagnosis being made was 10/mm3. The four independent risk factors for an opportunistic infection in the one study included:
1. Receipt of Alemtuzumab for rejection
2. Lung or heart/lung transplant
3. Intestinal or multi-visceral transplant
4. Allograft failure
Bacterial Infections
Numerous studies have demonstrated a lower incidence of bacterial infections as compared to other induction regimen (induction dose is lower than the chemotherapy dose) with bacterial pneumonia and sepsis being reported most frequently. Due to the profound depletion of CD4 cells, the theory existed that patients who received alemtuzumab would be at risk for pathogens commonly associated AIDS. However, a study of 449 patients who received alemtuzumab as part of solid organ transplantation demonstrated that the most common causes of blood stream infections were Staphylococcus aureus, Coagulase negative Staphylococcus, Klebsiella, Enterococcus and Escherichia coli. No patients were reported to be infected with Streptococcus pneumoniae, Listeria, non-typhoidal Salmonella, or Mycobacterium avium complex (MAC). Therefore, while the immunologic status of AIDS patients is similar to those treated with alemtuzumab, their infectious complications do appear to be different (57). The same study demonstrated no difference in blood stream infections between utilization for induction and rejection (14% v17.6%) though infection did occur sooner when used for induction (23 days v 70 days). A blood stream infection (BSI) developed in 15% (69/449) (57). Others have noted that when it was used for rejection, bacterial infections occurred earlier than with induction (72.5 days v 120 days) (48).
There has been an association between alemtuzumab and Nocardia (disseminated and pulmonary) and non-Tuberculosis mycobacterium (NTM). This has mostly been noted when used for rejection. However, other studies of lymphocyte depleting therapy (including both alemtuzumab and anti-thymocyte globulin) have not been associated with Nocardia infections while high dose steroids, CMV infection and high calcineurin inhibitor levels were (49).
Viral Infections
Herpes Viruses: A retrospective review of 118 liver transplant recipients who had received alemtuzumab induction demonstrated that herpes zoster (HZ) occurred in 12 patients with a median time to infection of 10.2 months after transplant. It was calculated that the cumulative probability of developing HZ was approximately 16%. All patients had only 1 dermatome involved and there was no systemic infection or complications such as post-herpetic neuralgia. The incidence of HZ after solid organ transplant has previously been reported to be 8.6% while other studies have shown a rate of HZ after orthotopic liver transplantation of 1.2-18% (1). HSV reactivation is also a possibility, though there is no specific data available regarding the incidence associated with alemtuzumab. HZV and HSV typically occur once off of all antiviral prophylaxis (including CMV prophylaxis).
CMV has been demonstrated to be the most common opportunistic infection (median of 85 days after receipt of alemtuzumab and 145 days after transplant) after receipt alemtuzumab (for either induction or rejection) (48). When comparing alemtuzumab with IL-2R antagonists, there was an increased incidence of CMV (24.6% v 9.3%) though compared with anti-thymocyte globulin, the incidence was similar (54). When it is used for rejection, CMV often occurs within 3 months, though studies typically have patients also treated with ATG therapy. As expected, the incidence of CMV infection varies based on donor and recipient serostatus, which donor-positive to recipient-negative having the highest incidence (30). Thirty-three renal transplant recipients who received alemtuzumab induction with half-dose cyclosporine were compared to a control group treated with convention immunosuppression including cyclosporine, azathioprine and prednisolone. Graft loss was similar in both groups while there was no difference in infections or serious adverse events. CMV was noted in the control group more often (6 to 1) while zoster occurred in the alemtuzumab group more often (5 to 1), however, neither was statistically significant44. In regards to the efficacy of prophylactic treatment for CMV, studies have demonstrated that antiviral prophylaxis is effective when utilized (47). However, one study demonstrated significant antiviral prophylaxis failure when 2 doses of alemtuzumab were given (30).
BK Virus: The data is mixed regarding the role that alemtuzumab plays in BK virus infections. Simultaneous pancreas-kidney transplant recipients (n=243) who were treated with induction agents (either alemtuzumab or ATG) had fewer episodes of BKVAN (incidence of 1.4%) than recipients treated without induction but with triple therapy (incidence of 2.9%) (17). No episodes of BK infection (or CMV infection) were found in 26 consecutive pediatric renal transplant recipients who were treated with alemtuzumab induction and tacrolimus monotherapy. The mean recipient age in the study was 10.7 years, raising the possibility that there was a low incidence of prior BK infection in either the donor or recipient (56).
When comparing alemtuzumab with IL-2R antagonists, there has been an increased incidence of BK, but compared with other T-cell depleting induction regimens the incidence was unchanged. The incidence of BKVN following simultaneous pancreas-kidney recipients has been noted to be 6.8% (4/59) with ATG while alemtuzumab incidence was 5.1% (5/146) (23). There was no statistical significance between the two groups. Kidney-pancreas recipients who received induction with alemtuzumab have demonstrated a 4% BK infection rate after 2 year follow-up (30).
HBV/HCV Infection: There is limited data on the role that alemtuzumab plays with HBV/HCV reactivation after solid organ transplantation. In 2007, only 1.4% of orthotopic liver transplant recipients received it thus there is minimal data on this topic (14). In the oncologic population, alemtuzumab has been associated with reactivation of chronic HBV infection, though there is limited data in the solid organ transplant literature. Alemtuzumab and tacrolimus monotherapy in liver transplant recipients who are HCV positive has demonstrated no difference in HCV recurrences and alemtuzumab added no benefit over conventional therapy in those that were HCV positive (31). Others have reported increased systemic infections in HCV positive orthotopic liver transplant recipients (in addition to increased HCV viral load titers) thus it is no longer utilized in this population (14). More definitive studies are necessary to clarify its role in this patient population.
Fungal Infections
In patients who have been treated with alemtuzumab, a similar rate of fungal infections has been documented as compared with other induction agents. However, there is an increased incidence when it used for rejection. Aspergillus, zygomycetes, Histoplasmosis, Blastomycosis, Cryptococccosis have all been reported and typically occur within 3 months of therapy (24). Fungemia developed in only 1.5% of patients according to one study of alemtuzumab for induction in solid organ transplant (57). Cryptococcosis has been associated with the receipt of 2 but not 1 dose when used in renal or liver transplant recipients. Median time to the diagnosis was 255 days with a death rate of 14.2% (58). In a study of 121 pancreas transplant recipients (56 induction, 65 conversion) with CNI maintenance therapy, fungal infections developed in 8 (6.6%) patients (2 with induction, 6 with conversion) and were diagnosed at a median time of 115 days after treatment (44). The four fungi identified included: Cryptococcus, Histoplasma, Aspergillus, and Candida. Three of these patients died as a complication of the fungal infection.
T cell depleting antibody therapy (such as ATG or alemtuzumab) has not been associated with zygomycetes infection while renal failure, diabetes, prior voriconazole or caspofungin use were. Tacrolimus lowered the risk of zygomycosis infection (59).
Other Infections
Parasites including toxoplasmosis, acanthamebiasis and Balamuthia have been described when drug used for rejection. The risk for PCP infection is also increased with administration of alemtuzumab though infection can be prevented with appropriate prophylactic measures.
Impact on Prophylaxis and ID Screening Recommendations
Patient should receive PCP prophylaxis for 6-12 months after receipt of alemtuzumab, regardless of whether it is used for induction or rejection. Some centers utilize lifelong PCP prophylaxis, especially in the heart and lung transplant population. Trimethoprim-sulfamethoxazole (TMP-SMX) is the preferred agent, though dapsone, atovaquane or pentamidine are also effective. A G6PD qualitative assay should be performed before starting dapsone therapy. Patients who are at risk of CMV infection should be monitored by quantitative CMV assays every 2 weeks for 6 months after induction therapy in the absence of anti-CMV prophylaxis. If prophylaxis is utilized, then valganciclovir should be provided for 3-6 months, though recent data suggests that 6 months may be more effective. Some also endorse following a preemptive protocol with routine screening for CMV infection after the discontinuation of CMV prophylaxis, though the data supporting this approach is limited and may not be cost effective. The frequency and duration of CMV screening with a secondary preemptive protocol is not clear. When donor and recipient are both CMV negative, antiviral prophylaxis (e.g., famciclovir, valacyclovir, or acyclovir) for 4–6 months is recommended for prevention of infection with herpes simplex virus or varicella-zoster virus. BK virus screening should occur in renal transplant recipients and should be done monthly for the first 6-12 months followed by quarterly evaluations. Recipients who are EBV negative but receive an EBV positive organ should be screened monthly for EBV viremia for 12 months and if viremia is detected, appropriate adjustments in maintenance immunosuppression should take place. In patients who are HCV antibody positive, a quantitative HCV RNA load measurement is recommended at baseline and at 3, 6, 9, and 12 months after transplantation. Quantitative HCV load does not correlate with the degree of hepatic injury, and a liver biopsy will be needed to guide decisions regarding antiviral therapy. If there is a history of exposure to Histoplasma, Cryptococcus, Coccidiodomycosis, or Blastomycosis, then prophylaxis for 6-12 months with the appropriate antifungal therapy is indicated. If antifungal prophylaxis with an azole is utilized, proper adjustment with CNI or rapamycin must take place. Monitoring with antigen assays or immunoassays for Histoplasma and Cryptococcus species (and more recently for species that cause coccidioidomycosis and blastomycosis) may be useful.
Anti-thymocyte globulin
Anti-thymocyte globulin exists in 2 forms, though only 1 is currently used clinically. Rabbit anti-thymocyte globulin (R-ATG, ATG, Thymoglobulin) is obtained from rabbits immunized with cells derived from fragments of the human thymus gland. Human anti-thymocyte globulin (H-ATG, Atgam) is developed from serum of horses immunized with human thymus lymphocytes. Due to superior efficacy and a cleaner side effect profile, R-ATG is the most commonly used preparation for both solid organ transplant induction as well as for treatment of rejection.
Mechanism of Action
ATG is a polyclonal antibody that induces dose dependent depletion of T-cells while also having some effect on B-cells and interferes with dendritic cells, regulatory T-cells, and NK cell functions. The degree of T-cell depletion is based on total dose administered and the duration of therapy. A typical course of therapy is 3-5 days (range 1-10) (63). Longer courses are used to avoid calcineurin-induced nephrotoxicity. Neutralizing antibodies may develop against ATG that limit effectiveness of future therapy. One advantage of induction with ATG is the possible protective effect against reperfusion injury when administered prior to reperfusion of solid organs. This occurs via blockade of adhesion molecules, a decreased cell surface expression of B1 and B2 integrins and blockade of endothelial inflammatory cells such as ICAM-1.
Side Effects
ATG can induce a myriad of symptoms during infusion. Fever, chills, hypotension, serum sickness, CHF, leucopenia or eosinophilia, thrombocytopenia and rash have all been reported. Personal experience suggests that fever, leucopenia and thrombocytopenia are the most frequently encountered side effects (7, 9, 43). Leucopenia associated with ATG can make utilization of antimetabolites such as MMF and ganciclovir/valganciclovir challenging. Post-transplant patients who develop fever in the immediate postoperative period should be assessed to determine if the fever coincide with the infusion of ATG.
Duration of Effect
R-ATG long half life (30 days) but the profound CD3 lymphopenia may last up to 1 year. H-ATG has less intense CD3 suppression and a shorter duration of effect (lymphopenia resolves within 14 days) (24).
Malignancy
EBV associated PTLD is likely increased with ATG induction, though studies do demonstrate variable results due to different populations, risk factors, ages, etc. A higher incidence of malignancy has been noted with H-ATG as compared to R-ATG (21% v 6%). Renal transplant recipients treated with CNI monotherapy had no difference in PTLD or de novo malignancy (~400 patients) as compared to standard therapy. The highest risk population would be EBV D+/R-, particularly children, who are treated with ATG (24).
One study evaluated 391 orthotopic liver transplant recipients who received either CNI immediately after orthotopic liver transplantation (n = 129) or received a 3-day induction with ATG followed by delayed initiation of CNI. There was no statistical significance between the incidence of PTLD (2.3% with ATG and 0.9% control) and no statistical difference in the recurrence of hepatocellular tumors (1.9% with ATG and 5.4% in control group) (64). In another study of 472 orthotopic liver transplant patients who received either short course (3 day) or long course (10 day) therapy with ATG, there were no significant differences in PTLD or de novo malignancies (63). However, the longer course of induction was associated with higher rates of rejection as well as fatal infections.
General Infectious Disease Issues
There have been several studies that have compared R-ATG with H-ATG. In one such study, 56% of patients who were treated with R-ATG developed infection during the first year after transplant as compared to 75% with H-ATG. Another study compared R-ATG with OKT3 for steroid resistant renal transplant rejection. There were similar rates of CMV infection, bacterial pneumonia and no significant differences in overall infections between the two therapies. ATG compared with alemtuzumab or daclizumab for induction during renal transplantation demonstrated a 27% incidence in infection in each group with only 3 total cases of CMV and 1 case of BKVN (10).
Bacterial Infections
Effect of ATG on bacterial infections is somewhat unclear. Most studies showed no difference in rates of infection as compared to those who received no induction or other regimens (alemtuzumab or basiliximab) (Table 3). In kidney or kidney-pancreas recipients, there have been increased rates of urinary tract infections as well as wound infections. Other studies have associated ATG with increased reports of pneumonia, sepsis or bacteremia (37). Studies of lymphocyte depleting therapy (including both alemtuzumab and anti-thymocyte globulin) have not been associated with Nocardia infections while high dose steroids, CMV infection and high calcineurin inhibitor levels were (high dose steroids, CMV and high calcineurin inhibitor levels were a risk factor) (49).
Viral Infections
Herpes Viruses: There has been a long standing concern regarding ATG and CMV infection and disease. The association is related to depletion of T-cells, inversion of CD4/CD8 ratio, shift towards Th2 cytokines, release of TNF after infusion leading to stimulation of cellular nuclear factor kB and viral replication. The incidence and timing of CMV infection depends on the dose of ATG, donor/recipient serostatus, and the utilization of CMV prophylaxis. When utilized without prophylaxis, the rate of CMV (38%) was greater than with basiliximab (11.7%). One study demonstrated a rate of CMV infection of 32.5% in renal transplant recipients who received ATG induction compared with a rate of 19% in the non-induction group (39). A comparison of SPK recipients who were treated with ATG and those who did not receive induction therapy showed a statistically significant increase in CMV in those treated with ATG (7). Others have found the lowest rate of CMV infection was in renal transplant recipients was those who were treated with immediate tacrolimus therapy with induction (15.7%). The highest rate of CMV was ATG with cyclosporine (28.3%) followed by ATG with tacrolimus (24.2%) (9). The risk of CMV infection has also been demonstrated when ATG is used for rejection therapy.
BK Virus: Some studies link ATG induction to an increase risk of BVN (12). A prospective study showed that 19.4% of renal transplant recipients had BK viremia within 6 months of transplant; BK typically develops in 1-10% of patients who do not receive induction therapy.
An evaluation of the SRTR database identified an incidence of BKV was 1.6% at 6 months, 2.6% at 1 year. Risk factors for BKV included advanced donor age, pediatric recipient, African-American and male recipients, HLA mismatch and tacrolimus and ATG induction. Adjusted odds ratio was 1.73 with ATG versus 1.16 with IL-2R antagonists. Based on adjusted odds ratios, ATG was the most significant risk factor for BKV (54).
HBV/HCV: As expected, the data is somewhat variable in regards to the association of ATG and HCV infection. Induction of HCV positive recipients (especially liver), may increase viral replication and increase the rate of progression to cirrhosis. Progression is accelerated by CMV co-infection. In liver transplant recipients, no difference was found in recurrent HCV as compared to control group (40% with R-ATG v 64% in control) (24). Renal transplant recipients who received R-ATG did NOT have more accelerated viremia, cirrhosis, or increased mortality. Liver transplant recipients who were HCV + or – and received ATG were noted to have similar patient and graft survival rates (67). 32% had biopsy proven recurrent HCV between months 1 and 10 and 3 (of 18) were severe. Another study compared steroids with ATG induction for liver transplant. The same response rate to HCV antiviral treatment was noted in both groups, advanced fibrosis at 4 years was comparable between groups, but there was more severe inflammation at 3 months in the steroid group (25%) as compared to the ATG group (15%) (42).
There is limited data regarding solid organ transplant patients with chronic or active hepatitis B and their outcomes after ATG therapy.
Fungal Infections
In general, induction with ATG does not lead to increased risk for fungal infection. Anti-rejection utilization does increase the risk for fungal infection. ATG is associated with an increased risk for PCP without prophylaxis. False positive Histoplasma urine antigens have been identified in those who have received R-ATG. Cryptococcosis was associated with receipt of 2 doses of R-ATG but not 1 dose when used in renal or liver transplants. Median time to diagnosis was 255 days and the death rate was 14.2% (58). T cell depleting antibody therapy (such as ATG or alemtuzumab) has not been associated with zygomycetes infection while renal failure, diabetes, prior voriconazole or caspofungin use were. Tacrolimus lowered the risk of zygomycosis infection (60).
Impact on prophylaxis and ID screening recommendations
Patient should receive PCP prophylaxis for 6-12 months after receipt of alemtuzumab, regardless of whether it is used for induction or rejection. Some centers utilize lifelong PCP prophylaxis, especially in the heart and lung transplant population. Trimethoprim-sulfamethoxazole (TMP-SMX) is the preferred agent, though dapsone, atovaquane or pentamidine are also effective. A G6PD qualitative assay should be performed before starting dapsone therapy. Patients who are at risk of CMV infection should be monitored by quantitative CMV assays every 2 weeks for 6 months after induction therapy in the absence of anti-CMV prophylaxis. If prophylaxis is utilized, then valganciclovir should be provided for 3-6 months, though recent data suggests that 6 months may be more effective. Some also endorse following a preemptive protocol with routine screening for CMV infection after the discontinuation of CMV prophylaxis, though the data supporting this approach is limited and may not be cost effective. The frequency and duration of CMV screening with a secondary preemptive protocol is not clear. When donor and recipient are both CMV negative, antiviral prophylaxis (e.g., famciclovir, valacyclovir, or acyclovir) for 4–6 months is recommended for prevention of infection with herpes simplex virus or varicella-zoster virus. BK virus screening should occur in renal transplant recipients and should be done monthly for the first 6-12 months followed by quarterly evaluations. Recipients who are EBV negative but receive an EBV positive organ should be screened monthly for EBV viremia for 12 months and if viremia is detected, appropriate adjustments in maintenance immunosuppression should take place. In patients who are HCV antibody positive, a quantitative HCV RNA load measurement is recommended at baseline and at 3, 6, 9, and 12 months after transplantation. Quantitative HCV load does not correlate with the degree of hepatic injury, and a liver biopsy will be needed to guide decisions regarding antiviral therapy. If there is a history of exposure to Histoplasma, Cryptococcus, Coccidiodomycosis, or Blastomycosis, then prophylaxis for 6-12 months with the appropriate antifungal therapy is indicated. If antifungal prophylaxis with an azole is utilized, proper adjustment with CNI or rapamycin must take place. Monitoring with antigen assays or immunoassays for Histoplasma and Cryptococcus species (and more recently for species that cause coccidioidomycosis and blastomycosis) may be useful.
![]()
T-CELL NON DEPLETING AGENTS
IL-2 receptor antagonists (basiliximab, daclizumab)
Mechanism of Action
Basiliximab (Simulect) is a chimeric murine-human monoclonal antibody that binds selectively to the alpha chain (CD25) of the IL-2 receptor while dalcizumab (Zenapax) is a humanized IL-2R antagonist that contains a hyper variable region of murine antibody against IL-2 receptor alpha chain (CD25). IL-2 is a leukocytotrophic hormone that is instrumental in the body's natural response to microbial infection and in discriminating between foreign and self. CD25 is a type I transmembrane protein present on activated T-cells, activated B-cells, some thymocytes, myeloid precursors and oligodendrocytes. CD25 associates with CD122 to for a high affinity receptor for IL-2. Resting lymphocytes are not targeted by IL-2 receptor antagonists. CD25 participates in lymphocyte differentiation, activation, and proliferation. At this time, these medications are used mostly for solid organ induction in recipients who are low risk for rejection.
Side Effects
IL-2R antagonists are not commonly associated with infusion related toxicities. However, frequent vital sign monitoring should occur during infusion as there is a small risk of anaphylaxis. According to various clinical trials, IL-2R antagonists do not appear to add to the background of adverse events seen in organ transplantation patients as a consequence of their underlying disease and the concurrent administration of immunosuppressants. In four placebo-controlled studies, the pattern of adverse events in 590 patients treated with the recommended dose of basiliximab was similar to that in 594 patients treated with placebo. Basiliximab did not increase the incidence of serious adverse events observed compared with placebo. The most frequently reported adverse events were gastrointestinal disorders, reported in 69% of Simulect-treated patients and 67% of placebo-treated patients.
Duration of Effect
Both agents have a long half life (13.4 days adults, 9.4 days children). Basiliximab gives complete IL-2R saturation for 4-6 weeks in adult renal transplant recipients and for 42 days in pediatric recipients. Daclizumab saturates the IL-2 receptors for at least 3 months.
Malignancy
Rates of PTLD are similar to those recipients who get placebo or other induction regimens and have been reported to occur in less than 1% of patients.
General Infectious Disease Issues
A benefit of the IL-2 receptor antagonists is the likely decreased risk of infectious complications as compared with T-cell depleting agents. No increase has been noted in various studies in CMV, fungal and bacterial infections as compared to placebo or other therapies for induction (6, 8, 20, 29, 30, 33) (Table 4). When used for rejection, there were higher rates of CMV in one study as compared to ATG (17.5% v 7.8%) though this has not been confirmed in other studies. In clinical trials leading to basiliximab’s approval, the overall incidence of cytomegalovirus infection was similar in basiliximab- and placebo-treated patients (15% vs. 17%) receiving a dual- or triple-immunosuppression regimen. However, in patients receiving a triple-immunosuppression regimen, the incidence of serious cytomegalovirus infection was higher in basiliximab-treated patients compared to placebo-treated patients (11% vs. 5%) (43). The overall rates of infections, serious infections, and infectious organisms were similar in the basiliximab- and placebo-treatment groups among dual- and triple-therapy treated patients.
Personal experience suggests significantly less BK virus infection and more rapid viral clearance with intervention as compared with anti-thymocyte globulin therapy. In regards to HCV, the associated risk is unknown as studies have shown both increased and decreased rates of HCV recurrence. No data is available regarding HBV infection. There are no special recommendations for infectious disease screening in patients treated with IL-2 receptor antagonists. Standard prophylactic or preemptive strategies are encouraged.
![]()
ANTI- CD20 ANTIBODY
Rituximab
Mechanism of Action
Rituximab (Rituxan) is a chimeric human-murine anti-CD20 monoclonal antibody, first approved in 1997 for refractory B-cell lymphoma (70). It primarily depletes B cells thus affecting humoral immunity and should not affect the T cell immune response. There are 3 proposed mechanisms of action:
1) Antibody dependent cell-mediate cytotoxicty
2) Complement dependent cytotoxicity
3) Apoptosis
Side Effects
First dose infusion reactions with fever may occur. Rituximab administration can result in serious, including fatal infusion reactions. Approximately 80% of fatal infusion reactions occurred in association with the first infusion. It has been suggested to consider infusing first dose with a steroid bolus and it is recommended that patients be pretreated with an antihistamine and acetaminophen (72). Infusion reactions and sequelae include urticaria, hypotension, angioedema, hypoxia, bronchospasm, ARDS, myocardial infarction, cardiogenic shock, anaphylaxis, or death. Other noted side effects include late onset neutropenia. Mucocutaneous reactions (such as Stevens-Johnson syndrome), some with fatal outcome, can occur in patients treated with rituximab. The onset of these reactions has varied from 1-13 weeks following exposure. Hematologic side effects include lymphopenia, neutropenia and decreased serum IgG and IgM levels.
Duration of Effect
Lymphopenia lasts a median of 14 days but may last for 1 year. B cells that recover lack CD-27 (TNF receptor) for as long as 2 years. One study compared renal transplant recipients who received rituximab to placebo induction with subsequent standard tripe therapy with steroids, tacrolimus, MMF. They noted fewer and milder rejection episodes during the first 6 months and their recipients demonstrated complete B cell depletion with 1 dose. No difference was noted in IgG, IgM, anti-CMV and anti-tetanus at baseline, 3 or 6 months. There was no increase in infectious complications or leukopenia (69).
Malignancy
Rituximab may be protective against PTLD and is often times used to treat PTLD that are biopsy proven CD20 positive. A small, single center study had no cases of PTLD in intestinal transplant recipients while the usual rate is 6-8% (70).
General Infectious Disease Issues
Rituximab is generally considered to have a lower infectious risk profile (depicted in Table 5) than are alemtuzumab and anti-thymocyte globulin. Rheumatoid arthritis (RA treated with rituximab demonstrated that the risk of infection, including opportunistic infection was dose dependent (total dose >2,000 mg increased risk for opportunistic infections). Most of the infections were bacterial (pneumonia, septic arthritis, and pyelonephritis). The infection rates were 2.3% versus control group of 1.5%. There was no TB reported (53). There are case reports of Parvovirus B19 (with associated pure red cell aplasia) and West Nile Virus infection complicating therapy with this medication.
Recently published data further evaluates the incidence of infection and infection associated mortality after rituximab therapy in renal transplant recipients. Seventy-seven patients who received rituximab for various reasons were compared with 902 renal transplant recipients who did not receive rituximab. Overall, the rate of bacterial infections was similar between the two groups while viral infections were more frequent in the control group. Fungal infections were more common after rituximab therapy (including as compared with the ATG treated subgroup). In regards to infection related mortality, the combination of rituximab and ATG was independently associated with infection related mortality. Administration of rituximab or ATG alone was not associated with death (39). These conflicting results suggest that further data and long term follow-up on the safety of rituximab (alone or in combination with other medications) in solid organ transplant is still lacking.
Bacterial Infections
No increased risk of bacterial infections as compared to placebo based induction with standard triple immunosuppression therapy has been observed (69). No increase in bacterial infections has been noted with rituximab when used for rejection as compared to thymoglobulin. However, it has been associated with inability to clear Babesia microti infection.
ABO incompatible, positive cross match renal transplant recipients who were pretreated with rituximab plus plasmapharesis and anti-thymocyte globulin have been evaluated to assess bacterial infections associated with this regimen. Thirteen patients had 21 episodes of infection (8 soft tissue infections, 5 blood stream infections, 3 esophagitis, 1 pneumonia). The rate of infection was 48% compared with a historic control group at 11%. Despite the increased rate of infection, there was no difference in rate of rejection, graft or patient survival (16). However, it is difficult to draw conclusion regarding rituximab’s role in contributing to infection in patients who are also treated with anti-thymocyte globulin therapy.
Viral Infections
Herpes Viruses: Data suggests there is no increased risk for CMV infection as compared with other regimens (46). Rituximab after renal transplant was compared with basiliximab and standard therapy. The rate of CMV infection with rituximab induction was 58% compared with the control group at 75%. There was no difference between low dose (200 mg) and high dose (500 mg) therapy. Four patients in the rituximab treatment arm converted from CMV IgG negative to IgG positive after treatment suggesting adequate humoral response. The rituximab arm did not have more prolonged or refractory CMV infection. Rituximab was not a risk factor for CMV infection based on multivariable analysis while acute rejection and CMV D+/R- was (46).
BK Virus: There is a scarce data on BKV infection though likely the risk is not increased (69). There is one report of BK clearance with rituximab therapy but there is also a report of BK leukoencephalopathy in a stem cell recipient who was treated with RTX. Rituximab has been associated with JC virus associated progressive multifocal leukoencephalopathy therefore standard monitoring for BK viral infection in the appropriate host should be employed regardless of when the in the post-transplant period it is administered.
HBV/HCV: A somewhat unique viral infection that recipients of rituximab are at risk for is hepatitis B reactivation. There are numerous reports of HBV reactivation regardless of surface antibody status, though this is mostly outside of the transplant literature. HBV reactivation has occurred as late as 1 year after rituximab treatment and often occurs in core antibody positive patients. In patients with lymphoma, it has been reported to be associated with HBV reactivation despite detectable antibody levels prior to infusion but was antibody undetectable after treatment (68).
Rituximab does not seem to increase chance for HCV reactivation, though there is a lack of data on this.
Fungal Infections
When used for renal transplant induction, there is no difference in fungal infection rates as compared to placebo (69). However, recently data is somewhat conflicting and this needs to be further clarified in future studies (39). Rituximab does not affect T cells therefore should not lead to increased risk for PCP, however, in the oncologic population there are case reports of PCP infection. Whether the diagnosis of PCP was due to rituximab, underlying malignancy or other therapies is not clear. Further data is needed to clarify this and to determine if this issue crosses over to transplant recipients.
Impact of Drug on Prophylaxis (Type and Duration) and ID Screening Recommendations
Patients treated with rituximab do not require any special prophylactic therapy with the exception of HBV infection. Solid organ transplant recipients who receive rituximab as part of induction therapy should receive standard prophylaxis as guided by institutional protocols. CMV prophylaxis (or preemptive therapy) should be undertaken and guided by donor and recipient CMV status. Reinstitution of CMV prophylaxis following rituximab therapy for rejection or PTLD is not needed. Due to the lack of impact on T cell function, there is no need for prolongation in PCP prophylaxis. There is no data in regards to antifungal prophylaxis, though the lack of associated increase in fungal infections suggests that no special prophylaxis be undertaken.
In regards to HBV, we recommend consideration of prophylaxis in chronic hepatitis B (including core antibody positive regardless of the surface antibody status) even if the patient is surface antibody positive (as rituximab has been associated with loss of surface antibody protection). An alternative would be routine screening for viral activation and subsequent preemptive therapy.
![]()
CONCLUSION
Determining the actual risk of infection for each of these medications is challenging as there are many overlapping factors. ATG and alemtuzumab in general have a greater impact on the risk for infectious complications as compared with rituximab or the IL-2R antagonists though many of these drugs have its own unique infectious niche. Each transplant patient should be evaluated on an individual basis and their net state of immunosuppression should be considered with special focus on the potential receipt of any of the above medications. Reinstitution of appropriate prophylaxis after administration, especially with ATG and alemtuzumab, can help prevent infectious complications that could lead to undesired outcomes.
![]()
CALCINEURIN INHIBITORS
Calcineurin inhibitors first introduced in 1980s included cyclosporine A and tacrolimus (FK506). With their advent, the risk of acute rejection in solid organ transplant recipients was substantially reduced, and short-term outcomes were significantly improved (25). As a result, calcineurin inhibitors have emerged as the cornerstone of maintenance immunosuppression. cyclosporin and FK506 exert their potent immunosuppression by binding to cyclophilin and FK506-binding proteins 12 (FKBP12), respectively. Cyclophilin and FKBPs are intracellular binding proteins known as immunophilin. These immunophilin-immunosuppressant complexes inhibit calcineurin activity (19). This inhibition prohibits subsequent translocation of nuclear factor of activated T cells to the nucleus, and, as a result, production of interleukin-2 (IL-2) necessary for T cell proliferation is blocked, leading to markedly diminished T-cell response to alloantigens. Tacrolimus is 100 times more potent than cyclosporine. A meta-analysis of 16 randomized clinical trials concluded that the performance of tacrolimus is better than that of cyclosporine in survival, graft loss, acute rejection, and steroid-resistant rejection in the first year (18, 34).
Cyclosporine and tacrolimus have similar side effects, such as nephrotoxocity, hyperkalemia and hypomagnesemia (19). Nevertheless, hyperlipidemia, hypertension (usually within the first few weeks of therapy due to renal vasoconstriction and sodium retention), skin changes, hirsutism, and gigival hyperplasia, and bone loss develop more frequently in patients receiving cyclosporine while posttransplant diabetes, neurotoxicity (such as headache, seizure, posterior leukoencephalopathy, and hand tremor; usually reversible after dose reduction or discontinuation), gastrointestinal symptoms (diarrhea and abdominal discomfort), alopecia, hyperuricemia and exacerbation of gout occur more often in patients receiving tacrolimus (19). Since both agents are metabolized by cytochrome P450, meticulous review of concurrent medications and close monitoring of cyclosporine or tacrolimus levels is essential to avoid drug overdose or under dosing due to drug-drug interaction.
The frequency and spectrum of infections in organ transplant recipients does not appear to be notably modified by the choice of calcineurin-inhibitor agents per se (61). Some studies have reported a higher risk of cytomegalovirus and poorer outcomes associated with hepatitis C virus in patients receiving cyclosporine, but it may be related to a greater requirement of adjunctive immunosuppression, such as T-cell antibodies, with cyclosporine-based regimens (61). Tacrolimus with or without mycophenolate mofetil is believed to be a significant contributor to a higher incidence of BK virus nephropathy in renal transplant recipients (5).
Despite the potent immunosuppressive action, calcineurin inhibitors also have antifungal attributes (62, 66). Cryptococcus neoformans, Candida albicans, and Aspergillus fumigatus have calcineurin homolog (62, 66). It has been shown that calcineurin pathway similar to the one in mammalian exists in these fungi, and contributes to their virulence, antifungal drug tolerance, etc. (62, 66). Calcineurin is required for growth of C. neoformans at 37oC but not at 24oC. Thus, at high-temperature stress, calcineurin inhibitors impair Cryptococcus growth. Cyclosprine does not penetrate the central nervous system well, and tacrolimus demonstrated greater activities against C. neoformans than cyclosporine (11, 50). At 37oC, minimum inhibitory concentration (MIC) of tacrolimus for C. neoformans was <0.09 µg/mL while that of cyclosporine was 0.39-5 µg/mL (11). Nevertheless, the receipt of calcineurin inhibitors does not change the incidence of cryptococcosis in solid organ transplant recipients, but it influences their predominant clinical manifestations, including less CNS disease, more skin and soft-tissue infections, and a lower mortality (21, 60).
Calcineurin inhibitors also have antifungal activity against A. fumigatus (66). Additionally, calcineurin inhibitors enhance the activities of antifungal agents. Calcineurin inhibitors are synergistic with fluconazole against C. neoformans and Candida species, and with caspofungin against Aspergillus species (62). MIC of tacrolimus for C. neoformans decrease approximately 30 folds and that of fluconazole decrease 3 fold (13). Furthermore, long-term exposure to calcineurin inhibitors does not select calcineurin inhibitors-resistant isolates (66).
![]()
ANTIMETABOLITES
Mycophenolate Mofetil (MMF)
MMF is metabolized in vivo to mycophenolic acid (MPA), a potent inhibitor of inosine-5’-monophosphate dehydrogenase (IMPDH) (2). MPA preferentially inhibits de novo guanosine synthesis, and results in a lack of deoxyguanosine triphosphate which suppresses DNA synthesis and subsequent proliferation of T and B lymphocytes (3). Activated T lymphocytes, cytotoxic T cells, the proliferation of human B lymphocytes, and immunoglobulin production are all negatively affected by MMF (51). Because MMF does not have neurotoxicity and nephrotoxicity, it is widely employed as a calcineurin inhibitors- or steroid-sparing agent. Hematologic changes (anemia or leukopenia) and gastrointestinal complaints (mainly diarrhea) are most commonly encountered side effects (19). These symptoms are usually dose-related, and may be improved with dose reduction. Dosing should be one hour before or two hours after meals to avoid food interference with absorption.
CMV disease is the infection most commonly associated with receipt of MMF (22, 51). Although information about ganciclovir prophylaxis was not always provided, compared with patients receiving azathioprine in the majority of studies, many studies reported a significantly higher incidence of CMV disease in patients receiving MMF at a dose of either 3g/day or 2g/day (22, 51). Nevertheless, in a review and meta-analysis of calcineurin inhibitor sparing with MMF in 19 randomized controlled trials with cyclosporine as the comparator in most studies, the incidence of infections and CMV disease/infection rates did not differ in two groups (38). The mechanism by which MMF may enhance the risk of CMV infection/disease remain unclear while some studies suggested decreased CMV IgM levels may correlate with the risk of CMV disease. Additionally, patients receiving MMF with or without tacrolimus were more likely to have BK virus viremia or nephropathy (3, 36, 55). Varicella-zoster virus has also been reported to occur more commonly in MMF recipients.
In addition to its immunosuppressive effect, MMF also demonstrated antimicrobial activities against several pathogens in in vitro or animal models, including Dengue virus, hepatitis C virus, hepatitis B virus, Pneumocystis jirovecii, Coxsachie virus B3, West Nile virus, yellow fever virus, and human immunodeficiency virus (HIV) (51). Nevertheless, except for its activity against Pneumocystis pneumonia (PCP) in liver transplant recipients (22), other antimicrobial activities have not been observed or evaluated in clinical settings. The exact mechanisms of these antimicrobial effects remain unclear, and some may be independent of inhibition of guanosine synthesis.
Sirolimus
It is gradually recognized that calcineurin inhibitors do not improve long-term renal allograft survival (35), and the nephrotoxicity of calcineurin inhibitors is considered to be one of the reasons (15). Thus, efforts have been made to reduce or eliminate the use of calcineurin inhibitors, such as sirolimus-base calcineurin inhibitors sparing regimen. Like tacrolimus, sirolimus binds to FKBP12 forming FKBP12-rapamycin complex while the target of this complex is mammalian target of rapamycin (mTOR), not calcineurin (19). mTOR signaling proceeds via two complexes: TOR Complex 1 (TORC1) and TORC2, and mTOR inhibition results in proliferation blockade, IFN-γ suppression, and fostering of Treg emergence (52).
Although the use of sirolimus reduces chronic renal graft damage and prevents malignant development, its use is limited by the high incidence of side effects (65). Hyperlipidemia is most common; total cholesterol, triglycerides, and apolipoprotein C-III are affected (27). Other side effects include impaired glucose tolerance and posttransplant diabetes mellitus, impaired wound healing, increased incidence of lymphocele formation, proteinuria, acute renal toxicity, anemia, interstitial pneumonia, mouth ulcers, joint pain, and edema. The majority of these side effects are dose-dependent, and some risk factors are identified, such as obesity and concurrent use of corticosteroids for impaired wound healing. Thus, careful patient selection and high dose avoidance are suggested when sirolimus is employed (65). Sirolimus is a substrate for both cytochrome P-450 3A4 and P-glycoprotein, and potential drug interactions with concurrent medication should be kept in mind.
With regard to infections during receipt of sirolimus, in a systemic review and meta-analysis of 33 randomized trials, no difference in CMV infection/disease was noted between mTOR inhibitors, primarily sirolimus, and calcineurin inhibitors while mTOR inhibitor recipients had a lower risk for CMV infection/disease than antimetabolites recipients (71). In an analysis of 32,757 primary renal transplant recipients without prophylaxis information, maintenance immunosuppression with sirolimus as part of the regimen was associated with development of PCP (45). In addition, an outbreak of PCP in recipients without PCP prophylaxis has been reported in a phase II trial of sirolimus, steroid and cyclosporine (26).
Sirolimus also has potent antifungal activity against C. neoformans and Candida species by inhibiting their TORC1 homolog. while conflicting data exist regarding its activity against Aspergillus species (62). When sirolimus is combined with caspofungin, synergism against Aspergillus species was observed (28).
![]()
REFERENCEs
1. Alcaide ML, Abbo L, Pano JR, Gaynor JJ, Tryphonopoulos P, Weppler D, et al. Herpes zoster infection after liver transplantation in patients receiving induction therapy with alemtuzumab. Clin Transplant. 2008 Jul-Aug;22(4):502-7. [PubMed]
2. Allison AC, Eugui EM. Mycophenolate mofetil and its mechanisms of action. Immunopharmacology. 2000 May;47(2-3):85-118. [PubMed]
3. Allison AC, Eugui EM. Mechanisms of action of mycophenolate mofetil in preventing acute and chronic allograft rejection. Transplantation. 2005 Oct 15;80(2 Suppl):S181-90. [PubMed]
4. Barton TD, Blumberg EA, Doyle A, Ahya VN, Ferrenberg JM, Brozena SC, et al. A prospective cross-sectional study of BK virus infection in non-renal solid organ transplant recipients with chronic renal dysfunction. Transpl Infect Dis. 2006 Jun;8(2):102-7. [PubMed]
5. Binet I, Nickeleit V, Hirsch HH, Prince O, Dalquen P, Gudat F, et al. Polyomavirus disease under new immunosuppressive drugs: a cause of renal graft dysfunction and graft loss. Transplantation. 1999 Mar 27;67(6):918-22. [PubMed]
6. Brennan DC, Daller JA, Lake KD, Cibrik D, Del Castillo D. Rabbit antithymocyte globulin versus basiliximab in renal transplantation. N Engl J Med. 2006 Nov 9;355(19):1967-77. [PubMed]
7. Cantarovich D, Karam G, Giral-Classe M, Hourmant M, Dantal J, Blancho G, et al. Randomized comparison of triple therapy and antithymocyte globulin induction treatment after simultaneous pancreas-kidney transplantation. Kidney Int. 1998 Oct;54(4):1351-6. [PubMed]
8. Carlsen J, Johansen M, Boesgaard S, Andersen CB, Arendrup H, Aldershvilet J, et al. Induction therapy after cardiac transplantation: a comparison of anti-thymocyte globulin and daclizumab in the prevention of acute rejection. J Heart Lung Transplant. 2005 Mar;24(3):296-302. [PubMed]
9. Charpentier B, Rostaing L, Berthoux F, Lang P, Civati G, Touraine JL, et al. A three-arm study comparing immediate tacrolimus therapy with antithymocyte globulin induction therapy followed by tacrolimus or cyclosporine A in adult renal transplant recipients. Transplantation. 2003 Mar 27;75(6):844-51. [PubMed]
10. Ciancio G, Burke GW, Gaynor JJ, Roth D, Kupin W, Rosen A, et al. A randomized trial of thymoglobulin vs. alemtuzumab (with lower dose maintenance immunosuppression) vs. daclizumab in renal transplantation at 24 months of follow-up. Clin Transplant. 2008 Mar-Apr;22(2):200-10. [PubMed]
11. Cruz MC, Del Poeta M, Wang P, Wenger R, Zenke G, Quesniaux VF, et al. Immunosuppressive and nonimmunosuppressive cyclosporine analogs are toxic to the opportunistic fungal pathogen Cryptococcus neoformans via cyclophilin-dependent inhibition of calcineurin. Antimicrob Agents Chemother. 2000 Jan;44(1):143-9. [PubMed]
12. Dadhania D, Snopkowski C, Ding R, Muthukumar T, Chang C, Aull M, et al. Epidemiology of BK virus in renal allograft recipients: independent risk factors for BK virus replication. Transplantation. 2008 Aug 27;86(4):521-8. [PubMed]
13. Del Poeta M, Cruz MC, Cardenas ME, Perfect JR, Heitman J. Synergistic antifungal activities of bafilomycin A(1), fluconazole, and the pneumocandin MK-0991/caspofungin acetate (L-743,873) with calcineurin inhibitors FK506 and L-685,818 against Cryptococcus neoformans. Antimicrob Agents Chemother. 2000 Mar;44(3):739-46. [PubMed]
14. Dhesi S, Boland B, Colquhoun S. Alemtuzumab and liver transplantation: a review. Curr Opin Organ Transplant. 2009 Jun;14(3):245-9. [PubMed]
15. Flechner SM. Sirolimus in kidney transplantation indications and practical guidelines: de novo sirolimus-based therapy without calcineurin inhibitors. Transplantation. 2009 Apr 27;87(8 Suppl):S1-6. [PubMed]
16. Grim SA, Pham T, Thielke J, Sankary H, Oberholzer J, Benedetti E, et al. Infectious complications associated with the use of rituximab for ABO-incompatible and positive cross-match renal transplant recipients. Clin Transplant. 2007 Sep-Oct;21(5):628-32. [PubMed]
17. Gupta G, Shapiro R, Thai N, Randhawa PS, Vats A. Low incidence of BK virus nephropathy after simultaneous kidney pancreas transplantation. Transplantation. 2006 Aug 15;82(3):382-8. [PubMed]
18. Haddad EM, McAlister VC, Renouf E, Malthaner R, Kjaer MS, Gluud LL. Cyclosporin versus tacrolimus for liver transplanted patients. Cochrane Database Syst Rev. 2006(4):CD005161. [PubMed]
19. Halloran PF. Immunosuppressive drugs for kidney transplantation. N Engl J Med. 2004 Dec 23;351(26):2715-29. [PubMed]
20. Hershberger RE, Starling RC, Eisen HJ, Bergh CH, Kormos RL, Love RB, et al. Daclizumab to prevent rejection after cardiac transplantation. N Engl J Med. 2005 Jun 30;352(26):2705-13. [PubMed]
21. Husain S, Wagener MM, Singh N. Cryptococcus neoformans infection in organ transplant recipients: variables influencing clinical characteristics and outcome. Emerg Infect Dis. 2001 May-Jun;7(3):375-81. [PubMed]
22. Husain S, Singh N. The impact of novel immunosuppressive agents on infections in organ transplant recipients and the interactions of these agents with antimicrobials. Clin Infect Dis. 2002 Jul 1;35(1):53-61. [PubMed]
23. Ison MG, Parker M, Stosor V, Kaufman DB. Development of BK nephropathy in recipients of simultaneous pancreas-kidney transplantation. Transplantation. 2009 Feb 27;87(4):525-30. [PubMed]
24. Issa NC, Fishman JA. Infectious complications of antilymphocyte therapies in solid organ transplantation. Clin Infect Dis. 2009 Mar 15;48(6):772-86. [PubMed]
25. Iwatsuki S, Starzl TE, Todo S, Gordon RD, Esquivel CO, Tzakis AG, et al. Experience in 1,000 liver transplants under cyclosporine-steroid therapy: a survival report. Transplant Proc. 1988 Feb;20(1 Suppl 1):498-504. [PubMed]
26. Kahan BD, Julian BA, Pescovitz MD, Vanrenterghem Y, Neylan J. Sirolimus reduces the incidence of acute rejection episodes despite lower cyclosporine doses in caucasian recipients of mismatched primary renal allografts: a phase II trial. Rapamune Study Group. Transplantation. 1999 Nov 27;68(10):1526-32. [PubMed]
27. Kasiske BL, de Mattos A, Flechner SM, Gallon L, Meier-Kriesche HU, Weir MR, et al. Mammalian target of rapamycin inhibitor dyslipidemia in kidney transplant recipients. Am J Transplant. 2008 Jul;8(7):1384-92. [PubMed]
28. Kontoyiannis DP, Lewis RE, Osherov N, Albert ND, May GS. Combination of caspofungin with inhibitors of the calcineurin pathway attenuates growth in vitro in Aspergillus species. J Antimicrob Chemother. 2003 Feb;51(2):313-6. [PubMed]
29. Lebranchu Y, Bridoux F, Buchler M, Le Meur Y, Etienne I, Toupance O, et al. Immunoprophylaxis with basiliximab compared with antithymocyte globulin in renal transplant patients receiving MMF-containing triple therapy. Am J Transplant. 2002 Jan;2(1):48-56. [PubMed]
30. Magliocca JF, Odorico JS, Pirsch JD, Becker YT, Knechtle SJ, Leverson GE, et al. A comparison of alemtuzumab with basiliximab induction in simultaneous pancreas-kidney transplantation. Am J Transplant. 2008 Aug;8(8):1702-10. [PubMed]
31. Marcos A, Eghtesad B, Fung JJ, Fontes P, Patel K, Devera M, et al. Use of alemtuzumab and tacrolimus monotherapy for cadaveric liver transplantation: with particular reference to hepatitis C virus. Transplantation. 2004 Oct 15;78(7):966-71. [PubMed]
32. Martin SI, Marty FM, Fiumara K, Treon SP, Gribben JG, Baden LR. Infectious complications associated with alemtuzumab use for lymphoproliferative disorders. Clin Infect Dis. 2006 Jul 1;43(1):16-24. [PubMed]
33. Mattei MF, Redonnet M, Gandjbakhch I, Bandini AM, Billes A, Epailly E, et al. Lower risk of infectious deaths in cardiac transplant patients receiving basiliximab versus anti-thymocyte globulin as induction therapy. J Heart Lung Transplant. 2007 Jul;26(7):693-9. [PubMed]
34. McAlister VC, Haddad E, Renouf E, Malthaner RA, Kjaer MS, Gluud LL. Cyclosporin versus tacrolimus as primary immunosuppressant after liver transplantation: a meta-analysis. Am J Transplant. 2006 Jul;6(7):1578-85. [PubMed]
35. Meier-Kriesche HU, Schold JD, Srinivas TR, Kaplan B. Lack of improvement in renal allograft survival despite a marked decrease in acute rejection rates over the most recent era. Am J Transplant. 2004 Mar;4(3):378-83. [PubMed]
36. Mengel M, Marwedel M, Radermacher J, Eden G, Schwarz A, Haller H, et al. Incidence of polyomavirus-nephropathy in renal allografts: influence of modern immunosuppressive drugs. Nephrol Dial Transplant. 2003 Jun;18(6):1190-6. [PubMed]
37. Midtvedt K, Fauchald P, Lien B, Hartmann A, Albrechtsen D, Bjerkely BL, et al. Individualized T cell monitored administration of ATG versus OKT3 in steroid-resistant kidney graft rejection. Clin Transplant. 2003 Feb;17(1):69-74. [PubMed]
38. Moore J, Middleton L, Cockwell P, Adu D, Ball S, Little MA, et al. Calcineurin inhibitor sparing with mycophenolate in kidney transplantation: a systematic review and meta-analysis. Transplantation. 2009 Feb 27;87(4):591-605. [PubMed]
39. Mourad G, Garrigue V, Squifflet JP, Besse T, Berthoux F, Alamartine E, et al. Induction versus noninduction in renal transplant recipients with tacrolimus-based immunosuppression. Transplantation. 2001 Sep 27;72(6):1050-5. [PubMed]
40. Muthusamy AS, Vaidya AC, Sinha S, Roy D, Elker DE, Friend PJ. Alemtuzumab induction and steroid-free maintenance immunosuppression in pancreas transplantation. Am J Transplant. 2008 Oct;8(10):2126-31. [PubMed]
41. Morris PJ, Russell NK. Alemtuzumab (Campath-1H): a systematic review in organ transplantation. Transplantation. 2006 May 27;81(10):1361-7. [PubMed]
42. Nair S, Loss GE, Cohen AJ, Eason JD. Induction with rabbit antithymocyte globulin versus induction with corticosteroids in liver transplantation: impact on recurrent hepatitis C virus infection. Transplantation. 2006 Feb 27;81(4):620-2. [PubMed]
43. Nashan B, Moore R, Amlot P, Schmidt AG, Abeywickrama K, Soulillou JP. Randomised trial of basiliximab versus placebo for control of acute cellular rejection in renal allograft recipients. CHIB 201 International Study Group. Lancet. 1997 Oct 25;350(9086):1193-8. [PubMed]
44. Nath DS, Kandaswamy R, Gruessner R, Sutherland DE, Dunn DL, Humar A. Fungal infections in transplant recipients receiving alemtuzumab. Transplant Proc. 2005 Mar;37(2):934-6. [PubMed]
45. Neff RT, Jindal RM, Yoo DY, Hurst FP, Agodoa LY, Abbott KC. Analysis of USRDS: incidence and risk factors for Pneumocystis jiroveci pneumonia. Transplantation. 2009 Jul 15;88(1):135-41. [PubMed]
46. Nishida H, Ishida H, Tanaka T, Amano H, Omoto K, Shirakawa H, et al. Cytomegalovirus infection following renal transplantation in patients administered low-dose rituximab induction therapy. Transpl Int. 2009 Oct;22(10):961-9. [PubMed]
47. O'Brien S, Ravandi F, Riehl T, Wierda W, Huang X, Tarrand J, et al. Valganciclovir prevents cytomegalovirus reactivation in patients receiving alemtuzumab-based therapy. Blood. 2008 Feb 15;111(4):1816-9. [PubMed]
48. Peleg AY, Husain S, Kwak EJ, Silveira FP, Ndirangu M, Tran J, et al. Opportunistic infections in 547 organ transplant recipients receiving alemtuzumab, a humanized monoclonal CD-52 antibody. Clin Infect Dis. 2007 Jan 15;44(2):204-12. [PubMed]
49. Peleg AY, Husain S, Qureshi ZA, Silveira FP, Sarumi M, Shutt KA, et al. Risk factors, clinical characteristics, and outcome of Nocardia infection in organ transplant recipients: a matched case-control study. Clin Infect Dis. 2007 May 15;44(10):1307-14. [PubMed]
50. Perfect JR, Durack DT. Effects of cyclosporine in experimental cryptococcal meningitis. Infect Immun. 1985 Oct;50(1):22-6. [PubMed]
51. Ritter ML, Pirofski L. Mycophenolate mofetil: effects on cellular immune subsets, infectious complications, and antimicrobial activity. Transpl Infect Dis. 2009 Aug;11(4):290-7. [PubMed]
52. Saemann MD, Haidinger M, Hecking M, Horl WH, Weichhart T. The multifunctional role of mTOR in innate immunity: implications for transplant immunity. Am J Transplant. 2009 Dec;9(12):2655-61. [PubMed]
53. Salliot C, Dougados M, Gossec L. Risk of serious infections during rituximab, abatacept and anakinra treatments for rheumatoid arthritis: meta-analyses of randomised placebo-controlled trials. Ann Rheum Dis. 2009 Jan;68(1):25-32. [PubMed]
54. Schold JD, Rehman S, Kayle LK, Magliocca J, Srinivas TR, Meier-Kriesche HU. Treatment for BK virus: incidence, risk factors and outcomes for kidney transplant recipients in the United States. Transpl Int. 2009 Jun;22(6):626-34. [PubMed]
55. Shi Y, Moriyama T, Namba Y, Yamanaka M, Hanafuse T, Imamura R, et al. Association of treatment with 15-deoxyspergualin and BK virus nephropathy in kidney allograft recipients. Clin Transplant. 2007 Jul-Aug;21(4):502-9. [PubMed]
56. Shapiro R, Ellis D, Tan HP, Moritz ML, Basu A, Vats AN, et al. Alemtuzumab pre-conditioning with tacrolimus monotherapy in pediatric renal transplantation. Am J Transplant. 2007 Dec;7(12):2736-8. [PubMed]
57. Silveira FP, Husain S, Kwak EJ, Linden PK, Marcos A, Shapiro R, et al. Cryptococcosis in liver and kidney transplant recipients receiving anti-thymocyte globulin or alemtuzumab. Transpl Infect Dis. 2007 Mar;9(1):22-7. [PubMed]
58. Silveira FP, Marcos A, Kwak EJ, Husain S, Shapiro R, Thai N, et al. Bloodstream infections in organ transplant recipients receiving alemtuzumab: no evidence of occurrence of organisms typically associated with profound T cell depletion. J Infect. 2006 Oct;53(4):241-7. [PubMed]
59. Singh N, Aguado JM, Bonatti H, Forrest G, Gupta KL, Safdar N, et al. Zygomycosis in solid organ transplant recipients: a prospective, matched case-control study to assess risks for disease and outcome. J Infect Dis. 2009 Sep 15;200(6):1002-11. [PubMed]
60. Singh N, Alexander BD, Lortholary O, Dromer F, Gupta KL, John GT, et al. Cryptococcus neoformans in organ transplant recipients: impact of calcineurin-inhibitor agents on mortality. J Infect Dis. 2007 Mar 1;195(5):756-64. [PubMed]
61. Singh N. Infectious complications in organ transplant recipients with the use of calcineurin-inhibitor agent-based immunosuppressive regimens. Curr Opin Infect Dis. 2005 Aug;18(4):342-5. [PubMed]
62. Singh N, Heitman J. Antifungal attributes of immunosuppressive agents: new paradigms in management and elucidating the pathophysiologic basis of opportunistic mycoses in organ transplant recipients. Transplantation. 2004 Mar 27;77(6):795-800. [PubMed]
63. Soliman T, Hetz H, Burghuber C, Gyori G, Silberhumer G, Steininger R, et al. Short-term versus long-term induction therapy with antithymocyte globulin in orthotopic liver transplantation. Transpl Int. 2007 May;20(5):447-52. [PubMed]
64. Soliman T, Hetz H, Burghuber C, Gyori G, Silberhumer G, Steininger R, et al. Short-term induction therapy with anti-thymocyte globulin and delayed use of calcineurin inhibitors in orthotopic liver transplantation. Liver Transpl. 2007 Jul;13(7):1039-44. [PubMed]
65. Stallone G, Infante B, Grandaliano G, Gesualdo L. Management of side effects of sirolimus therapy. Transplantation. 2009 Apr 27;87(8 Suppl):S23-6. [PubMed]
66. Steinbach WJ, Reedy JL, Cramer RA, Jr., Perfect JR, Heitman J. Harnessing calcineurin as a novel anti-infective agent against invasive fungal infections. Nat Rev Microbiol. 2007 Jun;5(6):418-30. [PubMed]
67. Tector AJ, Fridell JA, Mangus RS, Shah A, Milgrom M, Kwo P, et al. Promising early results with immunosuppression using rabbit anti-thymocyte globulin and steroids with delayed introduction of tacrolimus in adult liver transplant recipients. Liver Transpl. 2004 Mar;10(3):404-7. [PubMed]
68. Tsutsumi Y, Kanamori H, Mori A, Tanaka J, Asaka M, Imamura M, et al. Reactivation of hepatitis B virus with rituximab. Expert Opin Drug Saf. 2005 May;4(3):599-608. [PubMed]
69. Tyden G, Genberg H, Tollemar J, Ekberg H, Persson NH, Tufveson G, et al. A randomized, doubleblind, placebo-controlled, study of single-dose rituximab as induction in renal transplantation. Transplantation. 2009 May 15;87(9):1325-9. [PubMed]
70. Vianna RM, Mangus RS, Fridell JA, Weigman S, Kazimi M, Tector J. Induction immunosuppression with thymoglobulin and rituximab in intestinal and multivisceral transplantation. Transplantation. 2008 May 15;85(9):1290-3. [PubMed]
71. Webster AC, Lee VW, Chapman JR, Craig JC. Target of rapamycin inhibitors (sirolimus and everolimus) for primary immunosuppression of kidney transplant recipients: a systematic review and meta-analysis of randomized trials. Transplantation. 2006 May 15;81(9):1234-48. [PubMed]
72. Zarkhin V, Li L, Kambham N, Sigdel T, Salvatierra O, Sarwal MM. A randomized, prospective trial of rituximab for acute rejection in pediatric renal transplantation. Am J Transplant. 2008 Dec;8(12):2607-17. [PubMed]
Table 1: Opportunistic Infections (OIs) Among the 547 Organ Transplant Recipients Who Received 1 Dose of Alemtuzumab from September 2002 through March 2004 (48)
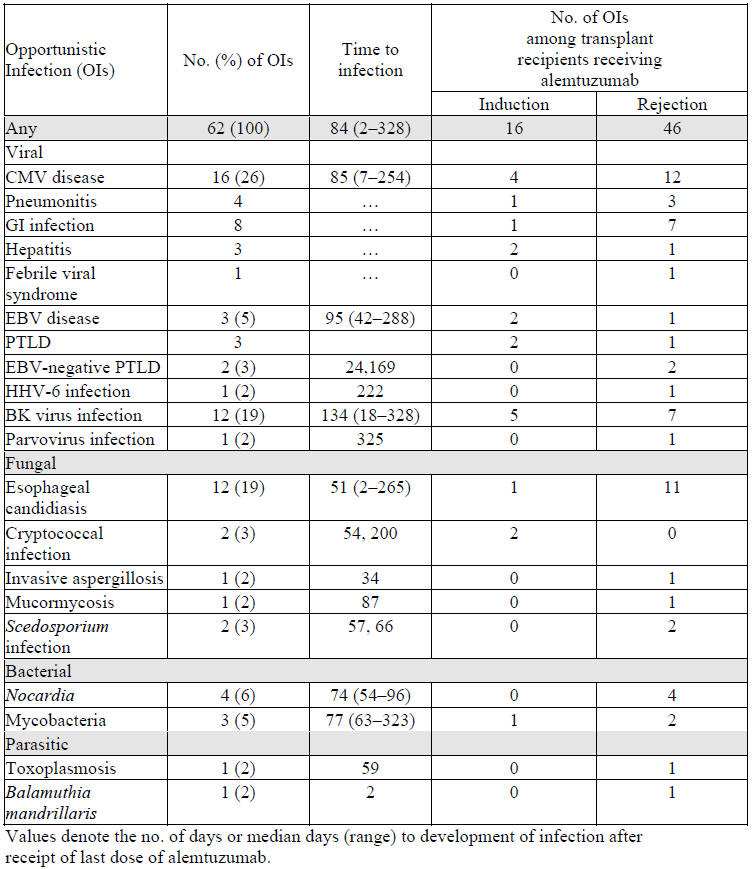
Table 2: Overview of the Infectious Complications of Alemtuzumab
| Risk | Impact on Prophylaxis | Impact on Laboratory Monitoring | |
|---|---|---|---|
| Bacterial Infections | No increased risk including Streptococcus, Listeria, Nocardia or MAC (common pathogens in AIDS) (49, 57) | None | Aggressive microbiologic evaluation for febrile transplant recipients who have received ATG |
| BK Virus | Increased risk as compared to IL-2R antagonists or no induction (17) but similar to ATG (23) | N/A | Consider more frequent screening (monthly rather than quarterly) |
| CMV | Increased risk as compared to IL-2R antagonists (48) but likely similar to ATG | Consider extended prophylaxis to 6 months, especially in D+/R-. Failure of prophylaxis has been reported | Consider either prolonged preemptive protocols or screening for reactivation after completion of prophylaxis |
| EBV / PTLD | Likely increased risk but data is mixed and long term data lacking | None | EBV donor + /recipient – patients should be screened for EBV infection |
| Fungal Infections | No increased risk when used for induction, significant increased risk when used for rejection. | If exposure to endemic fungi, prophylaxis for 6-12 months is indicated | If exposure to endemic fungus, routine screening likely indicated |
| HSV/HZV | Increased | Adequately covered by CMV prophylaxis or acyclovir derivatives if not on CMV prophylaxis | None |
| HCV/HBV | No benefit over conventional induction treatment for liver transplant with potential for increased complications including systemic infection (31) | N/A for HCV, Follow standard protocols for HBV prophylaxis | Consider routine viral load monitoring in known to have positive viremia.
Consider monitoring for reactivation of viremia in recipients with negative viral loads prior to transplant |
| Pneumocystis | Prolonged risk due to T-cell depletion | Minimum of 6-12 months of prophylaxis, consider more prolonged prophylaxis in heart and/or lung recipients | None |
Table 3: Overview of the Infectious Complications of Anti-Thymocyte Globulin (ATG)
| Risk | Impact on Prophylaxis | Impact on Laboratory Monitoring | |
|---|---|---|---|
| Bacterial Infections | Unclear impact | None | Aggressive microbiologic evaluation for febrile transplant recipients who have received ATG |
| BK Virus | Increased risk of infection especially with higher doses of ATG administration (54) | N/A | Consider more frequent screening (monthly rather than quarterly) |
| CMV | Increased risk of infection (9) | Consider extended prophylaxis to 6 months, especially in D+/R- | If preemptive protocol followed, consider extended duration of monitoring |
| EBV / PTLD | Possible increased risk, especially EBV D+/R-, though data is mixed (64) | None | Active screening for EBV viremia if EBV D+/R- |
| Fungal Infections | No increased risk during induction; Increased risk during rejection therapy | If exposure to endemic fungi, prophylaxis for 6-12 months is indicated | If exposure to endemic fungus, routine screening likely indicated |
| HCV/HBV | Accelerated HCV replication but no increased rate of hepatic graft injury (24)
No association with poor outcomes with HCV + renal transplant pts. |
N/A for HCV, Follow standard protocols for HBV prophylaxis | Consider routine viral load monitoring in known to have positive viremia.
Consider monitoring for reactivation of viremia in recipients with negative viral loads prior to transplant |
| HSV/HZV | Increased | Adequately covered by CMV prophylaxis or acyclovir derivatives if not on CMV prophylaxis | None |
| Pneumocystis | Increased risk of infection without appropriate prophylaxis (29) | Minimum of 6-12 months of prophylaxis, consider prolonged prophylaxis in heart and/or lung recipients | None |
Table 4: Overview of the Infectious Complications of IL-2 Receptor Antagonists
| Risk | Impact on Prophylaxis | Impact on Laboratory Monitoring | |
|---|---|---|---|
| Bacterial Infections | No increased risk during induction (29) | Standard prophylaxis | None |
| BK Virus | No increased risk | N/A | Standard BK screening protocols |
| CMV | No increased risk during induction (43, 20) increased risk compared to ATG during rejection therapy (6) | Standard prophylaxis or preemptive protocols | None |
| EBV / PTLD | No increased risk (43, 29) | N/A | Standard EBV screening protocols for EBV D+/R- SOT recipients |
| Fungal Infections | No increased risk (6) | None | None |
| HCV/HBV | Data is mixed, demonstrating both increased risk and no risk of recurrent HCV infection | N/A for HCV, Follow standard protocols for HBV prophylaxis | Standard monitoring |
| HSV/HZV | No increased risk | None | None |
| Pneumocystis | No increased risk (6, 8, 33) | Standard prophylaxis | N/A |
Table 5: Overview of the Infectious Complications of Rituximab
| Risk | Impact on Prophylaxis | Impact on Laboratory Monitoring | |
|---|---|---|---|
| Bacterial Infections | No increased risk (69) | None | None |
| BK Virus | No increased risk (69) | N/A | Standard monitoring (if indicated) |
| CMV | No increased risk compared to other regimens (69, 46) | Standard prophylaxis or preemptive therapy is required | None |
| EBV / PTLD | No increased risk, potentially protective (70) | None | None |
| Fungal Infections | Traditionally, no increased risk (69) though recent data somewhat conflicts (39) | None | None |
| HCV/HBV | Increased risk for HBV reactivation (68), lack of data regarding HCV | Consider HBV prophylaxis if evidence of chronic HBV infection (including core antibody positive) | Monitor for HBV reactivation if not taking prophylaxis and evidence of chronic HBV |
| HSV/HZV | No increased risk | None | None |
| Miscellaneous Infections | Increased risk for JC virus infection (cause of PML); No association with TB (53) | N/A | N/A |
| Pneumocystis | No increased risk (No impact on T cells) | Prophylaxis only if other high risk agents administered | None |
When rituximab is combined with ATG there appears to be an increased risk for infection related mortality.