Genital Ulcer Disease - Diagnosis
LABORATORY DIAGNOSIS
The laboratory diagnosis of genital ulcer disease may be problematic based upon the relative lack, and in some instances, the affordability of diagnostic tests. Combined with the relative insensitivity of those tests which are available, healthcare professionals often make therapeutic decisions centered upon the clinical presentation. However, the clinical diagnosis may not always reflect an accurate appraisal of the situation. Using this measure of diagnosis, various published reports have demonstrated successful treatments ranging from 22% to 82%, depending on the pathogen. Therefore, many organizations such as the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) endorse therapy based upon syndromic treatment, especially in resource limited situations.
Individuals with genital ulcer disease are usually keenly cognizant of their problem, but on occasion, may be unaware of the affliction. The approach to the patient with genital ulcer disease generally begins with historical information, and encompasses such items as a thorough sexual history, including high risk behaviors such as exposure to partners with known sexually transmitted infections or visible ulcer disease, exchange of sex for drugs or money, use of illicit drugs, same sex contacts, encounters with commercial sex workers, and lack of condom use. A previous history of STD’s is also beneficial information, as is HIV status, if known. A travel history may be particularly important during the evaluation as some ulcerative diseases of the genitalia are not routinely common in the United States. Moreover, having a sex partner from a developing country is essential information as well. A clearly delineated sequence of signs and symptoms related to the infection has to be detailed, including whether the ulcer is solitary or multiple, painful or painless, self-resolving or persistent, and whether or not there is accompanying inguinal lymphadenopathy. A careful examination of the genitalia, perineum and inguinal regions is mandatory. Once these items are completed, then a clinical impression is formulated. This process provides the format from which to proceed (Figure 1). It is important to note that when high suspicion exists for a particular diagnosis, then an option to begin presumptive therapy for that disease should be contemplated while awaiting confirmatory tests.
All patients who present with genital ulcer disease should have a basic laboratory examination for other STD’s, including tests for gonorrhea and chlamydia, with syphilis and HIV serology. Further laboratory examination is based upon the clinical presentation, and which tests are available to the clinician.
Figure 1: Approach to the Patient with Genital Ulcer Disease
Chancroid:
Chancroid is usually a diagnosis of exclusion, based upon the historical characteristics and clinical appearance of the ulcerative process. The definitive diagnosis requires the isolation of the causative organism on special media. This media, however, is not routinely available, and if used, only has a sensitivity of approximately 80%. The diagnostic material for culture is best removed from the base of a purulent ulcer, or from the aspiration of a suppurative lymph node, then applied to the special selective media. A Gram stain is not recommended of the material prior to culture, but if done, the classic “school of fish” pattern of gram-negative coccobacilli is seldom seen. No licensed PCR test exists for chancroid. Therefore, the final determination relies on high clinical suspicion with the presence of genital ulceration, and if present, the typical inguinal lymphadenopathy (which may or may not be suppurative), coupled with negative darkfield microscopy and serologic tests for syphilis, and the absence of multinucleated giant cells on ulcer preparation microscopy.
Clinical Manifestations of Chancroid
The incubation period is on average between 5 and 7 days. The initial pustular lesions often erode and become ulcerative. These ulcers may be multiple in numbers, painful, and non-indurated (unless secondarily infected. The most commonly involved sites in men are the glands, corona, or inner surface of the foreskin. For women, most lesions are located at the introitus or labia. Genital lesions may autoinoculate when the ulcer opposes onto the surrounding uninvolved skin or mucosal surfaces. These paired lesions are often referred to as “kissing lesions”. Inguinal lymphadenopathy is bilateral, tender, and found in nearly half of those who are infected with chancroid. The lymph nodes can suppurate and may develop into local buboes if treatment is either delayed or not prescribed.
Genital Herpes:
There is value in the type specific identification of the species of Herpes
simplex that causes genital disease: HSV-1 has fewer recurrences and less subclinical
shedding of virus than HSV-2. This is important information when counseling patients with
genital herpes. Though not FDA approved for routine use, and not universally
available, PCR assays have been employed for species identification. Otherwise,
routine viral culture is the standard method for isolating and determining the
species of the infecting strain of HSV. Type specific serology might be
beneficial to assist with the diagnosis of genital herpes in the patient who has
signs and symptoms of infection but negative HSV cultures; or in a patient
having a clinical diagnosis without laboratory confirmation; or a patient who
has a partner with genital herpes. Screening of the general population for HSV
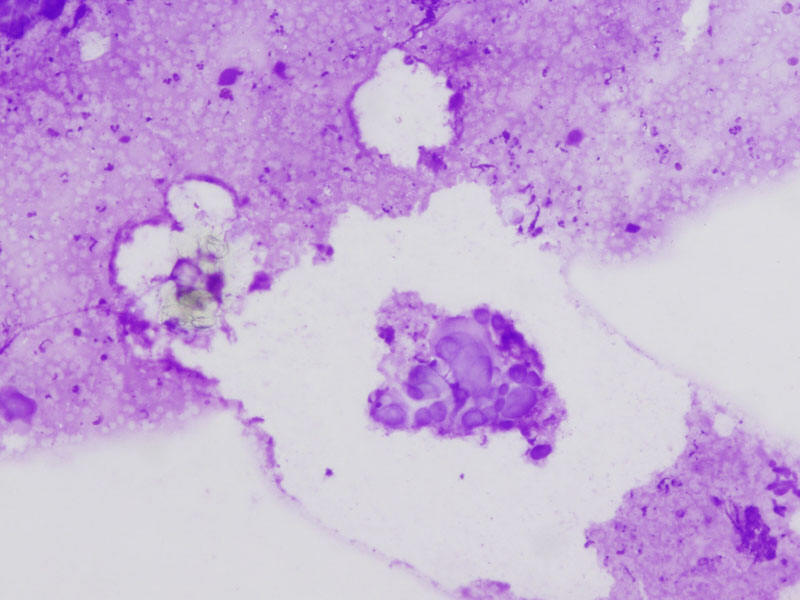
with serology is neither prudent nor practical. Basic microscopy revealing
multinucleated giant cells
![]() begins the diagnosis of HSV. Cell culture growth of
the virus is the preferred method to confirm the diagnosis, but is not routinely
performed. The clinical scenario is relatively distinct, and combined with the
microscopy results, the diagnosis is usually solidified. Although not approved
for testing of genital specimens, HSV PCR testing is used for spinal fluid
analysis for central nervous system HSV infection.
begins the diagnosis of HSV. Cell culture growth of
the virus is the preferred method to confirm the diagnosis, but is not routinely
performed. The clinical scenario is relatively distinct, and combined with the
microscopy results, the diagnosis is usually solidified. Although not approved
for testing of genital specimens, HSV PCR testing is used for spinal fluid
analysis for central nervous system HSV infection.
Multinucleated giant cell associated with herpes simplex.
Clinical Manifestations of Genital Herpes
Infection with herpes simplex virus infection is lifelong and recurrent, with time intervals between recurrences as variable as monthly to once per year. Classically, the primary infection is worst in terms of number of lesions and severity of pain. Many genital herpes cases are subclinical, while some individuals may have mild or unrecognized symptoms, and thusly remain undiagnosed. Transmission of the disease occurs with shedding of the virus with active lesions, although despite asymptomatic periods, virus shedding still may occur and transmission proceeds. The incubation period is on average between 2 and 7 days. The lesions are multiple, begin as papules, become vesicles, form pustules, then unroof and ulcerate. A crust over the lesions signals not only the termination of the episode, but the end of the highly transmissible period. Often times the appearance of the papules is heralded by a painful sensation at the affected location, described as a tingling or sun burn-like sensation. Women frequently have erosive cervicitis in addition to the external lesions, while men may have dysuria and urethritis-like complaints in addition to their ulcers. With viremia a component in the pathophysiology of the primary herpes simplex virus infection, nonspecific complaints of fever, malaise, headache and photophobia may be documented. On occasion, neuropathic symptoms such as urinary retention, constipation and pelvic paresthesias are manifest, and are related to the viral involvement of the sacral nerve roots where the infection is centered. Lymphadenopathy, when present, is usually bilateral, firm and tender, but not suppurative.
Granuloma Inguinale:
No culture, serologic, or genetic testing currently exists, thus transforming this diagnosis into one of equal parts high suspicion and exclusion of other entities. The diagnosis is predicated upon the histologic identification of specific findings demonstrated via Wright or Giemsa stains that requires either biopsy or crush preparations of tissue. These findings are known as “Donovan bodies” (hence the name donovanosis) and are actually the micro-organism contained within vacuoles located within macrophages seen on microscopic examination. A negative evaluation for other genital ulcer diseases should precede biopsy of the ulcer.
Clinical Manifestations of Granuloma Inguinale
The incubation period ranges from 1 to 4 weeks after exposure, but symptoms may be delayed until 3 to 6 months later. The classic form is a nonpainful, indolent ulcer, sometimes multiple, occasionally destructive, and vascular in nature. The base of the ulcer is often described as “red and beefy”, and bleeds easily. In unusual circumstances, there may be systemic dissemination, often manifested by hepatic and osteolytic lesions. Three other clinical variants are described, including a verruciform or hypertrophic form; a necrotic form with extensive tissue destruction; and a sclerotic form with extensive fibrosis and stricture formation. There is no true lymph node involvement, but pseudobubo formation (granulomatous nodules in the inguinal region encompassing the skin and subcutaneous tissues) is routinely identified. Primary lesions occur solely on the genitals and perineum in 80%-90%. In men, the lesions are commonly found on the glans and prepuce of the penis, while in women, the labia is the most common site. When the fibrotic form of granuloma inguinale is present, it may be complicated by stenosis of the urethral, vaginal, and anal orifices, and genital deformation, including pseudoelephantisasis of the labia.
Lymphogranuloma Venereum:
The diagnosis is generally based upon clinical suspicion with the exclusion of other more common genital ulcerative diseases such as HSV, syphilis, and chancroid. There is no microscopic examination available to aid in the diagnosis, but cell culture and serology are supportive measures to establish the exact diagnosis. Testing for C trachomatis from clinical specimens via culture, direct immunofluorescence, or nucleic acid amplification tests may be employed if available. Specimens for testing should be obtained from the ulcer base or rectal lesions, although aspiration of lymph nodes may result in higher yields. Genotyping of C. trachomatis to differentiate lymphogranuloma venereum from non-lymphogranuloma venereum serotypes is not widely available. Complement fixation and immunofluorescent antibody serology may enhance the clinical diagnosis. Although these serologic tests may be the most readily available methodology, the delayed reporting renders this a confirmatory test, less useful in the acute setting.
Clinical Manifestations of Lymphogranuloma Venereum
The incubation period varies from 3 days to 6 weeks, but routinely averages between 1 and 3 weeks. Of all the ulcerative illnesses, lymphogranuloma venerum is the least likely to present with a genital ulcer. A single lesion is present, usually at the site of inoculation, often self-limited in expression, and may actually present as a papule rather than as an ulcer. The ulceration may be variable in nature, ranging from superficial to deep in depth, sometimes painful, occasionally firm. Many cases are subclinical or go unrecognized. The most common clinical manifestation, however, is enlarged tender unilateral inguinal and/or femoral lymphadenopathy, also know as buboes. When both lymph node chains are involved, they are separated by the inguinal ligament producing the “groove sign”. Although considered pathognomonic for lymphogranuloma venereum, it is found only in the minority of cases. The enlarged lymph nodes are often quite firm and tender, and may spontaneously rupture, forming draining sinuses. Repetitive aspiration may reduce the incidence of rupture and secondary bacterial infection. Proctocolitis and its accompanying symptoms may eventually follow rectal exposure or spread to the perineum via lymphatics from the cervix or vagina in women. Lymphogranuloma venereum is an otherwise invasive, progressive systemic infection, and if not treated early, severe complications are the rule. The genitoanorectal syndrome with its attendant problems are the result of lymphatic obstruction and fistulization, and may be the end stage of a previously unknown lymphogranuloma venereuminfection.
Syphilis:
The diagnosis of syphilis requires clinical decision making and diagnostic testing. If an ulcer is present and can be scraped, visualizing the spirochete by darkfield microscopy secures the diagnosis. Serologic testing then confirms the presence of syphilis. Direct fluorescent antibody (DFA) tests of exudates from the chancre may be a useful adjunct if darkfield microscopy is not available. Histologic examination of tissues either using silver stain or immunofluoresence markers may also be informative. It is immaterial what is seen on the darkfield exam, as nontreponemal testing is ordered for confirmation. Both the rapid plasma regain (RPR) test and the Venereal Disease Research Laboratory (VDRL) test are valid tests, with 70%-80% reactivity in primary syphilis. The antibody titers correlate with disease activity, and are used sequentially for monitoring purposes. They will revert to negative after appropriate treatment, although in some instances, these tests may reveal low titer positivity for prolonged time periods, a phenomenon known as the serofast reaction. The results from the RPR and VDRL are not interchangeable, and if done sequentially, they should be performed at the same reference laboratory.
The main objective of the treponemal tests is to confirm a positive nontreponemal serology. The majority of patients in whom the treponemal tests are positive will be so forever, although in some patients (15%-25%), they will revert to negative after several years following successful treatment. The Treponemal pallidum hemagglutination assay (TPHA, MHA-TP) and the fluorescent antibody absorbed (FTA-abs) test are positive approximately 75% of the time in primary syphilis. One test or the other is used to confirm a positive VDRL or RPR; they are not used to monitor disease activity, and rarely should they be repeated.
If the exudate or ulcer preparation is negative, then the evaluation is centered on the serologic testing for the disease. Once one of the nontreponemal tests (VDRL or RPR) is positive, a treponemal test (FTA-abs or TPHA or MHA-TP) should be positive before the diagnosis of syphilis can be established.
Clinical Manifestations of Syphilis
Syphilis has been nicknamed the “Great Imitator” due to its protean manifestations which may mimic various medical disorders. Syphilis is a systemic illness, which if left untreated, will disseminate and manifest multiple phases of disease, each with separate and unique findings. The ulcer seen during the primary stage of infection is called a chancre, and is described as smooth edged, with a nonpurulent base, which may be indurated, but not painful. It is classically solitary. Cell mediated immunity plays an essential role in the host defense’s containment of the organism and the subsequent stages of infection it produces. The genital ulcer at the site of the inoculation is the prominent focus of the infectious process. It will spontaneously heal in 3 to 6 weeks without treatment. Many times the chancre will be inapparent due to its painless nature or because of an inaccessible location or both. It is not uncommon, once the chancre disappears or when symptoms resolve if the lesion is inapparent, for syphilis patients to proceed from the primary to the secondary stage. The net effect is spread throughout the body via the bloodstream, leading to the later stages of syphilis. Regional lymphadenopathy may occur in the primary stage but is more frequent in secondary syphilis. The chancre heals without scarring, although it may become secondarily infected and then have residual abnormalities. Multiple chancres have been documented in approximately 30% of cases. It is important to realize that atypical presentations and disease courses are relatively common. The spirochete also has a propensity to invade the central nervous system during the primary stage, occasionally manifesting as the aseptic meningitis syndrome.