
Candida species
Authors: John H. Rex, M.D., Jack D. Sobel, M.D., William Powderly, M.D.
MICROBIOLOGY
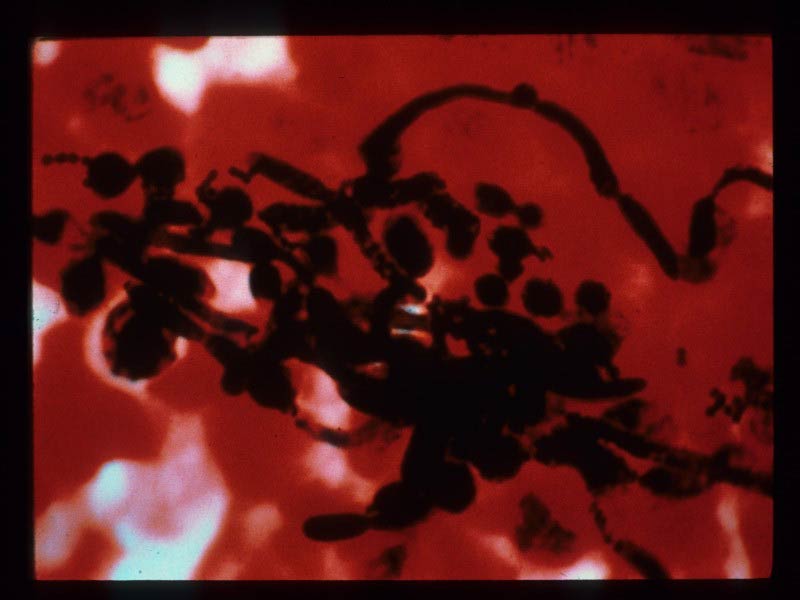
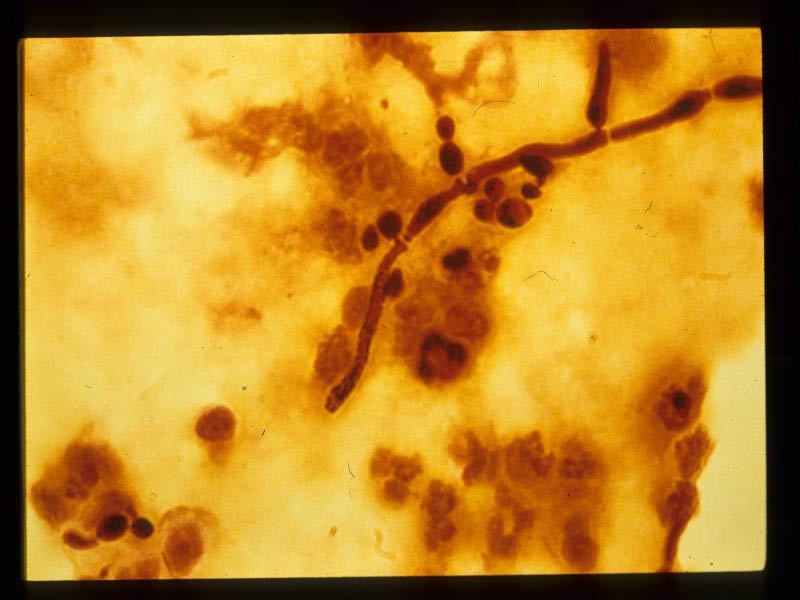
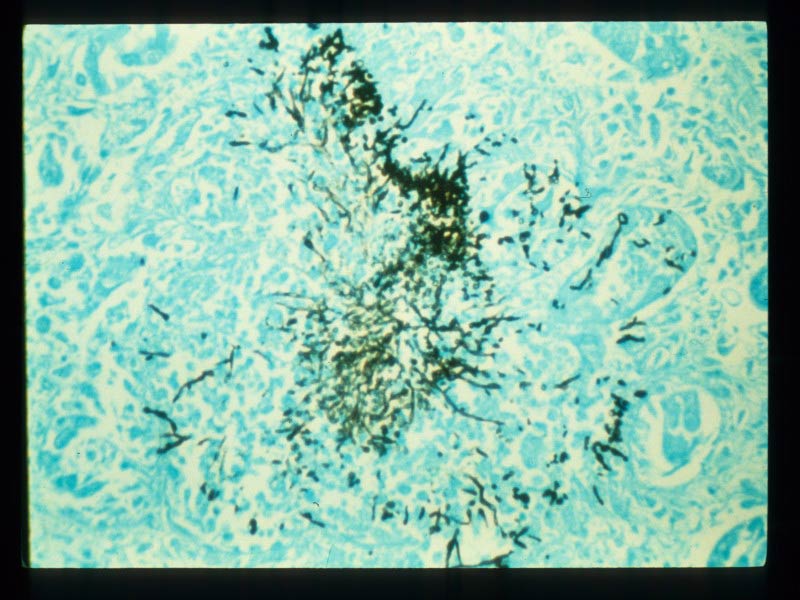
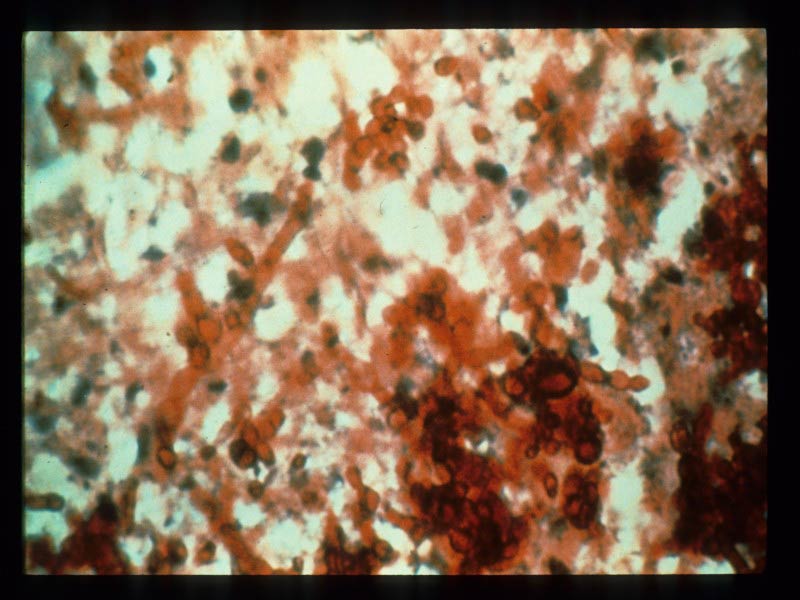
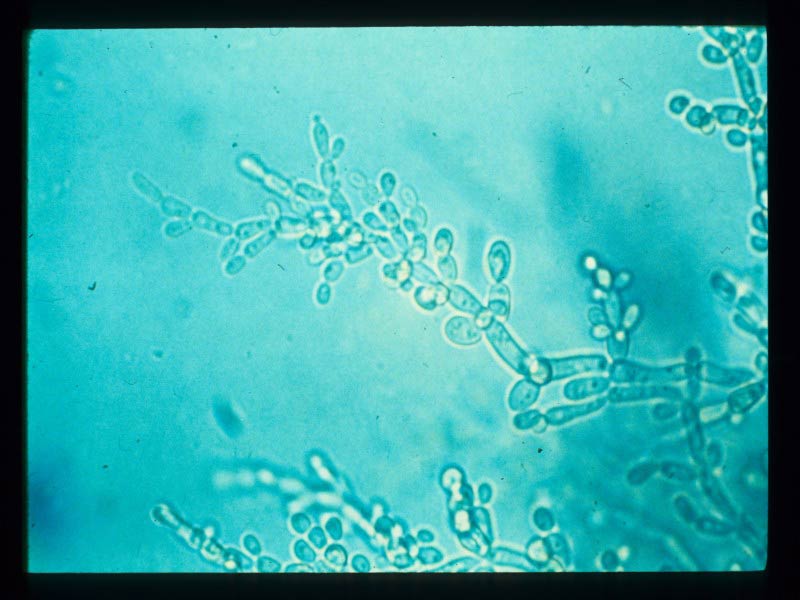
The genus Candida contains > 100 different species (380), but only a limited number of these species regularly cause disease in man (Table 1). Morphologically,Candida are 4-6 μm thin-walled yeast fungi that reproduce by budding. Candida can also produce hyphae and pseudohyphae in tissue , but this behavior is a function of both species and the involved organ. Identification of the individual species is based on standard sugar assimilation and morphological techniques. Of note, C. glabrata is the one species that does not produce hyphae or pseudohyphae and it has variously been considered to belong to the genus Candida and the genus Torulopsis (444). However, DNA-based data have placed this organism in the genus Candida (408).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
C. nivariensis, a species closely related to C. glabrata, has recently started to be reported as a cause of invasive candidiasis in Europe (86). Initial data suggest that it may be even more resistant to azole antifungals than C. glabrata. Awareness of less common species is driven by the ongoing broad epidemiological surveys now in constant application around the world.
EPIDEMIOLOGY
The major pathogenic species of Candida differ in their frequency, virulence, and clinical associations (Table 2). Recent surveys continue to support the long-established pattern of C. albicans as the most frequent cause of all forms of candidiasis (134, 531, 562, 565). It also generally appears to be the most virulent of the species and data suggesting a high rate of fungus-related mortality have been reported (531). However, data on invasive candidiasis from some (4, 454, 458, 496, 598, 609, 715, 821), but not all (377, 817) reports have documented a general reduction in the frequency of C. albicans associated with a concomitant increase in the frequency of C. glabrata, C. tropicalis, and C. parapsilosis infections (185, 562). This pattern of species shifts varies by region for unknown reasons (562). Overall, Candida spp. are typically among the five most common causes of bloodstream infections of hospitalized patients (50, 180, 562).
Of these major non-albicans species, C. tropicalis may be the most virulent. Colonization with this species often leads to invasive disease (361, 555, 823), and it appears to be especially able to colonize and infect gastrointestinal mucosa that has been compromised by neutropenia, chemotherapy-induced direct damage, and altered bacterial flora (791, 819, 820).
C. glabrata is either the first or second most common non-albicans species found in the blood (Table 2). As C. glabrata appears to have relatively low virulence (8,817), patients infected with it tend to be severely immunocompromised (8, 361) and infections due to this species have been associated with an increased mortality rate (774).
C. parapsilosis is the fourth most common Candida sp. found in the blood, and infections due to it are very strongly linked with the presence of intravenous catheters and other prosthetic devices (4, 238, 434, 801, 817). The organism’s propensity to grow in glucose-containing solutions such as those use for parenteral hyperalimentation (458, 574, 590, 801, 817), as well as its ability to form a slime that enhances adherence (94, 281, 574, 679) are probably responsible for these observed associations. C. parapsilosis has been thought to generally be less virulent than C. albicans (201, 305), was less often associated with septic shock than C. albicans in a study of fungemia (15), and has been associated with a lower mortality rate in cancer patients (774). However, isolates of C. parapsilosis demonstrate significant inter-isolate genetic differences (402,638) and a broad range of pathogenicity (113, 238). In addition, isolates colonizing the skin may differ in relative pathogenicity and mechanisms for invasion from those isolates found in the bloodstream (148). The cause(s) of the broad range of pathogenicity of this species are not fully understood, but the genetic heterogeneity among isolates is such that two new species, Candida orthopsilosis and Candida metapsilosis, have recently been proposed for less common two of the three major variants (739). In this proposal, the most common DNA variant will retain the name Candida parapsilosis. The relationship between these new species names and patterns of disease remains incompletely resolved.
C. krusei is the fifth most common species, and tends to be seen in relatively immunocompromised patients (247, 454).
C. lusitaniae is the sixth most common species. Like C. krusei it tends to be seen in relatively immunocompromised patients (77). C. dubliniensis was defined as a separate species in 1995 (735). Overall, this species is phenotypically very similar to C. albicans and specialized techniques are required for its definitive identification. Isolates of this species are usually susceptible to standard agents (470, 510, 573, 671). The species generally appears less virulent than C. albicans, it has been seen in pediatric patients as well as in adults (351), and it has been noted principally in the oropharynx of HIV-infected individuals—rates in the blood have typically been < 2% (540, 646, 671, 734). At present, there does not appear to significant clinical value in distinguishing therapy for this species sharply from the approaches taken to treat C. albicans.
C. nivariensis, a species closely related to C. glabrata, has recently started to be reported as a cause of invasive candidiasis in Europe (86). Initial data suggest that it may be even more resistant to azole antifungals than C. glabrata. Awareness of less common species is driven by the ongoing broad epidemiological surveys now in constant application around the world.
![]()
CLINICAL MANIFESTATIONS
The clinical manifestations of candidiasis are diverse. First, there are a number of localized syndromes that are widely appreciated. These include involvement of the mucosa with such syndromes as oropharyngeal candidiasis and genital candidiasis (especially vaginitis). Skin and nails may also be involved, thus giving rise to paronychia and involvement of the glabrous skin of areas that remain moist (the groin, peri-rectal region, and sometimes the axilla).
{kind=link}
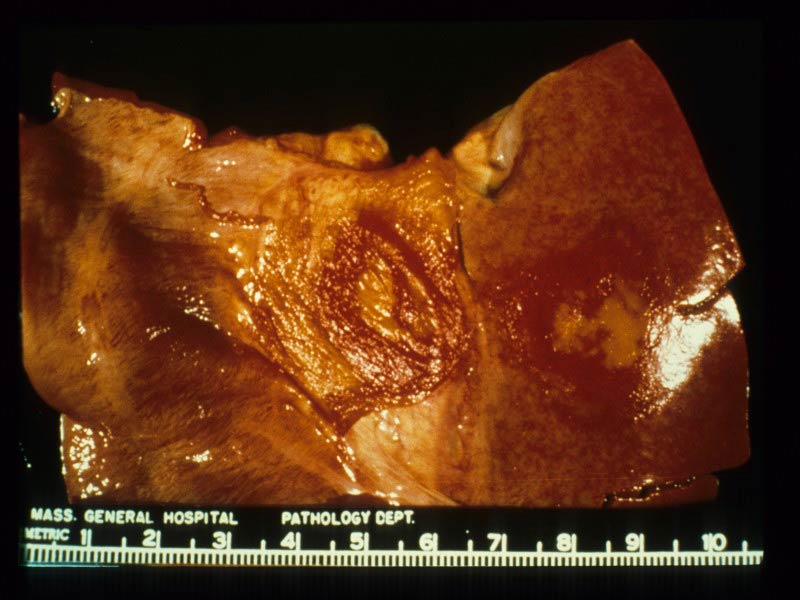
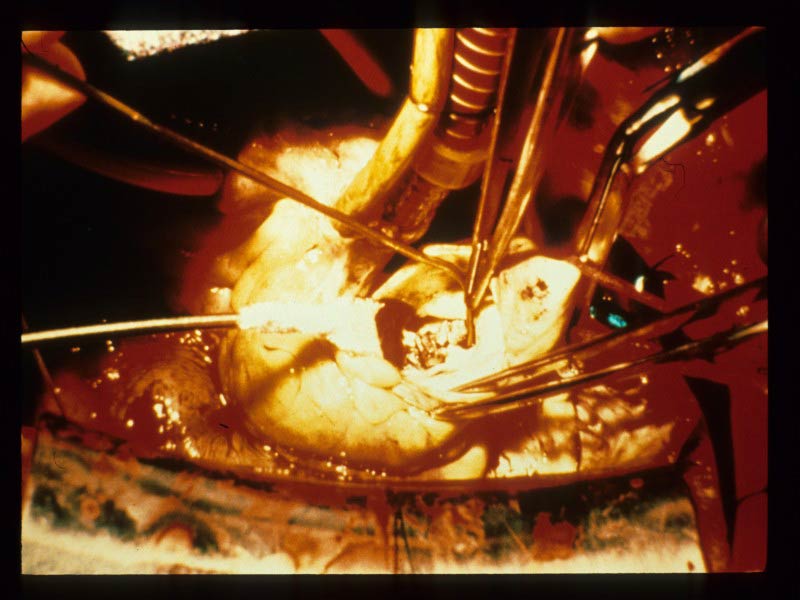
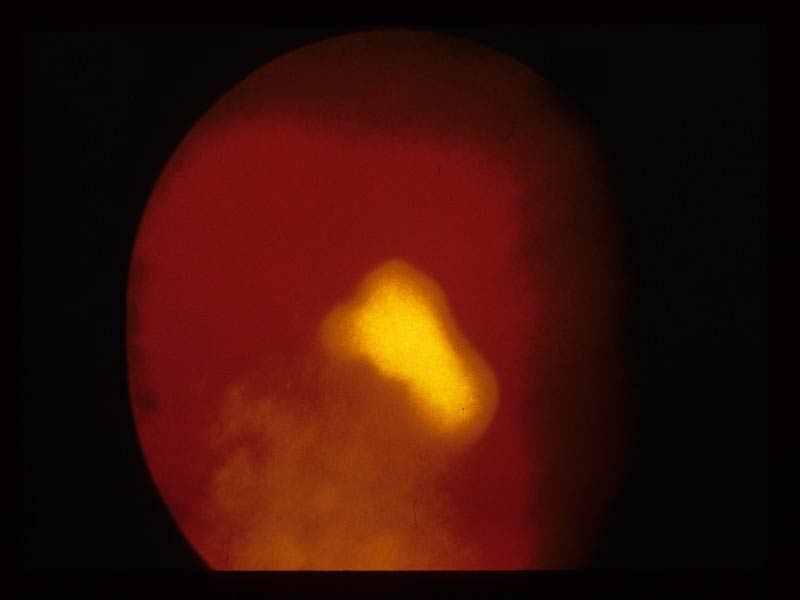
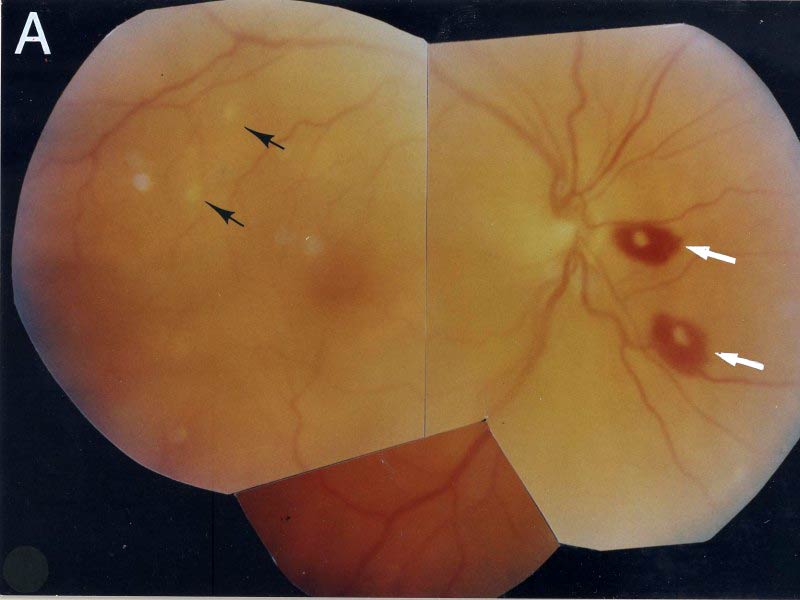
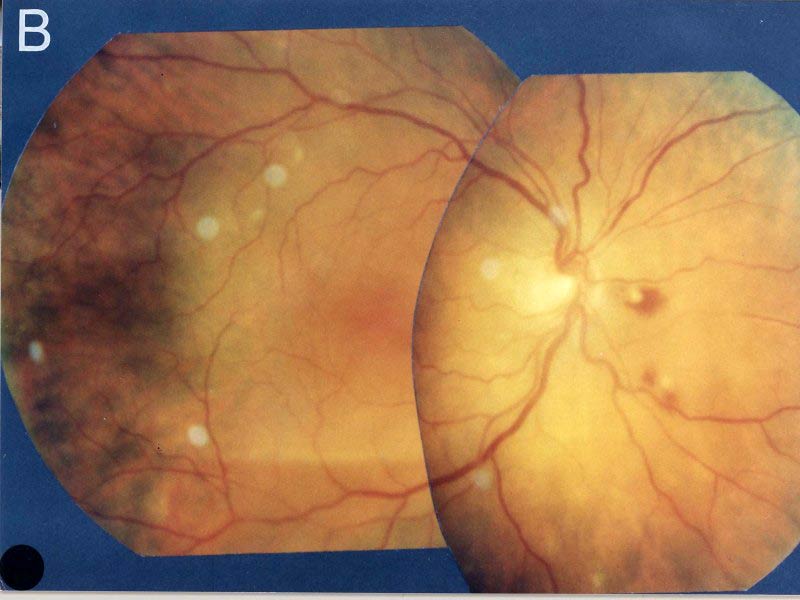
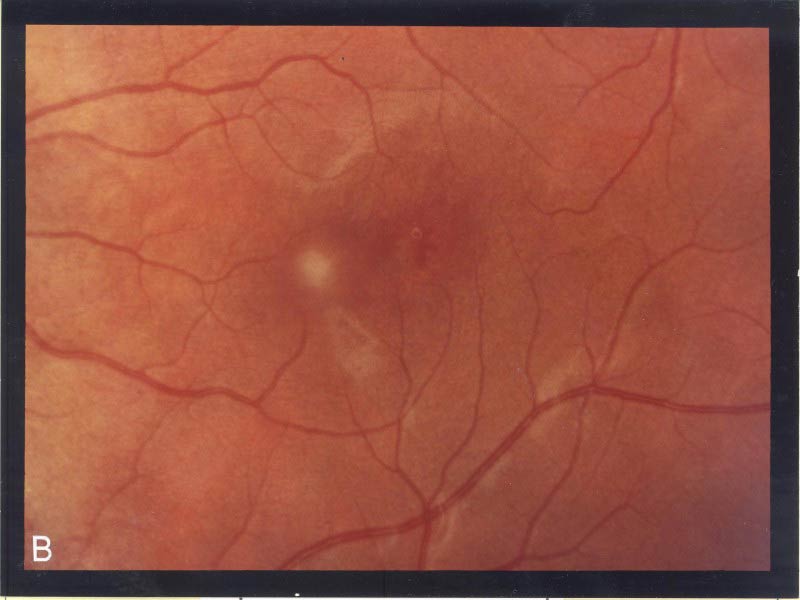
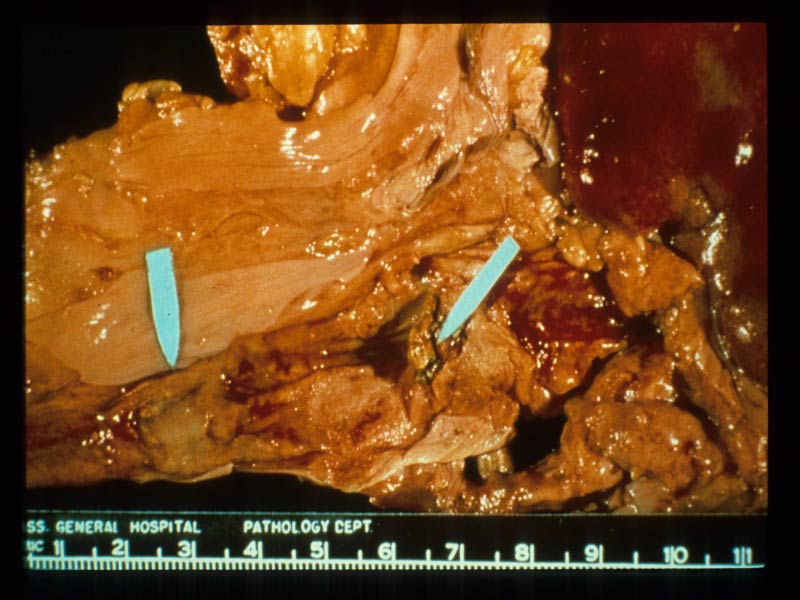
Quite distinct from these irritating but non-life-threatening forms are the various types of invasive candidiasis. The simplest of the syndromes is bloodstream infection or candidemia. From this start, Candida can spread to involve virtually any other organ: heart, eye (retina) , kidney, liver spleen, and bone are especially common. Local involvement with abscess formation is seen and can sometimes be seen without candidemia, especially when injury of the gut precedes formation of the abscess.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
LABORATORY DAIGNOSIS
Culture is the gold standard for the diagnosis of all forms of candidiasis. When culture of a non-sterile site is involved, it is important to remember that Candida spp. can also be surface colonizers. Thus, a report of growth of Candida spp. from skin or mucosa is only relevant if there is associated proof of disease based either on physical findings or microscopic examination of tissue.
Growth of Candida from a sterile specimen is almost always clinical relevant and should only rarely be ignored. Growth from the blood is the most common such report. In the case of candidemia specifically, it is also important to appreciate the role of intravascular catheters in the pathogenesis of candidemia (502, 794). In brief, it is generally believed that most episodes of Candida bloodstream infection begin with an organism that enters the blood via the gut. From this start, even a very minor episode of fungemia provides the organism with a chance to seed any intravascular catheter that happens to be present. An alternative source is contamination of the catheter hub during handling, and this may be especially common with C. parapsilosis due to its ability to adhere to the hands (304, 397, 411, 648). In either event, Candida spp., and especially C. parapsilosis, have a significant ability to adhere to plastic surfaces. The ability to adhere and form these biofilms does vary between species and between isolates of a given species (359, 679), but C. parapsilosis in particular appears to have a significant ability to form biofilms. Thus, the catheter may function as the nidus for a true endovascular source of the organism. Removal of intravascular catheters is often a helpful adjunct in therapy of candidal bloodstream infections.
Specifically with respect to invasive candidiasis, blood cultures remain the key to diagnosis. Automated systems make such cultures straightforward (302), but cultures are still slow and lack 100% sensitivity. It may be possible to reduce reporting time by use of PNA FISH for identification of Candida (including direct detection from blood culture bottles) (11, 222, 513, 607, 627, 678, 748, 815). Culture of the maximal possible volume does increase diagnostic yield (89) but is not always practical. Non-culture-based serodiagnostic tests have thus long been sought as alternatives (382). Selected tests such as assays for 1-3-D-ß-glucan (347, 503, 504, 674), PCR for candidal DNA (446,785), and detection of candidal metabolites (790) have shown promise. Among these, the detection of beta-glucan is most promising for Candida and commercial kits are available. Used serially in high-risk groups, beta-glucan testing does permit early and rapid case detection (504, 674) but it has yet to gain widespread use.
![]()
PATHOGENESIS
The current understanding of candidal virulence factors is generally limited. Aspartyl proteinases (149), phospholipases (312), phenotypic switching (713), and adherence and biofilm formation (117) are among the potential mechanisms used by these organisms (211, 547). The various species of Candida do differ in their apparent virulence, as this is discussed above under “Epidemiology.”
From a practical standpoint, cutaneous forms of candidiasis are generally precipitated by injury to glabrous skin (e.g., chronic moisture exposure of the groin) or loss of lymphocyte function (e.g., oropharyngeal candidiasis in late stage HIV infection). Invasive forms of candidiasis may be precipitated by injury to the bowel wall (e.g., surgery or chemotherapy-induced mucositis) or local structural damage (abscesses may occur at any site following injury and local inoculation). The potential role of intravascular catheters in propagating candidal bloodstream infections is discussed in the preceding section under “Laboratory Diagnosis.”
![]()
SUSCEPTIBILITY IN VITRO AND IN VIVO
Monotherapy
While additional agents with topical activity are available (see above), the principal licensed systemic agents with anti-Candida activity are amphotericin B, ketoconazole, itraconazole, fluconazole, voriconazole, caspofungin, micafungin, anidulafungin, and flucytosine (40). The activities of these agents against Candida are predictable and vary with species (Table 3 and Table 4). The drug of choice depends on the infecting species and the clinical setting. C. albicans isolates are the most susceptible to all of the antifungal agents. The pattern for C. tropicalis and C. parapsilosis is quite similar, with just slightly higher MICs for fluconazole. C. parapsilosis tends to have higher MICs for all of the echinocandin agents (378, 559, 564, 575) and there are reports from Africa and the Middle East of > 10% rates of flucaonzole & voriconazole resistance as well (564). C. glabrata tends to have fluconazole MICs that are 16–64-fold higher than those for C. albicans. C. krusei isolates tend to have higher azole MICs in general and definitely have the highest fluconazole and flucytosine MICs of any of the species, whereas C. lusitaniae isolates may have elevated amphotericin B MICs and failure of amphotericin B therapy is well described (463).
Among the less common species, reported data for C. dubliniensis generally suggest similar susceptibility to that for C. albicans for both azoles and echinocandins (520, 567). By contrast, C. guilliermondii tends to have higher MICs for both fluconazole and the echinocandins (520, 557, 558, 560, 566). Very high echinocandin MICs (e.g., caspofungin MIC > 2 micrograms/ml) are uncommon and voriconazole also appears generally reliable. As a further contrast, C. rugosa is frequently resistant to both fluconazole and voriconazole (563). In the reports that provide details on MICs of C. rugosa for the echinocandins, the small number of tested isolates had MICs in the presumed treatable range (520, 561).
Interpretation of the MIC results shown in Table 3 is controversial and remains the focus of intensive study (569, 570, 578, 618, 622). The principal difficulty is that MICs obtained in any in vitro system are arbitrary—variations in methodology can lead to 50,000-fold differences in measured MIC for the same isolate (621). This, along with the many non-drug-related causes of therapeutic failure (e.g., failure to remove a foreign body, drug-drug interactions (56), reduction in drug availability by protein binding, etc.) means that interpretation of MICs is not necessarily as simple as comparing achievable blood levels with measured MIC (620). While studies in animal models can be of some assistance in correlating MIC differences with therapeutic outcome, translation of these results into interpretive breakpoints ultimately requires examination of outcome in therapeutic trials in humans.
To address these overlapping concerns, the Clinical and Laboratory Standards Insititute (CLSI, formerly NCCLS or National Committee on Clinical Laboratory Standards) established a Subcommittee for Antifungal Susceptibility Testing in 1982. Over a many year period and in collaboration with numerous workers, a standardized and reproducible broth dilution method for susceptibility testing of Candida and Cryptococcus isolates has been developed. This method is known as CLSI M27 (130) and is currently in its third revision. The M27 method and the related CLSI M44 disk diffusion agar-based method (490) provide interpretive breakpoints for fluconazole, itraconazole, voriconazole, flucytosine, caspofungin, anidulafungin, and micafungin (568, 569, 618, 620). The details of these methods have been reviewed elsewhere (618, 621, 622). This method has now been used in a variety of efforts to correlate outcome with MIC (see below).
Based on an adaptation of the CLSI methodologies, the European Committee on Antimicrobial Susceptibility Testing (EUCAST) has separately developed a methodology for broth-based testing of yeasts (197). Interpretive breakpoint guidance released to date for the EUCAST method is limited to fluconazole (198, 631) & voriconazole (632). With small differences as MICs rise, this method generally gives similar fluconazole MICs to those produced by the CLSI M27 method (633). Confusingly, however, the interpretive breakpoints suggested for use with this method are meaningfully different from those recommended by CLSI and the guidance in particular excludes interpretation of results for C. glabrata and C. krusei. These points in turn lead to inconsistency with both US and EU labeling, especially for voriconazole. As the CLSI interpretive breakpoints (especially for fluconazole) are both consistent with US/EU labeling and are supported by a broad range of studies (46, 125, 392, 525, 569), the discussion below will focus on results and interpretations based on the CLSI methods unless otherwise stated.
The Azoles
The most extensive correlation data are available for fluconazole, itraconazole, voriconazole, and flucytosine vs. Candida—correlations for other organism-drug combinations are still under development. Approved interpretive breakpoints for these three drugs when tested by M27 are available and are summarized in Table 4. Table 5represents another way to summarize this information. The detailed rationale supporting the fluconazole, itraconazole, and voriconazole breakpoints has been described (569,618, 620). In addition, breakpoints are now available for the echinocandins (130).
While important advances, all breakpoints invited continued refinement. For fluconazole, the breakpoints were based substantially on experience with C. albicans in oropharyngeal candidiasis or in non-neutropenic patients with candidemia. Further, C. krusei is presumed to be intrinsically resistant to fluconazole, and its MICs should not be measured and or interpreted using this scale. Since their publication, the fluconazole breakpoints in particular have been supported by numerous additional clinical observations (29, 46, 125, 525) and pharmacodynamic studies (23, 618). The required fluconazole AUC/MIC ratios for efficacy are also consistent with recent observations on the pharmacodynamics of voriconazole (22) and other azoles (20, 21, 23, 525). For itraconazole, the breakpoints are based entirely on experience with a cyclodextrin-based solution in patients with oropharyngeal candidiasis. The voriconazole breakpoints are based almost entirely on invasive isolates drawn from a mixture of therapeutic studies. Although entirely consistent with with the predictable relationship of fluconazole and voriconazole MICs (572) as well as other available data across the azole class, the principal limitation of the voriconazole breakpoints is a lack of a clear dose-response curve.
For the azoles, the novel category S-DD implies that susceptibility is dependent on obtaining the maximal possible drug level. For fluconazole, this implies use of doses of > 400 mg/d in adults with normal renal function. For itraconazole it implies that measures must be taken to ensure that enough drug is absorbed to produce a measurable blood level, preferably one of least 0.5 μg/mL. And, for voriconazole it implies that maximal blood levels will be required—advancing the drug dosage to the maximum permitted may be required (e.g., from 200 mg q12h to 300 mg q12h PO in subjects weighing more than 40 kg). As discussed elsewhere in this chapter, blood level monitoring appears useful for both itraconazole and voriconazole.
Flucytosine
Large datasets correlating MIC with outcome are not available for flucytosine, and this situation is further complicated by the fact the drug is only rarely used as monotherapy. The interpretive breakpoints for this drug are based on a combination of historical and pharmacokinetic data (489). Isolates tend to have MICs < 0.5 μg/ml or > 64μg/ml, and this distribution of MICs has been shown by epidemiological studies to be a function of clade membership (599). The intermediate (I) category for this drug differs from the S-DD category for the other two drugs in the designation I implies that insufficient data exist to permit clear categorization of the isolates as either susceptible or resistant. Fortunately, such isolates are uncommon.
Amphotericin B
Measurement of meaningful amphotericin B MICs is problematic and the NCCLS M27 method is unable to reliably detect amphotericin B-resistant isolates (616). Modifications based on the use of Antibiotic Medium 3 (616) or measurements of minimum fungicidal concentrations (494) may help resolve this problem, but consistent demonstrations of clinical relevance for amphotericin B MICs have been elusive (534). The rate of killing by amphotericin B appears to vary by species (quickest with C. albicans, slowest with C. tropicalis and C. krusei) and incomplete killing at achievable serum levels is easily documented for some isolates (107). As a consequence of these complexities, additional work is still required before convincing breakpoints can be established. At present, the available data indicate that isolates with M27 amphotericin B MICs > 1 μg/mL are likely resistant to amphotericin B, but use of amphotericin B MICs for clinical guidance should be undertaken only with expert consultation.
Echinocandins
Interpretive criteria based on the CLSI testing procedure have been proposed for all 3 registered compounds (Table 4). Caspofungin shows higher MICs for some species in some surveys (520) than others (559), but this appears due to trailing effects and is eliminated by testing in the presence of serum (524). In practical terms, most isolates of most species appear likely to respond to achievable systemic exposures, no differences have been seen in practice in response across species, and the three currently available echinocandins should be considered therapeutic equivalents. Mechanisms of resistance are increasingly well understood (228, 550), and clinical resistance is associated with MIC of > 2 micrograms/ml for all three drugs (562). This has been noted in individual isolates of a variety of species with C. parapsilosis appearing most often problematic (140, 271, 289, 323, 338, 369, 387, 476, 535, 543).
Interpretation
Based on these breakpoints, the MICs in Table 3 can now be interpreted and Table 5 offers a brief summary. C. albicans, C. parapsilosis, C. tropicalis, and C. lusitaniae are generally quite susceptible to fluconazole, whereas isolates of C. glabrata typically have an MIC that places them in fluconazole’s S-DD category. For itraconazole, C. glabrata and C. krusei often have MICs in the S-DD category while the other major species are generally susceptible. Voriconazole has reliable in vitro activity for all species except C. glabrata. All species but C. krusei are generally susceptible to flucytosine. Resistance to the echinocandins appears rare.
![]()
Resistance to Antifungal Agents
Development of resistance to the azole antifungal agents is uncommon except during prolonged therapy of recurrent mucocutaneous disease in immunocompromised hosts and has been reviewed (623). A variety of mechanisms of resistance exist, with the most significant being those due to efflux pumps (35). Emergence of resistance during therapy in other settings appears uncommon (577) but has been infrequently described in settings other than HIV-infected patients (429, 472). Patients in cancer centers appear to be at greatest risk for infection with a resistant isolate from a normally susceptible species. For example, Antoniadou et al. (29) noted that 9% of bloodstream isolates of C. albicans were resistant with a fluconazole MIC > 64 micrograms/ml! Spontaneous fluconazole resistance in the absence of prior azole therapy has also been rarely described in one otherwise healthy adult, implying that the individual became primarily infected or colonized with a resistant organism (832). Approximately 50% of fluconazole-resistant isolates of Candida species (usually C. glabrata) are also resistant to voriconazole. Hence, fluconazole-resistant isolates are best treated with echinocandins since class cross-resistance is rare.
Resistance to amphotericin B is relatively uncommon (388), but has been described for all species. Resistance appears most frequently due to changes in the ergosterol content of the cell membrane, the sterol to which amphotericin B appears to bind (35). The most common situation in which amphotericin B resistance has been seen is in C. tropicalis, C. lusitaniae, C. parapsilosis, and C. glabrata isolates from immunocompromised patients treated extensively with amphotericin B (164, 173, 174, 263, 453, 455, 530,723). Resistance to amphotericin B appears to be especially common with C. lusitaniae (463). Importantly, resistance to the parent compound of amphotericin B implies that the isolate is also likely to be resistant to the newer lipid-based formulations of amphotericin B (337). Testing for susceptibility to amphotericin B should use amphotericin B itself, rather than a lipid-associated form of amphotericin B (737).
Intrinsic or primary resistance to flucytosine may be present in any species of Candida (727). More importantly, acquisition of resistance by susceptible isolates during flucytosine monotherapy is common and flucytosine should not be used as monotherapy for this reason (591).
An understanding of resistance to the echinocandins is now beginning to emerge from studies of caspofungin (550). Caspofungin MICs as measured by the NCCLS M27 methodology using a partial inhibition endpoint have been shown to correlate with clinical response (289, 509). Resistance appears to arise both from mutations in the gene of one of the components of glucan synthase gene (FKS1) (338, 378, 535, 550)) and from mutations in the sphingolipid pathway (337). The latter group of mutations is worrisome in that they appear to also reduce susceptibility to the azoles. As noted above, interpretive breakpoints have been proposed for this class of agents (568). Further work in this area is eagerly awaited.
Combination Therapy
Use of combinations of antifungal agents remains an area of significant controversy. Well validated clinically only for cryptococcal infection (672), clear clinical insight in other infections remains scant. For candidiasis, little support exists at present for routine use of any combination.
Amphotericin B With an Azole or With Flucytosine
Combinations of flucytosine with either amphotericin B or an azole have been used, and these combinations often appear to produce a positive effect, at least in vitro (65, 321, 592). While rational due to the different mechanisms of action of these drugs, the problems with flucytosine (lack of a widely available IV preparation and its potential toxicities) have lead to strong interest in combinations of amphotericin B with an azole. Unfortunately, the overlapping mechanisms of action of these agents raise the possibility of antagonism and the available information has not clarified the relevance of this theoretical possibility. Antagonism is definitely seen under some circumstances, especially when ketoconazole or itraconazole are combined with amphotericin B (660, 661, 663, 664, 665). In particular, pre-incubation of the fungus with the azole often raises the apparent MIC to amphotericin B. In addition, modest antagonism can be seen in vitro when the drugs are used simultaneously but both are at carefully selected sub-MIC concentrations (236). A review of this problem concluded that (a) interactions ranging from antagonism to synergy have been reported; (b) the interaction is dependent on the selected drugs, the target organism, and the precise experimental model; and thus (c) generalization of the available data to infections in man was not truly possible (731). This analysis was supported by subsequent extensive review of this topic (321).
Relevant to Candida infections, antagonism is not seen with simultaneous exposure in vitro or in vivo to therapeutic concentrations of both fluconazole and amphotericin B (236, 732). A trial tested this assertion by randomizing non-neutropenic adults with candidemia to receive either fluconazole alone (800 mg/day) or fluconazole plus amphotericin B (0.7 mg/kg/d) (617). The amphotericin B component was given for only the first 3-5 days of therapy whereas the fluconazole was continued for 14 days following resolution of signs and symptoms of infection. No evidence of antagonism was noted and the combination arm produced more rapid clearance of the bloodstream. The combination was, however, more nephrotoxic. The implications of this trial are still being debated (508), but a useful initial view is that the combination is analogous to the addition of aminoglycoside therapy to initial therapy for staphylococcal endocarditis in that it has toxicities but may also provide benefits.
Echinocandins with Either Azoles or Amphotericin B
There is no a priori reason why combinations of an echinocandin with either an azole or an amphotericin B would demonstrate either microbiological antagonism or a meaningful drug-drug pharmacokinetic interaction. Thus, their empirical use together to achieve an extended empirical spectrum is plausible. On the other hand, and unlike the situation for aspergillosis where some in vitro (34, 546), in vivo (128, 354, 552), and clinical (416, 428) data suggest the possibility of synergy, there are no data to indicate that the combination would be synergistic for candidal infections, hence combination therapy is rarely justified or indicated. For example, a murine study of fluconazole plus caspofungin vs. C. albicans demonstrated no benefit (253). This remains an area of significant debate (221, 467, 483).
![]()
Clinical Use of Antifungal Susceptibility Testing
Given the problematic nature of antifungal susceptibility testing, routine testing of all isolates is not indicated. Rather, the following approach has been suggested (576,618):
1. All Candida isolates from deep sources and any other isolates of clinical significance should be identified to the species level—this information alone is quite valuable given the usual susceptibilities of Candida species (Table 3). Identification of non-sterile site isolates to the species level can be quite helpful clinically and is especially recommended isolates from patients with recurrent or refractory disease of any type.
2. Periodic batch testing of hospital-acquired isolates could be used to establish a local antibiogram.
3. Testing of isolates from patients with oropharyngeal or vulvovaginal candidiasis refractory to standard doses of fluconazole can be used to differentiate true resistance from other causes of failure.
4. Testing of isolates from deep sites is generally advisable. This is particularly true if the infection fails to respond and in cases when there is a desire to switch from an IV-only agent (e.g., an echinocandin such as caspofungin). Interpretive breakpoints are now available for fluconazole, itraconazole, voriconazole, and flucytosine (Table 4). Testing against fluconazole and voriconazole will usually provide the greatest value. If resources are limited, determination of the fluconazole MIC alone provides insight into the likely susceptibility of the isolate to all currently available azole antifungal agents (fluconazole-resistant isolates are often resistant to the other azole antifungal agents). The use of this principle has been recently well demonstrated for fluconazole as a predictor of voriconazole susceptibility category (572).
![]()
ANTIMICROBIAL THERAPY
GENERAL
Choice of an antifungal agent for a given infection is based on integration of relative drug toxicity, patient status, and microbiological information. Several sets of summary recommendations are available (82, 159, 532). In this chapter, the available information for each particular clinical condition is summarized in the relevant discussion below. Common to all of the therapy discussions are a set of basic background ideas laid out in this introductory section.
Guidelines: Pappas PG, et al. Clinical Practice Guidelines for the Management of Candidiasis: 2009 Update by the Infectious Diseases Society of America. Clin Infect Dis 2009;48:503-535.
Amphotericin B and its Various Lipid-Associated Preparations
A great deal of confusion and lore exists surrounding amphotericin B deoxycholate (Fungizone™, the classic version in use for decades) and its lipid-associated preparations. A number of useful reviews are available (55, 518, 831). From a practical standpoint, the key issues may be summarized as:
1. There are three lipid-based preparations of amphotericin B. These are amphotericin B colloidal dispersion (ABCD, Amphotec, Amphocil), amphotericin B lipid complex (ABLC, Abelcet), and liposomal amphotericin B (AmBisome). Of these three, only the latter is a truly liposomal preparation—the other two have different physical constructions.
2. Because the phrase “liposomal amphotericin B” is so similar to “lipid-associated amphotericin B”, many physicians incorrectly use the two as synonyms. This error must be avoided as (a) the dosages different slightly across the preparations and (b) the side-effect profiles differ slightly. Patients who have accommodated to one preparation may demonstrate intolerance when switched to another preparation.
3. Both the deoxycholate and lipid-based derivatives of amphotericin B are similarly active against Candida (17, 55, 67, 127, 337, 493, 518), although higher doses of the lipid-based formations are required.
4. The toxicity profiles of amphotericin B lipid complex and liposomal amphotericin B are superior to that of amphotericin B colloidal dispersion and amphotericin B deoxycholate (55, 518, 831), with liposomal amphotericin B sometimes appearing least toxic overall (752).
In this text, data will always be discussed relative to the particular preparation under study. However, summary recommendations may at times refer to “any lipid-associated preparation of amphotericin B.” In such cases, any of the three are thought likely to be active. As noted above, two of the preparations are generally preferred on the grounds of better tolerability.
When writing orders for amphotericin B preparations, the above issues suggest that specification of preparation by trade name (Ambisome, Abelcet, or Fungizone) may avoid catastrophic dosing errors (465).
![]()
The Azoles
Four azoles have been licensed for use as systemic therapy of fungal infections: fluconazole, itraconazole, voriconazole, and (most recently) posaconazole (484). Of these, neither itraconazole nor posaconazole has been studied carefully and systematically for invasive candidiasis. Although there is little reason to doubt their potential activity, a clinical demonstration of activity serves to integrate and address convincingly such concerns as tissue penetration and protein binding. Further, posaconazole currently lacks an intravenous formulation and itraconazole has somewhat unpredictable human pharmacology. Thus, and because of the much stronger datasets for fluconazole and voriconazole, the use of itraconazole & posaconazole for serious candidal infections is less attractive and will be little discussed in this chapter. When voriconazole is used, monitoring of serum levels should be considered — see specific discussion of this agent in the section on Candidemia and Disseminated Candidiasis.
The Echinocandins
Three echinocandin agents are now currently licensed. Caspofungin has the largest dataset to support its role in the therapy of invasive candidiasis (30, 469, 771, 772,795), but convincing data are also available for anidulafungin (364, 365, 604). Data on micafungin are more limited (155, 156, 516, 640, 756) and the US FDA-approved indications for this compound are currently limited to esophageal candidiasis and prophylaxis of fungal infection in hematopoietic stem cell recipients. Reviews are available of all three drugs (64, 119, 474, 768). For all three, the bulk of the data are from studies of therapy of esophageal candidiasis or candidemia. But, a small number of cases of infection at other specific sites are also available for each compound. Overall, there appears to be very little difference in overall efficacy of the compounds.
Of increasing interest with all three echinocandins is the observation of lessened antimicrobial efficacy at very high concentrations, at least in vitro (265, 550, 712,809). This observation is often termed the “paradoxical effect” and may due to induction of escape mechanism involving increased chitin synthesis. Current therapeutic regimens produce exposures below those associated with this preclinical observation and a strong demonstration of the clinical consequences (if any) of this observation has not been reported.
Finally, there is a growing body of data suggesting that the mechanism of action of the echinocandins may lead to an enhanced immunologic response to the fungus (725). These intriguing observations do not yet have any practical clinical implications but may explain dichotomies in the ability of these agents to kill fungi in vitro vs. in vivo.
Flucytosine
Flucytosine has predictable activity for all species except C. krusei (571) but is only occasionally used at present to treat candidiasis. As resistance develops rapidly during monotherapy (591, 806), it is always given in combination with another agent. Historically dosed at 100–150 mg/kg/day in four divided doses, recent work suggests that 100 mg/kg/d is sufficient to produce a maximal microbiological effect (297) with levels of 10-50 mg/ml representing an adequate target (690).
Approaches to Therapy When Susceptibility Testing Data are Unavailable
As illustrated in Table 3 and Table 4, the likely pattern of susceptibility of a given isolate can be predicted on the basis of knowledge of its species. As the process of obtaining susceptibility testing may take several days, the usually more rapid process of identification to the species level is often used as a surrogate for susceptibility testing. Therapy recommendations in the sections that follow will handle the general case for most clinical situations, but refinements are possible based on the isolated species. For C. albicans, C. tropicalis, and C. parapsilosis, susceptibility to all drugs is the usual case and azoles (fluconazole), an echinocandin, and amphotericin B may all be used. For C. glabrata and C. krusei, fluconazole susceptibility is less certain (C. glabrata) or unlikely (C. krusei). Voriconazole is usually active vs. C. krusei but variable for C. glabrata (526).
Overall, an echinocandin or an amphotericin B preparation are considered the more reliable initial choices. Voriconazole’s position in this hierarchy is still evolving—whereas it did well against C. glabrata in a randomized candidemia study (372), the patients in that study were non-neutropenic and there have been anecdotal reports (314) of breakthrough infection with C. glabrata in neutropenic patients. These data, along with voriconazole’s significant drug-drug interaction issues and its inability to be dosed IV in severe renal failure generally make it less attractive. When the isolate is C. lusitaniae, amphotericin B susceptibility is less predictable and thus an azole (fluconazole or voriconazole) or an echinocandin would be considered as the more reliable initial choices. Likewise (although based on limited data), C. rugosa seems less likely to be susceptible to amphotericin B (133, 367) and may also often be resistant to both fluconazole and itraconazole (563), thus leaving an echinocandin as the best choice.
The final situation to occur is the one in which the isolate is only known to be a Candida species. The laboratory is usually able to quickly eliminate the possibility of C. albicans, but the specific non-albicans species is not known and will not be known for several days. In this case, one uses a combination of knowledge regarding frequency and susceptibility to make a decision. As C. lusitaniae is relatively uncommon, the primary concern is that the isolate might be C. glabrata. In this situation, an echinocandin or an amphotericin B would usually be most appropriate as initial therapy.
![]()
Antifungal Dosing in Renal Failure
Appropriate dosing of the antifungal agents in situations of reduced renal function has recently been reviewed in detail (478). The situation for each of the systemically active agents can be briefly summarized.
Based on their non-renal mode of clearance, amphotericin B and its lipid preparations require no dose adjustment for any degree of renal function. Of course, dose reduction might be undertaken to mitigate the potential of these agents to produce nephrotoxicity, but such dose reductions have the effect of reducing systemic exposure to the active agent.
The kidney clears fluconazole and its dose should be adjusted as renal function declines (141, 478). After administration of a loading dose, the full daily dose should be given daily if the creatinine clearance is > 50 ml/min and half the usual full daily dose should be given daily if the creatinine clearance is < 50 ml/min. Patients on intermittent hemodialysis should receive the full dose daily dose after each dialysis session. In patients on CAPD, fluconazole’s half-life increases from 30h to 72–85h (157). No single best regimen is appropriate; use of approximately half the full daily dose on a daily or every other day basis seems plausible. Continuous hemofiltration (CVVH and its variants) appears to clear fluconazole very rapidly (478, 482, 833). Aggressive dosing appears warranted and we would advise use of no less than 800 mg/day (12 mg/kg).
Both itraconazole and voriconazole are cleared largely by hepatic mechanisms and there is no need for dose adjustment of either for any degree of renal dysfunction. However, both do share a limitation on administration of their intravenous formulations in renal failure. Each uses a cyclodextrin carrier to permit intravenous therapy and the kidneys clear this carrier. Thus, administration of the IV formulation is not recommended if the creatinine clearance is < 30 ml/min and oral therapy in usual doses should be considered. If IV therapy were deemed necessary, a study of the IV formulation of itraconazole in hemodialysis patients suggests that administration of each dose just prior to a session of hemodialysis would permit adequate systemic levels of itraconazole while also permitting removal of the cyclodextrin carrier by the hemodialysis session (464). A small number of subjects with moderate renal impairment were reported to tolerate twice daily voriconazole for 7 days (3), with clearance of the carrier shown to be proportional to creatinine clearance. No adjustment of voriconazole dose appears necessary if it is used during continuous venovenous haemodiafiltration (225). Posaconazole is cleared via biliary excretion rather than either hepatic metabolism or renal excretion — dose adjustment is not needed for hepatic or renal insufficiency (485).
As a class, the echinocandins are cleared by non-renal mechanisms and require no dose adjustment for any degree of renal failure (171). They are not removed by dialysis and supplemental dosing is not required.
Like fluconazole, flucytosine is cleared by the kidneys. Due to the narrow therapeutic window of this compound, the best approach is to avoid its use in renal failure. If therapy is required in a patient with renal insufficiency, the dose should be reduced proportionally with renal function. Blood level monitoring is strongly recommended (716).
![]()
Antifungal Dosing for Candida Infections in Pregnancy
Vaginal candidiasis is reasonably common in pregnant women and the other candidal infections are seen on occasion. The topic azoles may be used safely for superficial infections. Systemic antifungal therapy, however, may be carefully chosen. Amphotericin B has been used many times during pregnancy, appears to free of adverse effects on the fetus, and has been placed by the US FDA in pregnancy category B (“No evidence of risk in humans”). Fluconazole, Itraconazole, ketoconazole, griseofulvin,caspofungin, micafungin, and anidulafungin are all assigned to pregnancy category C (“Risk cannot be ruled out”). Voriconazole is assigned to category D (“Positive evidence of risk”). A detailed recent review of this area (477) concluded that (a) amphotericin B-based preparations are the therapy of choice, (b) azoles overall demonstrate a dose-related risk of teratogenic effects, and (c) griseofulvin, ketoconazole, voriconazole, and flucytosine are definitely associated with serious risks of fetal malformation.
Antifungal Dosing for Candida Infections in Pediatrics
Appropriate dosing regimens in infants and children have been suggested based on pharmacokinetic data and a limited amount of clinical experience. Dosing regimens in neonates (78, 757, 836) and children (80, 527, 720, 837) have been reviewed.
Amphotericin B
The kinetics of amphotericin B in neonates appear similar to those in adults, and therapy with 0.5–1.0 mg/kg/d is usually well tolerated (757). Infants and children have long been thought to tolerate amphotericin B deoxycholate well, but recent data suggests >15% rates of meaningful nephrotoxicity (248). Safe use of ABLC (796) and liposomal amphotericin B (294, 328, 659) has been described in pediatric and neonatal populations.
Fluconazole
The pharmacokinetics of fluconazole have been studied in several groups of pediatric patients (93, 658, 670). In neonates in particular, the volume of distribution can 2–3 fold higher than the 0.7 L/kg figure for adults. However, volume of distribution is usually < 1 L/kg by three months of age. Clearance rates in children are both higher and lower than those seen in adults: neonates have a t½ of 55-90h, children above the age of 3 months have a t½ of 21–22h, and adults have a t½ of approximately 30 hours (252). Combining these data with the known progressive changes in renal function in newborns, these data suggest that daily doses roughly double those used in adults would be appropriate for most children older than 1 month of age. Neonates should be given this doubled dose every 72 hours during the first 1–2 weeks of life and every 48 hours during the remainder of the first month of life (93, 658).
Itraconazole
Intravenous itraconazole at 2.5 mg/kg produced reasonable blood levels in children from 7 months to 17 years of age (2), although trough blood levels were not consistently above the currently suggested 500 ng/ml target (260).
Voriconazole
Voriconazole dosages for children have been proposed as 6 mg/kg (load) q12h and then 3-4 mg/kg (maintenance) q12h (527, 837). Higher dosages may be needed in infants (527). Significant inter-subject variation in voriconazole systemic exposure has been reported and voriconazole plasma level monitoring is probably useful (99,537, 538).
Caspofungin
The limited data available suggest safety and utility (487, 511, 804). Caspofungin at 50 mg/m2 q24h gave exposures similar to those seen in adults treated with 50 mg/day (782), has been used successfully in a small number of cases (450), and is recommended by a pediatric expert (720). A dosage of 2 mg/kg/d has been suggested for neonates (836).
Anidulafungin
Pediatric patients treated with anidulafungin at 0.75 mg/kg/d and 1.5 mg/kg/d had drug exposures comparable to those achieved for adults treated with 50 and 100 mg/d, respectively (61).
Micafungin
Seibel et al. reported that micafungin was well tolerated at 0.5 and 4.0 mg/kg/day in pediatric patients and doses of 3 and 4.5 mg/kg would give exposures comparable to those seen in adults treated with 2 and 3 mg/kg/day, respectively (673). Population PK analyses by Hope et al. found that dosages of 5.1–6.7 mg/kg may be needed in pediatric subjects to achieve exposures seen in adults at 2–3 mg/kg/d (296). Micafungin at 2 mg/kg/d appeared as effective as liposomal amphotericin B in a comparative study of 106 pediatric subjects with candidemia (39). As for neonates, data on micafungin pharmacokinetics in premature infantsneonates > 1000g suggest that 5–7 mg/kg will approximate the AUC drug exposure of adults receiving daily doses of 100 mg and 150 mg (287).
Flucytosine
The half-life of flucytosine is variable, but tends to be prolonged in neonates. While doses of 50–200 mg/kg/d have been used, careful monitoring of serum levels (levels should remain < 100 μg/mL) and consideration of a reduced frequency of dosing are important. In particular, one report found such variation between patients (including patients with very slow elimination) that the authors recommended that flucytosine be started at q24h in newborns and adjusted after checking serum levels (49). A reference laboratory data on serum levels in children suggest that excessive concentrations are common with dosage regimens adapted from those used in adults (716), close monitoring and dosage adjustment are suggested when using this drug.
![]()
SPECIFIC SITUATIONS
Non-Genital Mucocutaneous Candidiasis
Oropharyngeal and Gastrointestinal Candidiasis
Candida are frequently found as asymptomatic commensals of the human gastrointestinal tract (131, 645). However, compromise of immune and mucosal defenses by HIV-1 infection, chemotherapy-induced neutropenia, or direct mucosal damage permits direct local invasion by Candida. Oropharyngeal candidiasis, with or without esophageal involvement, is the most readily appreciated form of disease. Mild infections limited to the oropharynx will often respond to topical agents used in a swish & swallow or oral troche format. Recognized topical therapies include nystatin (suspension of 100,000 U/ml, given as 4-6 ml qid; flavored pastilles containing 200,000 U, given as 1-2 pastilles 4-5 times daily) or clotrimazole (troches containing 10 mg, given as 1 troche 5 times daily) (136, 677, 834). The nystatin suspension has a bitter taste and most patients find the flavored nystatin pastilles or clotrimazole troches to be easier to tolerate. Work with a suspension of amphotericin B (163) has lead to commercial release of a 100 mg/mL suspension that appears effective when given as 1 mL swish and swallow qid.
If the oropharyngeal disease is extensive, if the patient has AIDS, or if signs and symptoms of esophageal involvement are present, then systemic therapy is indicated. Ketoconazole (PO, 200–400 mg/d, (384, 457, 692)), itraconazole (PO as capsules or solution, 100–200 mg/d, (254, 579, 692, 811)), fluconazole (PO, 100–400 mg/d, (12,254, 384, 385, 457, 579, 772, 811)), voriconazole (PO, 200 mg bid, (12)), posaconazole (PO, 200 mg load then 100 mg/day, (767)), caspofungin (IV, 70 mg load then 50 mg/d, (771, 772)), micafungin (IV, 150 mg/d, (155, 156)), anidulafungin (IV, 200 mg load then 100 mg/d, (365)), and amphotericin B (IV, 0.4–0.6 mg/kg/d, (385, 771, 778)) have all been used, with fluconazole generally being viewed as the initial therapy of choice because of its safety, its reliable pharmacology when administered by mouth, and the failure of any other therapy to be shown to be superior to fluconazole for infections due to azole-susceptible organisms.
Parenteral therapy with amphotericin B is effective but toxic and inconvenient, and should only be used in extreme circumstances. Likewise, the echinocandins are also effective and associated with little toxicity, but their lack of an oral form makes use inconvenient except in the situations discussed below. Ketoconazole and itraconazole can be efficacious, but their bioavailability is unpredictable and may be diminished by lack of gastric acid (especially ketoconazole) or lack of intake with food (itraconazole capsules) (275, 758, 761). Ingestion of ketoconazole with an acidic beverage helps its absorption (123). Ensuring adequate systemic exposure is important: therapy using itraconazole capsules was inferior to fluconazole in one study (522), and administering the solution of itraconazole in cyclodextrin improves the bioavailability and clinical efficacy of this drug (27, 254, 579, 810). Absorption of the cyclodextrin-based itraconazole solution is further enhanced if the solution is taken on an empty stomach.
Voriconazole is as effective as fluconazole, but associated with a greater rate of adverse events (12). Thus, it should be used only a second-line approach in selected patients with fluconazole-refractory disease.
On the other hand, fluconazole’s ready oral bioavailability makes it attractive under many circumstances and it has been shown to be more efficacious than the topical therapies for disease limited to the oropharynx (219, 360, 593) or ketoconazole for Candida esophagitis (384). Fluconazole at 100–200 mg/d is adequate for disease limited to the oropharynx, while 200–400 mg/d is suitable for patients with esophageal involvement.
The Problem of Resistance in Individuals with AIDS
While patients with cancer usually experience mucocutaneous candidiasis only while severely immunosuppressed, patients with advanced AIDS (CD4+ T-cell count < 100/mm3) have a permanent form of immunosuppression that leads to relapsing episodes of symptomatic oropharyngeal and esophageal disease. The agents discussed above are efficacious in these patients (256), although ketoconazole tends be poorly absorbed due to frequent gastric atrophy in this setting (96). Following successful initial therapy, individuals with AIDS frequently experience a relapse of the infection, re-treatment and/or chronic suppressive therapy are required in most patients who remain immunocompromised (167). Fluconazole is most often used in this setting at doses of 150 mg/week to 100–200 mg/day. However, use of such prolonged or repeated courses of therapy provides an opportunity for development of resistance. The prevalence of resistance has decreased dramatically since the introduction of effective antiretroviral therapy, emphasaising the importance of cell-mediated immunity in controlling oral candidal infections.
This problem has been reviewed and is most evident with fluconazole (623). The clinical situation is well understood, and this problem is seen after 1-2 years of either continuous or intermittent fluconazole therapy. Resistant infections are almost always due to C. albicans. Over time and under antifungal pressure, 8–10% of patients will develop a mutant strain of C. albicans that is no longer responsive to fluconazole, and the risk of development of resistance appears to be the same with continuous and intermittent therapy (246). This pattern has also been described with ketoconazole in patients with chronic mucocutaneous candidiasis and is both a function of the underlying disease and of the prolonged antifungal pressure in a host with a limited immune response. This pattern has also been described with topical therapy with clotrimazole (544).
This problem can develop with either intermittent or continuous antifungal therapy—one study found that chronic suppressive therapy produced a lower relapse rate than intermittent therapy but similar rates of microbiological resistance (610). Another large study examining the epidemiology of fluconazole resistance in AIDS patients linked continuous fluconazole use and trimethoprim-sulfamethoxazole prophylaxis with the onset of fluconazole-resistance mucosal disease (210). However, Goldman et al. subsequently showed in a randomized trial that continuous fluconazole therapy was more effective than episodic fluconazole therapy HIV-infected patients with access to active antiretroviral therapy and that episodic therapy was not associated with significant risk of fluconazole-refractory candida infection (245). That study also showed that the emergence of fluconazole resistance was associated with poor survival, reflecting (as does the use of trimethoprim-sulfamethoxazole prophylaxis) the advanced immunodeficiency in these patients. Once resistance develops, the mutation to resistance can be overcome for a time by increasing the dose of fluconazole stepwise to up to 800 mg/d (605). Unfortunately, once begun this process almost inexorably leads to a situation where fluconazole becomes completely ineffective (808). In addition, fluconazole resistance is often (but not always) associated with cross-resistance to the other azole antifungal agents (52, 418, 526, 762). One study found that about half of patients with fluconazole-unresponsive esophageal candidiasis did respond to itraconazole cyclodextrin solution at 100 mg bid (642). Similar concerns apply with voriconazole (526). Susceptibility testing and a review of the patient’s medication history are helpful at this point: non-compliance and/or concomitant use of a medication that lowers the effective level of fluconazole (e.g., rifampin) must be eliminated.
If antifungal resistance seems likely, a variety of alternative strategies can be employed. First, azole cross-resistance is not universal (418) and a trial of itraconazole at 200 mg bid is warranted. Use of the itraconazole solution is preferred: due perhaps both to its local effects and its better absorption, 64–80% of patients who failed to respond fluconazole have been reported to respond to itraconazole solution (187, 581). Second, data from individuals with refractory esophageal candidiasis have shown response rates of 61% (549) and > 50% (283) for voriconazole at its standard dosage of 200 mg twice daily. Third, posaconazole is also effective in this situation (687) with 75% response rates using either oral posaconazole (400 mg twice daily for 3 days followed by oral posaconazole 400 mg once daily for 25 days) or oral posaconazole (400 mg twice daily) for 28 days. Fourth, topical solutions of amphotericin B (163) or azoles (436, 437) produce relief in some patients. The topical nystatin preparations may also be tried but anecdotally appear less helpful than amphotericin B solution. Fifth, the echinocandins have been shown active. For example, caspofungin(70 mg loading dose followed by 50 mg daily, all given iv) has been shown to have response rates of 70-80% for esophageal candidiasis (771, 772), including that associated with fluconazole reistance (167). Consistent with the lack of cross-resistance with other mechanisms of action for this class of compounds (378), excellent results have been obtained in the setting of otherwise refractory disease (335, 694). Similarly, anidulafungin (100 mg load then 50 mg/day, (766)) has been shown active in azole-refractory oropharyngeal/esophageal candidiasis. Specific data are not available for micafungin in refractory disease, but its activity in azole-susceptible infections suggests it would work here as well. Finally, parenteral amphotericin B at 0.5–0.6 mg/kg/d is usually, but not always (386) effective. Flucytosine at 50–100 mg/kg/d is sometimes helpful in combination with amphotericin B. If the patient responds to amphotericin B, suppression may then be attempted with amphotericin B suspension. Other anecdotal remedies include (a) a maintenance regimen of amphotericin B at 0.5–1 mg/kg given 2–4 times weekly for suppression and (b) swish and swallow tid-qid with a 0.1–0.5% solution of gentian violet. All of these approaches require close clinical observation and dose titration in order to produce clinical relief without introducing additional side effects.
Improvement of immune status of patients with AIDS is critical, and the striking immune recovery that may be seen with initiation of effective antiretroviral therapy has been associated with marked clearance of the signs and symptoms of oropharyngeal candidiasis (115, 435, 841) and significantly reduces the risk of recurrence. Indeed, the resolution of thrush with protease inhibitors is so rapid as to lead to the suggestion that there may be a direct effect of these drugs on Candida spp. (363), as well as their known effect on improving the immune system. Effective antiretroviral therapy also obviates the need for suppressive or prophylactic antifungal treatment in patients with recurrent candidiasis (258).
In summary, oral or parenteral fluconazole remains the treatment of first choice for OPC or Candida esophagitis, with the newer agents offering no advantage. Moreover, one study found that anidulafungin use was associated with significantly higher relapse of esophatitis compared to fluconazole (365). In patients with fluconazole-refractory (resistant) disease caused by C. albicans or C. glabrata, a rapid therapeutic effect can be expected in 70-75% of patients with use of voriconazole, posaconazole, or parenteral echinocandins. Unless effective antiretroviral therapy follows, one can anticipate only a temporary reprieve. Relapse is inevitable and progression to complete azole and even echinocandin resistance may be seen. Finally, development of candidiasis should be taken as an indication to initiate or change antiretroviral therapy. The development of Candida infection in a patient already taking antiretroviral therapy suggests non-adherence to the antiretroviral therapy, the development of resistant HIV, or both.
Infection of Dentures and Dental Appliances
When oropharyngeal candidiasis occurs in the setting of denture use, aggressive disinfection of the prosthesis is usually required for definitive cure (168, 448, 799).
Candidal Diarrhea and Infection of the Gut Wall
Candida overgrowth in the lower gastrointestinal tract has been associated with a variety of ill-defined syndromes. Most prominently, persistent diarrhea has been described in the presence of heavy colonization of the fecal stream by Candida (267, 330, 399). A very careful epidemiological study found no convincing consistent linkage between carriage of Candida in the stool and the occurrence of antibiotic-associated diarrhea (366). That stated, there are reports that patients with (a) persistent diarrhea and (b) large numbers of yeast on stool gram stain do sometimes respond to therapy with nystatin at 250,000–1,000,000 U tid or qid (399). The pathophysiologic link here, if any, is unknown.
Candida can produce focal ulcerations in both the small and large bowel, and this can be associated with invasion of the submucosa (195). This is most common in immunocompromised patients, and therapy of this process follows the principles discussed in the section on Candidemia and Acute Disseminated Candidiasis.
Skin and Nail Candidiasis
While macronodular skin lesions due to disseminated candidiasis can be seen in neutropenic cancer patients (81), this is relatively uncommon and is treated in the context of treating the disseminated Candida infection. In otherwise healthy individuals, Candida can affect the glabrous skin, and this involvement is usually seen in areas that are compromised by moisture. Thus, intertriginous candidiasis, diaper-related candidiasis, paronychia, and toe or finger web space candidiasis (also known as erosio interdigitalis blastomycetica) are all well described (311). Candida can also cause folliculitis in regions compromised by moisture. Therapy should always begin by promoting local dryness, avoiding occlusion, and providing good local hygiene (26). In conjunction with these local measures, topical antifungal therapy is helpful and many active agents are available, including the azoles (clotrimazole, econazole, ketoconazole, miconazole, oxiconazole, and sulconazole), ciclopirox olamine, haloprogin, and the polyenes (nystatin, amphotericin B). Of note, tolnaftate-based preparations are active against the dermatophytes but not against Candida. Short courses of topical steroids are occasionally needed for severe cases. Systemic therapy with fluconazole, ketoconazole, or itraconazole will only rarely be appropriate, but could be considered in patients with very widespread disease or in other difficult situations (e.g., patients with poorly controlled diabetes).
Candida can also cause onychomycosis (199). While general therapy for onychomycosis has long depended on griseofulvin and ketoconazole, these drugs require prolonged therapy and have cure rates for toenail infections of < 50% (628). Use of these drugs for onychomycosis has largely been supplanted by terbinafine and the newer azole antifungal agents (31, 150, 362, 628). In the specific context of Candida onychomycosis, both terbinafine and griseofulvin have widely variable in vitro activity against isolates of Candida (63, 553, 641), and neither has been consistently efficacious Candida onychomycosis (628, 635).
Itraconazole’s excellent anti¬-Candida and anti-dermatophyte activity combined with its very long half-life in the skin and nails have made it very attractive for all forms of onychomycosis (290, 439, 711) Initial studies demonstrated that it had excellent activity against Candida when given at 100–200 mg/d for 3–6 months (287). Subsequent studies have taken advantage of the fact that substantial concentrations of itraconazole are present up to 6–9 months after cessation of therapy and have thus used pulse regimens of itraconazole in which the drug is given as 200 mg bid x 7 days and repeated monthly for a total of 3–4 months (151). It is important to realize when using these regimens that the nail may not appear completely normal at the end of the 3rd or 4th monthly cycle of therapy due to time required for new, healthy nail to grown and replace the diseased portions.
Fluconazole has likewise been shown to be active against Candida onychomycosis (as well as onychomycosis due to the more common dermatophyte agents) and is concentrated in the stratum corneum and nail matrix (711), but it is not retained as long in these tissues and it has been used as continuous therapy in studies to date (191, 628).
Chronic Mucocutaneous Candidiasis
Due to the associated underlying immune defect, the persistent and recurrent Candida infections seen in patients with chronic mucocutaneous candidiasis are difficult to treat and therapy with a systemic antifungal agent is required. This situation is analogous to the recurrent oropharyngeal candidiasis seen in patients with advanced AIDS, but differs in the universal need of chronic mucocutaneous candidiasis patients for continuous therapy. Therapeutic options are similar to those for patients with AIDS, and ketoconazole, itraconazole, and fluconazole have all been used successfully in these patients (104, 352). The required doses are similar and should be adjusted to find the minimal effective dose for each patient. Resistance to these azole antifungal agents can develop (301, 695) (see the section entitled “The problem of resistance in individuals with AIDS” for details). Use of immunomodulatory approaches have also proven successful in some patients (353).
![]()
Genital Candidiasis
Vulvovaginal candidiasis is affects up to 75% of women during their reproductive years (309, 349). In contrast to oropharyngeal candidiasis, vulvovaginal candidiasis is not an opportunistic infection and affects healthy women although the majority of attacks occur in the absence of recognizable precipitating factors (698). A small subpopulation of women suffer from recurrent, repeated bouts of vulvovaginal candidiasis, once more without known clearly proven causal factors. This latter group is thought to reflect an immunological breakdown in local protective mucosal defense mechanisms and frequent relapse is not due to resistant Candida or lack of protective lactobacilli (43,211, 212). Possible causal factors (e.g., reduced levels of mannose-binding lectin (42)) are under investigation.
The majority (80-95%) of infections are caused by Candida albicans isolates that are predictably susceptible to azole antifungal agents. Some evidence exists of an increased frequency of infections caused by non-albicans Candida species especially C. glabrata, C. parapsilosis and other species (300), but the true frequency and epidemiology of this phenomenon is uncertain at present. In HIV-infected women, use of fluconazole as chronic suppressive therapy has been associated with increased rates of vaginal carriage of C. glabrata (769).
An essential part of management of vulvovaginal candidiasis is accurate diagnosis. Millions of women each year receive antifungal agents unnecessarily due to incorrect self- and practitioner-made diagnosis (209). Topical and systemic therapy is not entirely benign and local application of azole antifungal agents may induce vulvar contact dermatitis. All treatment regimens should be preceded by microscopic (saline and 10% KOH) confirmation (70). Cultures should be obtained (a) in patients with compatible clinical syndromes and negative microscopy, (b) to document the rare instances of antifungal resistance in patients unresponsive to appropriate therapy, and (c) in women with recurrent vulvovaginal candidiasis in whom long-term suppressive prophylaxis is planned.
Treatment of vulvovaginal candidiasis in the 1990’s predominantly involves use of the imidazole and triazole agents available as topical or oral preparations (Table 6). Azoles achieve higher success rates even over shorter duration than nystatin vaginal suppositories or creams. Little evidence exists that the choice of formulation of the topical azoles influences cure rates. Topical agents previously prescribed for 7-14 days are now available as single dose or short (3-5 day) course regimens. Topical azoles when appropriately prescribed are remarkably free of systemic side effects and toxicity.
The oral azoles used for systemic therapy are ketoconazole, itraconazole, and fluconazole, but only fluconazole (150 mg given as a single dose) is approved by the FDA for this indication in the United States. Oral azoles have been shown to be at least as effective as topical agents while more convenient, popular and free of local side effects (153, 683, 701). Side effects of fluconazole are rare but include gastrointestinal upset, headache and rash. More serious hepatotoxicity precludes the widespread use of ketoconazole (400).
In selecting antifungal agent for therapy, it is useful to define vulvovaginal candidiasis as uncomplicated or complicated disease. By far the majority of episodes of vulvovaginal candidiasis are uncomplicated. These are sporadic, mild-to-moderate infections caused by Candida albicans that occur in normal hosts who lack predisposing factors. Uncomplicated infections can be successfully treated with any of the available topical or oral antifungal agents including short course and single dose regimens. Complicated infections are defined as those that (a) have a moderate to severe clinical presentation, (b) are recurrent in nature (> 4 episodes per year), (c) are caused by non-albicans Candida species, or (d) that occur in abnormal hosts (e.g., diabetic patients with poor glucose control).
Complicated infections are far less likely to respond to abbreviated courses of therapy (701) are should be treated more intensively for 7 to 14 days in order to achieve clinical and mycological response. In a study of almost 500 women with complicated vulvovaginal candidiasis, prolonging fluconazole therapy by adding a second dose of 150 mg fluconazole 72 hours after the initial dose resulted in significantly higher clinical and mycological cure rates in women with severe vulvovaginal candidiasis (705). Non-albicans Candida species are less sensitive in vitro to azoles and less likely to respond clinically to short course oral therapy (see Section entitled “Susceptibility in vitro and in vivo”). In particular C. glabrata is a vaginal pathogen that frequently fails to respond to azole agents regardless of route of therapy. Encouraging results have been obtained with boric acid 600 mg capsules given as one vaginally qd for 14 days (this must be prepared in gelatin capsules by a local pharmacy) (702, 703, 704) or topical flucytosine (299, 704). Similarly, infections due to C. krusei have been shown refractory to azole therapy and to benefit from boric acid therapy (686).
Vulvovaginal Candidiasis in Women with HIV Infection
Ulvovaginal candidiasis in HIV-infected women is incompletely understood. One large study found it to behave in a fashion similar to that in seronegative women (668). This study also found that vaginal carriage of Candida was slightly more common in seropositive women, but that symptomatic vulvovaginal candidiasis was not more frequent and did not increase with progressive immunosuppression. Other authors have, however, noted increased rates of vulvovaginal candidiasis with increasing immunosuppression (110, 176, 313, 625, 705, 718). The differences in results may be due to differences in study design and diagnostic criteria (668, 807). Longitudinal cohort studies of vaginal candidiasis in HIV-positive women show a progressive increase of colonization with C. glabrata and diminished fluconazole susceptibility (707). In a related analysis, vulvovaginal candidiasis was found to be more frequent with decreasing CD4 count and was associated with greater persistence but not greater severity than for seronegative women (175). Therapy of vulvovaginal candidiasis in HIV-infected women remains identical to that for seronegative women. Vulvovaginal candidiasis, even if recurrent, is not considered a sentinel of HIV infection and its presence does not justify HIV testing.
Recurrent Vulvovaginal Candidiasis
Recurrent vulvovaginal candidiasis is usually caused by susceptible strains of C. albicans. Although more intensive prolonged induction therapy lasting up to 14 days invariably induces remission, the fungistatic nature of the available agents combined with persistence of the underlying defect makes relapse almost inevitable without a maintenance antifungal regimen. Successful regimens include ketoconazole 100 mg daily (696) or fluconazole 150 mg weekly (697). In a prospective, multicenter, placebo-controlled study, Sobel el al. demonstrated a protective efficacy of 93% in women assigned to receive fluconazole 150 mg once weekly (710). Although relapse occurred in approximately 40% of women soon after stopping suppressive prophylactic therapy, cumulative cure rates at 1 year follow up were significantly higher than for the placebo group. Adverse reactions were rare and mild and no evidence of azole resistance emerged. No tendency was noted for selection of non-albicans species.
Male Genital Candidiasis
Male genital candidiasis presents in two forms. Most commonly a transient pruritic and erythematous penile cutaneous reaction may follow unprotected intercourse after exposure to Candida antigens present in the vagina and represents an hypersensitivity reaction. Successful treatment entails eradication of yeast in the vagina. True superficial penile invasive mycotic infection occurs infrequently and usually in diabetic and uncircumcised males who develop balanoposthitis which responds promptly to topical or systemic azole therapy.
Prevention of Vulvovaginal Candidiasis During Antibiotic Therapy
Lactobacillus-based probiotic preparations have long been used anecdotally to prevent vaginal candidiasis. They are taken both vaginally and orally, but data to support their use has always been limited. Pirotta et al. have provided data from a randomized and placebo-controlled study in which participants took a lactobacillus preparation either orally, vaginally, or both from the start of their course of antibiotics until four days after stopping antibiotics (584). 278 women were enrolled, 235 were evaluable, and compliance with therapy was high. However, the lactobacillus preparation had no measurable effect on the rate of post-antibiotic vulvovaginitis. These data make a strong case for lack of validity of this approach.
![]()
Candidemia and Acute Disseminated Candidiasis
As a marker of disseminated or invasive candidiasis, detection of candidemia is the single most specific tool currently available. Unfortunately, the term candidemia describes a very broad range of infections ranging from short-lived catheter-related fungemia in non-neutropenic ICU patients to persistent candidemia of uncertain (but probably gastrointestinal) origin in neutropenic cancer patients. While the overall mortality is strongly controlled by the patient’s underlying illness (298, 361), the presence of candidemia has been associated with a 38–49% attributable mortality over and beyond that of the underlying disease (262, 805). Further, an extensive analysis of the impact of microbiological factors on the outcome of nosocomial bloodstream infections found that infection due to Candida was the only specific infection that was independently associated with increased mortality in a multivariate analysis (586). Although the association of invasive candidiasis with mortality is thus strong, epidemiological data show a general trends towards a reduction in the absolute number of candidiasis-related deaths since the early 1990s (447, 562), an effect that is likely due to increasingly widespread use of effective antifungal therapy.
In the non-neutropenic patient, candidemia is related to the presence of an intravascular catheter in up to 80% of patients (614). In many of the remaining cases, an alternative source (urine, abscess) will be apparent. Removal of all intravascular catheters appears to help clear the bloodstream (361, 613) and has been associated with reduced mortality in both adults (413, 497, 629) and neonates (332). Some patients have even been cured with this simple approach (71, 356). However, even the most benign episodes of candidemia can be associated with subsequent hematogenous spread causing such disparate infections as endophthalmitis, osteomyelitis, and brain abscess (see the relevant sections on each of these forms of infection, below). Indeed, it was observed in a study of C. glabrata fungemia that the patients most likely to have a poor outcome were those who had persistent low grade fever (< 102.5 F) in association with a gradually declining clinical course (71).
Thus, it is currently believed that all episodes of candidemia merit some form of therapy (181,413). Minimizing the time elapsed from the first positive blood culture to initiation of effective therapy is also important: delays have been linked to increased mortality (229, 375, 473). Finally, a good dilated retinal examination is important in all candidemia patients. Candidal endophthalmitis can be subtle and delayed in its presentation, and such an examination should be performed at least once prior to discontinuation of therapy (98, 368, 630).
While amphotericin B was the standard approach for many years (456), the alternative options of fluconazole, an echinocandin, and voriconazole now offer therapy that is at least as effective and consistently better tolerated. While there may be a few remaining settings when amphotericin B will be preferred, most patients can now be treated with one of these agents.
Fluconazole
Fluconazole has a long history of successful use and is its multiple formulations permit oral follow-up therapy. Two prospective randomized trials (580, 614) and two uncontrolled retrospective/observational datasets (18, 497) have compared amphotericin B with fluconazole as therapy for candidemia. Taken together, these studies have shown that amphotericin B at 0.5–0.6 mg/kg/d and fluconazole at 400 mg/d, both given for approximately two weeks, are not significantly different as therapy of candidemia in non-neutropenic patients. It is important, however, to realize that this conclusion applies only to non-neutropenic patients and is also based largely on C. albicans fungemia.
The strength of the data with fluconazole is less robust for non-albicans species, but similar trends hold. However, as noted in the section entitled “Susceptibility in vitro and in vivo,” the non-albicans species have higher fluconazole MICs in particular and higher antifungal doses may be required for optimal outcome (525, 814). This point is especially pertinent with respect to C. glabrata and fluconazole. Although the available clinical data show similar outcomes with fluconazole and amphotericin B for C. glabrata (291, 614), the MICs for this species suggest that the standard 400 mg/d dosage would give blood levels barely adequate for therapy. Thus, there have been recommendations in the past to use of 800 mg/d (12 mg/kg) in adults with normal renal function. Therapy with 800 mg/day has, however, not been extensively studied. A collection of reports (73, 178, 251, 279, 617, 745) show the dose to generally be well tolerated and to appear more efficacious in some situations, but the availability of proven alternative therapies (especially the echinocandins) has reduced the need to maximize fluconazole’s range by pushing the dose in this fashion.
Caspofungin
This compound has been reviewed (109, 442). Mora-Duarte et al. have reported a study in adults that compared caspofungin (70 mg loading dose then 50 mg/d) with amphotericin B deoxycholate (0.6–1.0 mg/kg/d) for invasive candidiasis (469). The studied forms of candidiasis were a mixture of 83% candidemia, 10% peritonitis, and 7% miscellaneous forms. Overall, caspofungin was equivalent to but better tolerated than amphotericin B. Although supported to date by only this one trial, the demonstrations of the activity of this compound in esophageal candidiasis (including azole-resistant infections) (160), activity in a open-label series (336, 835), its clear activity in febrile neutropenia (795), and the compound’s excellent safety profile make caspofungin a suitable choice for initial therapy for invasive candidiasis.
The limitations of this compound are (a) the overall lesser experience with it to date, (b) the reduced in vitro activity of caspofungin against C. parapsilosis (564) and C. guilliermondii (557), and (c) the relative lack of excretion of caspofungin in to the urine (334). The clinical consequences of the latter two observations are as yet uncertain—successful therapy is seen in both settings. And, despite the handful of reports in the literature describing clinical resistance to echinocandins (and especially to C. parapsilosis), the number of reports is small and >99% of isolates in recent surveys apprear susceptible (562, 564).
Anidulafungin
This compound has been reviewed (109, 152, 768). Reboli et al. have reported a study in adults that compared anidulafungin (200 mg loading dose then 100 mg/d) with fluconazole (400 mg/d) for invasive candidiasis (604). Most (89%) of the enrolled subjects had candidemia alone. Response rates were similar for the two drugs, with anidulafungin showing statistical superiority at some early timepoints but not at the final 6-week followup observation point. The adverse event profiles were likewise similar for the two drugs. These strong data are supported by open-label data in candidemia (364), randomized data in esophageal candidiasis (365), and a demonstration of activity in fluconazole-refractory mucosal candidiasis (766).
Limitations of our understanding of this compound are similar to those for caspofungin: a relative paucity of data by comparison to fluconazole, concerns about the lesser in vitro activity towards some species (C. parapsilosis (564) and C. guilliermondii (557)), and the lack of excretion in to the urine (768). In addition, a notably high rate of relapse of esophageal candidiasis following anidulafungin therapy suggests that its penetration into oropharyngeal secretions or epithelial tissue is relatively limited (365).
Micafungin
This compound has been reviewed (109, 119). Kuse et al. have reported a study in adults that compared micafungin (100 mg/d) with liposomal amphotericin B (AmBisome, 3 mg/d) for invasive candidiasis (379). Most (ca. 90%) of the enrolled subjects had candidemia. Response rates were similar for the two drugs. Not surprisingly, micafungin had a lower rate of renal adverse events and a lower rate of infusion-related events. Pappas et al. have reported a three-arm randomized study in which micafungin 100 mg/d, micafungin 150 mg/d, and caspofungin 50 mg/d were compared (533). Approximately 85% of the patients had candidemia and response rates were similar across the three study arms. These strong data are supported by open-label data in invasive canddiasis (516) and randomized data in esophageal candidiasis (155, 156).
Limitations of our understanding of this compound are similar to those for caspofungin: a relative paucity of data by comparison to fluconazole, concerns about the lesser in vitro activity towards some species (C. parapsilosis (564) and C. guilliermondii (557)), and the lack of excretion in to the urine (119).
Voriconazole
Voriconazole is a reliable choice for therapy of invasive candidiasis. The principal proof of its activity comes from randomized study in which it was compared with amphotericin B followed by fluconazole as therapy for candidemia (372). In this large comparative study, efficacy and mortality rates for the two approaches were not statistically different across the full range of Candida species. In support of this study, a detailed review of the use of voriconazole as salvage therapy for invasive candidiasis provides data on treatment of 52 patients (517). The overall response rate was 56%. Consistent with this agent’s in vitro profile (see Table 4), a 70% response rate was reported for infections due to C. krusei. For C. glabrata, the potency of voriconazole is such that 98% of C. glabrata isolates that test as S-DD (susceptibility is dose-dependent) to fluconazole will be susceptible (S) to voriconazole (572). However, 40% of C. glabrata isolates that test resistant to fluconazole will also be resistant to voriconazole (572).
The limitations of this compound are (a) its many drug-drug interactions, (b) its relatively higher rate of treatment-related adverse events (although many of these are benign) (12, 372), (c) its less predictable serum concentration profile due to inter-subject variation in metabolism (693), and (d) the limitation on the administration of the intravenous formulation in individuals with a creatinine clearance < 30 ml/min or who are undergoing dialysis (the intravenous formulation uses a carrier that is not well cleared in these settings—see the section entitled “Antifungal Dosing in Renal Failure”). In general, voriconazole is simply not as easy to use as fluconazole and the latter is often preferred. If use of voriconazole seems appropriate, consideration of plama level monitoring may also be important in settings (e.g., treatment of children or in combination with agents known to induce the cytochrome systems responsible for voriconazole metabolism) where the systemic exposures are less reliably predicted (99, 537, 538). Target therapeutic concentrations in the range of 1–5.5 mg/L have been suggested (401, 537)
Itraconazole
Formulation of itraconazole in hydroxy-propyl-β-cyclodextrin permits reliable therapy via the intravenous route. The drug is given at 200 mg q12h for 4 doses (2 d) followed by 200 mg/d. Registration of this formulation was based entirely on demonstrations that intravenous therapy more rapidly achieves adequate blood levels with less patient-to-patient variability than itraconazole’s oral preparations (85, 763, 813, 840). In a a relevant study, intravenous then oral itraconazole (200 mg twice daily IV for two days as a loading regimen, then 200 mg IV daily, then 200 mg twice daily by mouth until completion of therapy) was equally efficacious with fluconazole (400 mg daily) as therapy of candidemia in non-neutropenic adults (749). As these data have thus far been presented only in abstract form, the possible use (parenteral) itraconazole for invasive candidiasis will not be further mentioned.
Posaconazole
Experience with posaconazole in candidiasis is relatively limited at present. Convincing activity in oropharyngeal candidiasis has been reported for a 200 mg loading dose followed by 100 mg/day (767) and also in fluconazole-resistant oropharyngeal and esophageal candidiasis (687). Response rates were similar to those for fluconazole with a trend towards a lower long-term relapse rate for posaconazole. Successful use in prophylaxis of invasive fungal infections (138) provides further support for the activity of this compound in candidiasis. However, and as for itraconazole, the greater data on other compounds and lack of an intravenous formulation makes use of posaconazole less necessary and its use for invasive candidiasis.
A Practical Approach to Therapy
On a practical basis, detection of fungemia in a non-neutropenic patient should prompt initiation of fluconazole (800 mg loading dose and then 400 mg/day) or an echinocandin (caspofungin: 70 mg load then 50 mg/day, anidulafungin 200 mg load then 100 mg daily, or micafungin 100 mg/day) (708). Of the three echinocandins, the greatest experience is available with caspofungin and the least with micafungin. Overall, the three echinocandins appear to have similar efficacy (109,708) and are particularly attractive empirical choices if infection due to a fluconazole-resistant isolate or species seems likely on epidemiological grounds. Voriconazole is also acceptable, but its limitations (see section entitled “Voriconazole”) generally make it less attractive. Amphotericin B at 0.6–0.7 mg/kg/d may be used if there is a strong concern regarding the possibility of resistance to fluconazole or the echinocandins, but this situation should be uncommon. The therapies of choice are summarized in Table 7. Useful further reviews of this area are also available (64, 717).
Predictions of the species of the infecting organism are difficult (682) and prompt evaluation of culture material in the laboratory is critical to choice of best continuation therapy (699). Once the isolate has been completely identified, it would be appropriate to complete therapy with fluconazole by mouth if the patient is doing well and the isolate is proven or likely to be susceptible to fluconazole. Otherwise, therapy may be completed intravenously with either an echinocandin or voriconazole. If voriconazole is deemed appropriate (as it will be most particularly for C. krusei infections), it is critical that the prescribing physician carefully review the potential for drug-drug interactions and the general pattern of adverse events associated with voriconazole. The situation in which a patient fails to respond to initial therapy is discussed below.
Within this strategic framework, therapy of C. glabrata infections is generally regarded as the most problematic situation. This organism consistently exhibits elevated MICs to all azoles (Table 4). Even when it is judged susceptible, these higher MICs suggest that maximal azole dosages would be required (46, 525, 814). In experience to date, therapy with amphotericin B and fluconazole has produced similar results (420, 614, 814). Based on current microbiological insight, the most reliable choice at present is an echinocandin. This limitation noted, many patients with C. glabrata infection have been treated successfully with fluconazole (614) and voriconazole (373). If the isolate is not resistant, follow-up use of one of these two agents is entirely acceptable. Both the US FDA and EU EMEA product labels support use of voriconazole for fluconazole-resistant isolates & species (especially C. krusei) that retain voriconazole susceptibility. Because of the lesser in vitro activity of the echinocandins vs. C. parapsilosis, therapy with fluconazole or an amphotericin is generally preferred.
Combinations of either fluconazole or amphotericin B with flucytosine at 100–150 mg/kg/d have been used anecdotally, but the utility of these combinations is not clear and they are not often employed (101). The combination of fluconazole with amphotericin B is intriguing, but long debated due to the theoretical potential for antagonism between these agents. See the section entitled “Combination Therapy” for further discussion of this area as well as the results of a study of combination fluconazole plus amphotericin B therapy for candidemia (617). The required duration of therapy is not certain, but this form of candidiasis has been successfully treated by giving the selected agent(s) for approximately two weeks after the last positive blood culture. With this approach, the rate of subsequent presentation with a recurrent infection at a hematogenously seeded site is about 1% (614).
The Neutropenic Patient
In the neutropenic patient, candidemia may take a more subacute, but nonetheless deadly course. Although the gut has on occasion been implicated as the source of fungemia in non-neutropenic patients (72), it appears likely that the gastrointestinal tract is the most common source of low-grade, persistent candidemia in neutropenic patients. Partial clearance of the blood by the liver and spleen explains the well-known syndrome of hepatosplenic, or chronic disseminated candidiasis (325). The organism can also spread to virtually every other organ of the body (307).
Therapy of candidemia in the neutropenic patient is less well understood. Removal of intravenous catheters may still be important (391), but the potential for a gastrointestinal source raises the possibility that the therapeutic effect of catheter exchange will not be as striking (502, 794). One notable exception to this rule is that C. parapsilosis fungemia is highly associated with intravascular catheters in cancer patients (238). Recovery of marrow function is critical, and no therapeutic approach is consistently successful in the face of persistent leukopenia. Reversal of neutropenia by removal of immunosuppression and use of colony stimulating factors is of course appropriate. Granulocyte transfusions would seem a rational stopgap maneuver in high-risk situations, but the data to date on this complex procedure are limited (165, 643).
Most therapeutic experience during neutropenia is with amphotericin B at 0.6–1.0 mg/kg/d until recovery of marrow function. The most appropriate dose of amphotericin B is not certain, but the non-albicans species do appear to require greater doses (0.8–1.0 mg/kg/d) of amphotericin B. This appears to be especially true of C. krusei (247) and C. glabrata, the two species that also are the least susceptible to fluconazole. However, and as with the more case of the non-neutropenic patient, data have been reported supporting the use during neutropenia of caspofungin (469), voriconazole (517), and fluconazole (19). Although none of these data are extensive, all suggest activity. A retrospective matched cohort study found that median daily doses of 400 mg for fluconazole and 0.6 mg/kg for amphotericin B were associated with similar outcomes in a mixed group of neutropenic and non-neutropenic cancer patients (19). Approximately 10% of the candidemia patients studied by Mora-Duarte et al. were neutropenic, and caspofungin performed as well as amphotericin B (469). Caspofungin performed as well as liposomal amphotericin B in those cases of febrile neutropenia wherein a baseline candidal infection was documented (795). Data on the use of the anidulafungin and micafungin in neutropenic patients are as yet quite limited. Finally, the salvage experience with voriconazole suggests similar activity in the small number of cases reported (517).
As always, flucytosine has been given to some patients, but its potential for marrow suppression and the lack of a readily available intravenous formulation lessen its attractiveness.
Taken together, these data would suggest at present that either amphotericin B or caspofungin would be appropriate as therapy the aggregate data suggest that therapy for invasive candidal infections in the neutropenic patient can be approached similarly to that for the non-neutropenic patient (Table 7). The major difference is that empiric use of an azole such as fluconazole is discouraged, especially given the fact that the majority of neutropenic patients routinely receive azole (fluconazole) prophylaxis. The only obstacle to declaring caspofungin the clear therapy of choice is the relatively lesser experience with it to date. Once the species of the infecting isolate is known and as the episode of neutropenia resolves, step-down therapy may proceed along the lines outlined above for the non-neutropenic patient.
Management of Catheters
As noted above, it is generally thought best to remove intravascular catheters where feasible in patients with candidemia (186, 207, 359, 502). However, this broad statement belies the complexity of this issue. To begin, it must be clearly understood that the gut is actually often the primary source of candidemia (501), with the catheter serving as a secondarily infected nidus. However, that infected nidus is often very important and worth treating. Three related questions then arise.
First, is there a strong method for determining if a given catheter is or is not the source of the problem? The answer here is a resounding “sometimes” and there a number of clues that may be considered. If the catheter’s insertion site appears inflamed, if the subcutaneous track appears abnormal, or if the catheter has malfunctioned, it should certainly be removed. Tunneled long-term catheters are somewhat less likely to be infected but use of any catheter for parenteral hyperalimentation seems to increase the likelihood of catheter infection. Bloodstream infections due to C. parapsilosis are almost always due to an infected catheter (18, 238). Differential quantitative venous and trans-catheter blood cultures have been proposed as a way to identify infected catheters (88, 740), as have differences in time to culture growth (88, 232). But, these approaches are not fully validated standardized, require special attention by the laboratory, and have not uniformly been effective (542). PET scanning (using 18F–fluorodeoxyglucose) has been suggested as a way to identify infected catheters (even in neutropenic patients) (459), but this obviously requires a significant technical expertise. Unfortunately, the physician is usually left with a need to make an arbitrary decision about a given catheter. Factors such as profound neutropenia and significant mucositis certainly increase the likelihood of a non-catheter source (502, 600), but the physician is unfortunately still left to make a very arbitrary choice.
Second, can the catheter be treated in place without removal? In our experience, the answer here is often no. However, the concept of therapy via “antibiotic lock” is sometimes suggested (451), and there are case reports in which installation of a solution of amphotericin B was used successfully to either treat or suppress the infection of a catheter (25, 37, 66, 319, 370, 770). Concentrations as high as 5 mg/ml have been used (25).
Third, how should one handle the report of a positive catheter tip culture for Candida spp. in the absence of positive blood culture? There are no firm guidelines on this point. It would seem rational, however, to approach this as one might approach the issue of colonization of any site. If the culture of catheter tip was obtained because the patient had a febrile syndrome, then the positive culture should probably be treated as being the equivalent of a positive blood culture. On the other hand, if the patient had no signs whatsoever of sepsis, then the catheter tip culture really should not have been obtained in the first place and can probably be ignored.
Presumptive Therapy of Disseminated Candidiasis
The Febrile Neutropenic Patient
In neutropenic patients with persistent fever despite several days of broad-spectrum antimicrobial agents, empiric initiation of amphotericin B as therapy for presumed fungal infections is well accepted (308, 588). The lack of adequate diagnostic tools (639) makes the situation challenging and pragmatic clinical thinking must be applied. Although Candida (and C. albicans) are the probably the most common fungi in this situation, concerns regarding azole-resistant isolates ofCandida and the possibility of aspergillosis drive the choice of therapy. Amphotericin B has long been the favored empirical agent due to its consistent activity against these two latter groups of organisms, but lipid-associated preparations of amphotericin B may be superior to standard amphotericin B in selected high-risk patients (784) and are preferred due to their superior safety. However, the recent demonstration of the similar efficacy but better tolerability of caspofungin relative to liposomal amphotericin B seem likely to turn this paradigm upside-down and caspofungin appears likely to emerge as the therapy of choice in this setting. At present, however, the use of either caspofungin or liposomal amphotericin B is well justified. As caspofungin has demonstrated similar efficacy but better tolerability relative to liposomal amphotericin B (795), it is also an appropriate choice. The other two echinocandins, anidulafungin and micafungin, would also likely be active but are less well studied at present in the neutropenic patient. Voriconazole is probably effective as well (793), but difficulties with interpretation of the primary trial data have limited its acceptance.
Fluconazole at 400 mg/day can be considered if the patient lacks signs, symptoms, or risk factors for aspergillosis; is at low risk for infection with azole-resistant isolates of Candida; and has not recently received azole prophylaxis (101, 423, 722, 773, 825). Itraconazole has activity against Aspergillus and has been shown to have similar efficacy to that of amphotericin B in this setting (84), and its good safety profile and activity against Aspergillus make it a valid choice in this setting—the only remaining concern would be azole-resistant Candida isolates. The intravenous and oral solution formulations of itraconazole can be used to lessen concerns about the poor bioavailability of the capsule formulation (239), and therapy should probably begin with the intravenous formulation. Blood itraconazole levels of 500 ng/ml (these levels are by HPLC and do not include itraconazole’s active metabolite) are correlated with efficacy (240). Ongoing work with diagnostic tools (e.g., galactomannan assays (415, 417)) may in the future help guide therapeutic choices.
The Non-Neutropenic Patient
While much less is well understood, disseminated candidiasis in non-neutropenic patients probably has a pre-candidemia phase in at least some patients. The typical setting will be that of a febrile ICU patient with an elevated APACHE II score (358), prolonged use of broad-spectrum antibiotics, parenteral hyperalimentation, central venous catheters, and recent surgery (especially surgery involving the gastrointestinal tract) (185, 361). Diabetes is also a strong risk factor (460). If alternative explanations for the persistent fever such as pulmonary emboli, cholecystitis, sinusitis, drug allergy, and wound infection are eliminated, the possibility of undetected disseminated candidiasis will arise. The most helpful clue in this regard is that colonization with Candida at any site will definitely increase the likelihood of disseminated candidiasis (185, 587). However, it is clear that merely being colonized is not the same as being infected (651) and no clear guidelines for initiating therapy in this setting are available (101) although some authors have suggested instructive decision algorithms (186).
A reasonable consensus approach at present is to consider use of empiric antifungal therapy in patients with (a) several days of fever that remains unexplained despite indicated investigations, (b) at least 4 days of ICU care, (c) use of broad-spectrum antibiotics for at least four days (d) presence of a non-tunneled central venous catheter, and (e) colonization with Candida of at least one site (519). Firm proof of the utility of this (or any) specific rule for initiation of antifungal therapy is lacking, with clinical studies often frustrated by low rates of candidiasis in the enrolled cohort. As a case in point, Schuster et al. found no aggregate value from initiation of empirical fluconazole therapy (800 mg/day) in a randomized placebo-controlled study (669). This study enrolled adults judged at high risk for candidiasis on the basis of persistent fever despite use of broad-spectrum antibiotics, an APACHE II score > 16, and use of a central venous catheter. The two groups had a similar overall outcome with about half of both groups failing to resolve their fever. Documented invasive fungal infections were seen in only 6 (5%) of the fluconazole group and 11 (9%) of the placebo group (RR 0.57, 95% CI 0.22-1.49). There were only two episodes of candidemia, both in the placebo-treated group. There was an intriguing trend favoring fluconazole in the subset colonized at baseline (invasive fungal infection was seen in 5 of 32 (15%) treated with fluconazole vs. developed invasive fungal infection compared to 9 of the 36 (25%) placebo-treated subjects, RR 0.63, 95% CI 0.23, 1.67), but this trend did not reach statistical significant due to small subject numbers.
If a decision is made to treat such a febrile non-neutropenic patient, a full therapeutic dose of an echinocandin, fluconazole, or amphotericin B should be employed. A prompt decision to institute such therapy may be life-saving: two studies now document a good connection between time to initiation of therapy and reduced mortality (229,473). As with all empirical therapies, continuous re-evaluation of the patient is required and therapy should be discontinued after 3–4 days if a response is not seen. As noted in the previous paragraph, it should be clearly understood that definite evidence supporting this strategy does not exist and that excessive use of this empirical approach should be avoided. The potential application and use of the beta-glucan serum test in this context is currently under investigation (515).
Chronic Disseminated Candidiasis
While therapy of chronic disseminated or hepatosplenic candidiasis has long depended on prolonged therapy with amphotericin B alone, this therapy has not been uniformly successful (277). Courses of 0.5–1.0 g of amphotericin B followed by a protracted course of fluconazole (200–400 mg/d for 2–14 months) are associated with cure rates of > 90% (16, 341). Indeed, use of fluconazole is sometimes successful for this disease when use of amphotericin B was not (16, 341). Lipid-associated amphotericin B has also been used successfully in small numbers of patients (796), as have caspofungin (336) and voriconazole (517). Provided that the lesions have stabilized, the patient is clinically improved, and antifungal therapy is continued, anti-neoplastic therapies (including those that will induce neutropenia) may be continued (781).
Neonatal Candidiasis
While critically-ill children can develop systemic candidiasis in a pattern just like that seen in adults, two distinct Candida syndromes can be defined in neonates, and especially in pre-term, low-birth-weight neonates. The most serious of these syndromes is neonatal systemic candidiasis, a syndrome that is usually due to C. albicans. Developing either via ascending infection of the uterine contents prior to birth or from colonization acquired during passage through the birth canal, hematogenous dissemination of Candida presents in the first days or weeks of life with symptoms identical to those of neonatal bacterial sepsis (201, 242, 318, 757). Involvement of the lung, skin, and particularly the CNS (36, 200, 479) are common, and involvement of almost all organs has been described (see (637), (203) and (120) for helpful reviews).
Amphotericin B at 0.5–1.0 mg/kg/d to a total of 10—25 mg/kg, with or without flucytosine, has long been the accepted therapy of choice for systemic neonatal candidiasis (see section entitled “Antifungal Dosing for Candida Infections in Pediatrics” for dosing considerations in the neonate). The excellent penetration of amphotericin B into the cerebrospinal fluid in infants (49) is presumably part of the reason that amphotericin B alone is often successful. The role of the lipid-formulations of amphotericin B is unknown in this setting, but data on therapy with liposomal amphotericin B (AmBisome, at doses from 2.5–7 mg/kg/day, but mostly at 5–7 mg/kg/day) suggests that it is safe and efficacious (327, 328, 404). A limited amount of data with amphotericin B lipid complex (ABLC) at 5 mg/kg/d likewise suggests safety and efficacy (404).
Fluconazole is also attractive in this setting, and has been used successfully at doses of 6–12 mg/kg day (172, 306, 779). Given the current data on optimal dosing in adults and the differences in kinetics between children and adults, doses of 12 mg/kg given every 24–72h (see above for a discussion of dosing frequency in pediatrics) appear suitable. Comparative data between amphotericin B and fluconazole in this setting are, however, lacking.
Data on use of the echinocandins in neonates are quite limited. See the section entitled Antifungal Dosing for Candida Infections in Pediatrics for a summary of available data.
Neonatal or congenital cutaneous candidiasis is distinct from the syndrome of neonatal systemic candidiasis. Neonates with congenital cutaneous candidiasis present within a few hours of birth with a diffuse maculopapular, erythematous rash involving almost any part of the skin (100, 242, 320, 329, 654). The rash can evolve to produce pustular or vesicular lesions with subsequent desquamation. Culture and microscopic examination of scrapings of the skin will reveal Candida species, usually C. albicans. If the affected infant is pre-term (< 1500g), systemic involvement is frequent and the infant should be evaluated repeatedly with blood, urine and CSF cultures in order to rule out neonatal systemic candidiasis (205, 320). On the other hand, this process in full-term infants is usually, but not always (54), limited to the skin and gastrointestinal tract. In this case, topical and oral therapy with agents such as nystatin or an azole antifungal often appears to be adequate therapy. Systemic therapy as described for neonatal systemic candidiasis would presumably also be efficacious, and should certainly be instituted promptly if there is any suspicion of systemic involvement.
![]()
Urinary Candidiasis
Urinary candidiasis is manifested by candiduria and involves infection at any of multiple anatomical levels in the urinary tract from kidney to urethra. Candida urinary tract infections account for 9% of nosocomial urinary tract infections and 90% Candida urinary tract infections are related to urinary catheters or instrumentation (719, 800, 828). While numerous host and treatment factors play a role in the pathogenesis of candiduria, a history of present or recent bladder catheterization, other indwelling devices and used broad spectrum antibiotics is found in 85-90% of candiduric patients (216, 274). Interpretation of candiduria is difficult (410), and outcome is probably driven largely by general host factors rather than directly by the candidal infection (541). Work from an in vivo model has shown that no specific number of CFU/ml can be used to identify true infection (492).
Candiduria in catheterized subjects usually represents catheter or superficial bladder colonization only, is extremely common, almost invariably asymptomatic, and of little clinical significance. Asymptomatic candiduria in this context should not be treated since ascending or invasive Candida infections are rare (24) and any effects of treatment are short-lived (706). Catheter removal alone eradicates candiduria in up to 40% of subjects (343, 706). Attempts to eliminate candiduria in chronically catheterized patients often fail.
Asymptomatic candiduria should be treated in neutropenic patients and those undergoing elective urinary instrumentation. In the past, investigators recommended treatment of asymptomatic candiduria following renal transplantation, however, a recent large retrospective study failed to show survival benefit by treating asymptomatic candiduria (644).
Symptomatic lower urinary tract infections due to Candida are rare and should be treated, especially in non-catheterized patients. Therapeutic options include oral fluconazole 200 mg/d for 7 days (777), IV amphotericin B as single dose of 0.3–1 mg/kg (215, 218), or conventional amphotericin B 0.3 mg/kg for 5-7 days (206). Single doses of amphotericin B are efficacious due to the slow terminal elimination of amphotericin B in the urine over at least 5–7 days following the dose (41, 218). Topical amphotericin B bladder irrigation with 1 L/d of a solution of 50 mg amphotericin B/L of sterile water or D5W through triple lumen catheter for 7-14 days is an effective but inconvenient option (653), although shorter courses may prove to be an alternative (396). Bladder irrigation is extremely labor intensive and less frequently used today.
Ketoconazole, itraconazole, voriconazole, and caspofungin the echinocandins achieve relatively lower urinary drug concentrations and as a consequence have the potential for reduced therapeutic efficacy (160, 830). Caspofungin has limited renal excretion (1-2% of active drug) and its role is likewise uncertain. However, the drug is of course present in the tissues of the urinary tract and a small number of well-studied treatment courses to date suggest potential efficacy when invasive Candida infections is involve the kidney or bladder (334, 700). Caspofungin local instillation has also been described (32).
Perhaps surprisingly, lipid-associated formulations of amphotericin B may also be less effective for urinary candidiasis. The lipid formulations produce reduced delivery of amphotericin B to the urine (59) and this has been linked to reports describing failure of lipid-associated amphotericin B formulations (7, 421).
In clinical practice, the difficulty inherent in evaluating the efficacy of any given therapy has effectively obscured any ability to estimate the clinical impact of these theoretical concerns. Oral flucytosine monotherapy is rarely indicated because of the high likelihood of emergence of resistance, but it is effective and anecdotally has appeared useful in eradicating non-albicans Candida infections. In contrast to Candida infections elsewhere, C. albicans is responsible for only 50-60% of candiduria episodes with C. glabrata causing 20-30%. Other species of non-albicans Candida urinary tract infection are also common and mixed infection with two or more Candida spp. are frequent in catheterized patients. Of these species, C. glabrata is the most frustrating to treat and can be quite refractory to therapy. No single best approach exists, but anecdotal experience suggests that fluconazole (higher doses are better and success is more likely if the isolate is not found resistant by in vitro susceptibility testing), flucytosine, and amphotercin B (either systemic or by bladder irrigation) be tried in sequence (421).
Ascending pyelonephritis, although uncommon, represents a serious infection that may be complicated by candidemia and disseminated infection (24). Therapy consists of relieving any urinary obstruction and use of fluconazole or systemic amphotericin B in doses used for disseminated candidiasis as described in the section entitled “Candidemia and Acute Disseminated Candidiasis.” Echinocandins have shown efficacy for Candida pyelonephritis and are especially useful for fluconazole-resistantCandida spp. or in the presence of renal failure procluding amphotericin B use (700). Finally candiduria may be the result of renal candidiasis secondary to previous or ongoing candidemia (hematogenous pyelonephritis). Therapy is again identical to that of disseminated candidiasis. With respect to caspofungin the echinoncandins, the concern about lack of urine level seems less relevant, and parenchymal renal disease has responded to this drug caspofungin (336).
Although available data are scant, candidal infections of the renal cysts of polycystic kidney disease would be expected to be difficult to treat. In the one available case report, C. krusei infection of such cysts proved refractory to therapy with AmBisome and nephrectomy was ultimately required (286). Amphotericin B levels in the cyst fluid were 0.1–0.2 mg/L and the MIC of the infecting organism was 0.5 mg/L.
Renal involvement is frequent in neonates with systemic candidiasis. Both parenchymal renal disease and collecting system ‘fungus balls’ may be seen. Prolonged medical therapy is usually required and most experience is with systemic amphotericin B therapy (331). Successful therapy has also been reported with fluconazole (747).
Candida Endophthalmitis
Lesions compatible with Candida endophthalmitis were seen in 15% of patients enrolled in a candidemia study (614), and other studies have a wide range of rates for such lesions with the strongest data suggesting a rate between 11 and 20% (169, 630). It is possible that the frequency of ocular involvement (and especially of more blatant lesions) is falling over time due to more consistent and earlier use of antifungal therapy (169, 630). While the classic lesion is a white, fluffy mass that extends from the retina into the vitreous, a variety of “non-classical” lesions (Roth spots, uveitis, hypopion, iritis, papillitis, retinal detachment, and ciliary body abscesses) have all been described with this infection (182) and the most common lesion is a small, white chorioretinal lesion without extension into the vitreous (169). As progressive endophthalmitis can lead to loss of vision, an examination after pupillary dilatation is a critical part of the evaluation of any patient with candidemia. Candida endophthalmitis can also present without a clinically evident episode of candidemia and should be considered in the differential diagnosis of suggestive retinal lesions in patients with recent risk factors for candidemia (528). However, the utility of retinal examinations as a diagnostic tool for otherwise cryptic invasive candidiasis is limited by the frequency with which other systemic illnesses causes the more common non-specific lesions (630).
Once lesions compatible with Candida endophthalmitis are identified, therapy is not standardized (350) although treatment guidelines have been suggested (486). The common small white chorioretinal lesions seen in patients with candidemia appear to respond readily to most available agents (169), while larger lesions or infections that develop following trauma or surgery may require more aggressive and targeted therapy. The penetration of amphotericin B into the eye is variable but generally poor (217, 507). Despite this, courses of at least one gram of amphotericin B have been curative in > 90% of infected eyes (182). However, intravenous therapy is not uniformly successful and intravitreal amphotericin B following vitrectromy has been helpful either as monotherapy or in conjunction with systemic therapy. Vitrectomy may be especially valuable in endophthalmitis due to intravenous drug abuse (433). This role for vitrectomy in therapy of Candida endophthalmitis is consistent with a parallel result reported for bacterial endophthalmitis (193) and with results from case series (196). Intravitreal doses of amphotericin B of 5-10 μg have been used (97, 108, 293, 486, 551, 724).
Fluconazole diffuses well into all parts of the eye (506, 656, 753), and the experience with this agent as therapy for Candidaendophthalmitis has been reviewed (9). Fluconazole was given as sole therapy at ~200 mg/d for approximately two months and cured 15 of 16 infected eyes. Fluconazole was also used effectively following short (~200 mg total dose) courses of amphotericin B. Patients requiring vitrectomy generally have more severe disease, and fluconazole monotherapy was curative in five eyes after vitrectomy when given at ~200 mg/d for ~ 3 months. If an implant is present in the infected eye, implant removal appears critical to resolution of the infection (342). Narendran et al. have reported a good experience with a combination of fluconazole (200–400 mg/day) and flucytosine (a somewhat unusually high dose of 200 mg/kg/d in four divided doses) in a case series (486). Ketoconazole and itraconazole penetrate the eye less readily than fluconazole in animal models (656).
Ketoconazole has been used successfully in a small number of patients (97, 249), but no meaningful clinical experience with itraconazole has been reported. ABLC combined with vitrectomy was successful in a case of endophthalmitis due to C. glabrata (147).
Based on recent case series, voriconazole at standard dosages appears to be a suitable alternative (95, 276). Breit et al. reported voriconazole concentrations in the aqueous and vitreous of 1.52 mg/L and 1.12 mg/L after 7 days of voriconazole therapy (95). Although simultaneous serum levels were not provided, these levels compare well with the typical levels of 1–5 mg/L seen in other clinical studies. This same report also mentions use of caspofungin in several patients, but the usage consistently overlapped with that of voriconazole and was of shorter duration. Hariprasad et al. summarize over 40 case reports and likewise conclude that voriconazole achieves effective intraocular concentrations and is associated with frequent clinical response (276). A 28-day course of caspofungin was curative in a patient with C. glabrata endophthalmitis (655).
Candida Endocarditis, Pericarditis, and Suppurative Phlebitis
Candidal Endocarditis
Candida can cause both native and prosthetic valve endocarditis (788) and is associated with approximately twice the mortality of non-fungal causes of endocarditis (45). The distribution of causative species generally parallels that for candidemia, with C. albicans as the most common single species (62, 192). C. parapsilosis is particularly associated with prosthetic valve endocarditis (230) Although medical therapy alone has occasionally been curative (202, 272, 839), the general recommendation is that most patients be treated with a combination of valve replacement and prolonged (often lifelong) antifungal therapy (192, 322,359, 481). Recent approaches to care may be changing — in 2 prospective cohorts (495, 45), the mortality rate was similar for patients receiving combined medical/surgical therapy and those receiving medical therapy alone. However, the non-randomized nature of such data limit the strength of the conclusions that can be drawn and surgery is often required for management of complications.
The reported literature on this approach has mostly employed amphotericin B followed by one of the azoles (583, 721). While both ketoconazole and itraconazole have been used, fluconazole has been the most frequently employed oral agent. Optimal doses of the drugs in combination with surgery are unknown: typical courses of amphotericin B are ~ 2 grams (237), and the azoles (most often fluconazole) are then used at 200–400 mg/d (106, 481, 495) for periods of as little as 6 months in two reported patients (326, 495) but more often for very prolonged periods or indefinitely. On a practical basis, it is really not known if lifelong therapy is required and we would suggest at least 6 months of therapy. If therapy is to be discontinued, very close observation is warranted. Caution may dictate continued suppression, and we would be more inclined towards lifelong therapy if the patient were at unusually high risk of adverse outcome should a recurrence led to the need for repeat valve replacement.
Fluconazole (614), amphotericin B deoxycholate (440), and liposomal amphotericin B (449) have been used successfully as the sole antifungal therapy in selected patients with native valve endocarditis. Such medical monotherapy has been described in adults (614), children (449), and neonates (202, 204, 440, 647, 839). As with other forms of candidiasis, flucytosine is also occasionally added to the base regimen (440), but its overall utility is uncertain. Late recurrence has been described even several years after the initial episode (322), emphasizing the need for prolonged follow-up.
Although the volume of available data is limited and often involve use of caspofungin as part of a sequential regimen (44, 414), caspofungin appears active as therapy of candidal endocarditis. Six weeks of caspofungin appeared curative in an elderly woman with a dual (C. glabrata and C. krusei) infection of a prosthetic mitral valve (602). Endocarditis due to C. glabrata in a neonate with multiple cardiac malformations and prior repair of a ventricular septal defect was successfully treated with patch removal and caspofungin at 3 mg/kg/d x 6 weeks (480). Native mitral valve endocarditis due to C. glabrata in an adult was successfully treated with medical monotherapy in a regimen that began with a combination of liposomal amphotericin B (3 mg/kg/d) plus caspofungin (50 mg/d) for 3 weeks followed by 8 weeks of caspofungin monotherapy at 50 mg/d, then four weeks of voriconazole, and then finally an additional 12 weeks of caspofungin at 100 mg three times per week (317). On the other hand, prosthetic aortic valve endocarditis due to C. albicansultimately responded to valve replacement and prolonged caspofungin therapy, but (and consistent with the relatively poor penetration of caspofungin into the CNS (160, 270, 303)) candidal brain abscesses appeared to progress during therapy and ultimately required liposomal amphotericin B followed by fluconazole for cure (597).
The ready oral availability of fluconazole has made it especially attractive in efforts to employ medical therapy alone. Most cases of Candida endocarditis are caused by C. albicans or C. parapsilosis (230), two species that are generally susceptible to fluconazole. On the basis in vitro data and some animal models (829), a number of investigators have now successfully employed chronic suppressive therapy with fluconazole as part of a medical strategy in selected patients with both native (114, 288, 636) and prosthetic valve endocarditis (1, 114, 780). This long-term suppressive approach has typically been taken following a course of amphotericin B in patients for whom cardiac surgery is judged unusually risky. The optimal dose and duration of therapy is uncertain: typical courses of amphotericin B have been ~2 grams, and fluconazole has then been used indefinitely at 200–400 mg/d. Data on the use of other azoles (e.g., posaconazole (28)) have begun to appear but are very limited. The lipid amphotericin B preparations would also be expected to be effective in this setting and Aaron et al. used liposomal amphotericin B (AmBisome) for 47 days (the dose used was not reported) prior to placing a patient with candidal prosthetic valve endocarditis on chronic suppressive therapy with fluconazole at 200 mg/day (1).
Candida infections of the transvenous portions of cardiac pacemakers have been described and appear to require both surgical removal of the infected device followed by moderately prolonged systemic antifungal therapy (324, 359). Case reports describe both successful and unsuccessful therapy of candidal infections of ventricular assist devices (680).
Candidal Pericarditis
Purulent Candida pericarditis has been reviewed (601, 667), and a combination of surgical drainage (pericardiocentesis or pericardiectomy) with prolonged antifungal therapy is required. Most experience is with amphotericin B (194,261, 667), and the utility of other antifungal agents is unknown.
Candidal Suppurative Phlebitis
Persistent candidemia is sometimes due to Candida suppurative phlebitis of either central or peripheral veins. In the case of peripheral phlebitis, the involved vein may merely appear thrombosed and is not always tender. Treatment by removal of the catheter; aspiration, resection, or incision & drainage of the vein; and a short course of amphotericin B (total dose of 200–500 mg) is generally effective (71, 746, 783). Surgical resection, aspiration, or drainage often appear to be critical to successful therapy. Fluconazole has been employed successfully in a small number of reported cases (224). When a central vein is involved, surgery is not an option and several authors have reported successful outcomes following amphotericin B given for a total of ~30 mg/kg (i.e., about 2 grams in a typical adult) (69, 316, 729). Systemic anticoagulation was used in some, but not all of the described patients.
Infection of Dialysis Fistulas and Other Intravascular Devices
Candida infections of arteriovenous dialysis fistulas have been reviewed (499). These infections are very rare and effective therapy appears to require both antifungal therapy and removal of the fistula. Likewise, infections of vascular bypass grafts can be difficult to clear, relapse after apparently successful therapy, and require removal for successful therapy (394). Management of other types of infected vascular devices would be presumed to follow similar problems (47, 48, 359).
![]()
Candida Infections of the Peritoneum, Gallbladder, Pancreas
Candida can cause peritonitis in two settings. First, patients undergoing peritoneal dialysis may develop catheter-related peritonitis. Removal of the dialysis catheter is usually required for successful therapy (188, 244, 461, 466), and some patients have been cured via this maneuver alone (57, 189, 730). Short courses of amphotericin B have been used by both the intravenous and intraperitoneal routes as antifungal therapy. Intraperitoneal therapy with infusate containing 0.5–5 μg/mL amphotericin B has been recommended, but is often associated with significant abdominal pain and development of adhesions (33, 189). Numerous reports have documented the utility of fluconazole, sometimes in combination with flucytosine, as therapy for dialysis catheter-related peritonitis (137, 398, 461, 741). These reports have generally used 100–200 mg/d fluconazole and the authors emphasizing the use of flucytosine used 15 mg/kg after hemodialysis or 50-100 mg/L in the peritoneal dialysate (188, 461). Successful therapy with voriconazole has also been described (357).
Candida-related peritonitis is also seen following intra-abdominal events such as surgical opening or spontaneous perforation of the bowel. Injury or surgery above the level of the transverse mesocolon appears to be more strongly associated with finding Candidain the peritoneal fluid (468). Patients with refractory gastrointestinal perforation may have an especially high risk of developing this problem (184). Peritoneal cultures in this setting are often polymicrobial. Although experimental studies suggest that Candida and bacteria may both contribute to abscess-related mortality (657), the significance of Candida in the culture is not always obvious clinically. As previously described for involvement of the biliary tree or pancreas, however, the potential for untreated Candida both to be associated with worse outcomes (652) and to cause objective disease (10, 105, 714) has now been clearly demonstrated.
While no single set of criteria identify the patients in whom Candida is significant (652), factors such as presence of fungemia, increased severity of illness, multiple operations, pancreatic involvement, isolation in the absence of a peritoneal catheter, and heavy or pure growth of Candida from peritoneal cultures strongly suggest that antifungal therapy will be critical to the patient’s outcome (10,105, 603). Examination of biopsy specimens for evidence of tissue invasion has also be used to be diagnose and monitor the course of therapy (371). As a rule, isolation of Candida from patients with non-catheter-related intra-abdominal infections should not be ignored. Amphotericin B at widely varying doses (but averaging 0.5–1 g total) has been used to treat this condition (10, 105, 714), as has fluconazole at 200–400 mg/day (6, 371, 741). Flucytosine has also been used, but as in other forms of candidiasis its actual utility is unclear.
Candida may infect the gallbladder, biliary tree, or pancreas (307). While it is isolated from the bile in up to 2% of cholecystectomies (266), mere isolation of the organism does not provide convincing evidence that it is pathogenic. However, if the patient has biliary obstruction or gangrenous cholecystitis, then isolation of Candida should not be ignored and systemic therapy with amphotericin B or fluconazole should be given. Amphotericin B achieves bile concentrations that are 2- to 7-fold higher than serum concentrations (5). Caspofungin biliary levels were reported at 30% of simultaneous serum levels in one patient (243). There are no meaningful data comparing these agents in this setting. Candida fungus balls can cause obstruction biliary of the collecting system and may require surgical removal (266, 419).
Involvement of both the pancreatic parenchyma and pancreatic pseudocysts has been reviewed (14, 348). Candida is often present in combination with enteric bacteria in these processes, although Candida is at times the sole agent isolated (626). In this setting, the pathogenic role of the isolated Candida relative to that of concomitantly isolated bacteria is not certain, but the association between increased mortality and Candida superinfections in patients with acute necrotizing pancreatitis (257, 292, 315) provides strong support for use an antifungal agent if Candida is isolated. After suitable debridement and/or drainage, amphotericin B at standard systemic doses (0.5–1.0 mg/kg/d to a total of 1–2 grams) has been the most commonly used reported therapy. The utility and comparative value of the other agents in this setting is unknown.
Candida Osteomyelitis, Arthritis, and Mediastinitis
Candidal Osteomyelitis
Candida seems to have special predilection for causing osteomyelitis. The infection is usually hematogeneous (although contiguous infection related to surgical procedures such as median sternotomies is well described), usually involves the vertebral column, and can even occur following reasonable courses of antifungal therapy for presumed or proven candidemia (208, 231, 733). Osteomyelitis is also quite common as part of the widely disseminated disease seen in neonatal systemic candidiasis (see section entitled “Neonatal Candidiasis”, above), and therapy for the systemic disease should be adequate for the bony component. In general, a variety of therapeutic strategies have been successful in adults and children. Surgical debridement can be helpful, but is not required (231).
Vertebral osteomyelitis may be an exception to this rule—published data suggest that medical therapy alone may have a high failure rate (284, 675). While flucytosine monotherapy (181, 226) has been occasionally successful, most authors have used amphotericin B as the primary agent. Courses of 1–1.5 g have usually (13, 183, 208, 220, 231), but not always (208), been successful. One report suggested that amphotericin B might safely be added to bone cement in complicated cases (430). A number of authors have followed a course of amphotericin B with 6–12 months of ketoconazole (200–600 mg/d) (13, 231) or fluconazole (150 mg/d) (462,733). Although no follow-up data are given, liposomal amphotericin B at 5 mg/kg given 42 days without surgical debridement was apparently successful as therapy of culture-proven C. tropicalis vertebral osteomyelitis (135).
There is also some experience with azoles as sole therapy. Ketoconazole was been used successfully at 50 mg/d for three months in a three-year-old boy with phalangeal osteomyelitis (51) and at 400–1600 mg/d for 3–7 months in adults (166). Fluconazole has been successful at 200–400 mg/d for 6–12 months in three brief reports (285, 733, 738) and at 400 mg/d for one month (381). In a fourth report, an infected prosthetic knee was cured by fluconazole at 800 mg/day plus prosthesis removal and repeated debridement (395). However, fluconazole at 400 mg/d failed as therapy for zygomatic osteomyelitis (38) and as therapy for sternal osteomyelitis in a second patient (146). However, fluconazole (generally at 400 mg/d for six months and following surgical debridement) produced durable cures in 7 of 10 patients with sternal osteomyelitis due to C. albicans (422). The remaining three patients responded but later relapsed—of these, two responded to an additional 9–12 months of fluconazole whereas the third was placed on lifelong suppressive therapy. A report from Petrikkos et al. described a patient in whom initial therapy with fluconazole at 400 mg/day failed but subsequent therapy at 800 mg/day (total duration of 6 months) was successful (554).
There is limited experience with itraconazole for Candida osteomyelitis. Consistent with a report of successful itraconazole therapy of Aspergillus osteomyelitis (764), six months of itraconazole (600 mg/d) was reported to cure a probably sternal osteomyelitis caused by C. krusei (554). There is a report of successful use of caspofungin for osteomyelitis due to C. parapsilosis (685).
Candidal Arthritis
Like osteomyelitis, Candida arthritis can develop in adults, children, and neonates (58, 585, 684), and has been noted to present as much as one year after an episode of fungemia (736). This topic has been reviewed (684). Combined medical-surgical therapy will often cure native joint infections, but relapse after seemingly successful therapy is always a risk (389). If the infection involves a prosthetic joint, resection arthroplasty is virtually always required (359, 750). Merrer et al. described successful medical treatment (fluconazole for 17 months) of a hip prosthesis that was infected with Candida albicans (452), but post-therapy followup was only 11 months and this type of response appears to be the exception rather than the rule. Amphotericin B has been used intravenously at quite variable doses: as little as 200 mg and as much as 2 g has sometimes been needed (58). Intraarticular amphotericin B has also been used at variable doses: typically 5–10 mg is injected at intervals in association with joint aspiration (58). Flucytosine at standard doses has been used with amphotericin B (684).
Experience with the azole antifungal agents is limited. Ketoconazole has been used successfully at 200–800 mg/d (177), but was ineffective at 800 mg/d in another report (340). Fluconazole at 200 mg/d was effective in a case of prosthetic joint arthritis that had failed to respond to ketoconazole at 400 mg/d (750). Fluconazole at 400 mg/d for 12 weeks was curative in a case of native joint arthritis (514). A seven-month course of therapy at 400 mg/day was effective in a second case of native joint arthritis (802). In this case, simultaneous synovial fluid and blood drug concentrations of 20 μg/mL were reported, thus documenting good drug penetration. Another report describes the cure of an infected knee in a neonate with fluconazole alone given for 6 months (803). Finally, fluconazole was effective at 5 mg/kg/d with 150 mg/kg/d flucytosine in an infant (512) with native joint arthritis.
Candidal Mediastinitis
Mediastinitis due to Candida is rare, usually due to C. albicans, and has been reviewed (125). Based on a small number of cases, surgical debridement followed by either amphotericin B or fluconazole appears suitable.
![]()
Candidal Meningitis
Three forms of Candida meningitis can be identified. First, patients with acute hematogenously disseminated candidiasis may develop involvement of the brain and meninges (162, 406, 536). This occurs most often in neonatal systemic candidiasis (see that section as well as (203) and (479) for reviews), but can also occur in older children (443) and adults. The species distribution follows that for systemic candidal infections in general—C. albicans is consistently the most common specific species.
The available literature on this condition focuses almost entirely on therapy with amphotericin B, often in combination with flucytosine because of the later agents ability to penetrate the blood-brain barrier (102, 122, 450, 689). Amphotericin B is usually given intravenously, although occasional patients have required intrathecal therapy, presumably in order to overcome the poor penetration of amphotericin B into the cerebrospinal fluid. Liposomal amphotericin B is attractive as a substitute for amphotericin B deoxcyolate due to the demonstration in rabbit models of greater brain concentrations with it than with either amphotericin B lipid complex or the deoxycholate form (259). Clinical data supporting the relevance of this observation are few, but response trends from a series of cases of invasive rhinocerebral zygomycosis suggest greater efficacy for liposomal amphotericin B (606).
Fluconazole with flucytosine was successful in one case (427), and fluconazole monotherapy was used in another report (268). Voriconazole achieves CSF levels that are 22–100% of those in plasma (412). Posaconzole, however, produces low CSF levels (744). The utility of the echinocandins is as yet uncertain due to very limited data on tissue penetration and clinical efficacy (76). Caspofungin has been used successfully in neonates (487, 511) and an adult (407), although only limited brain tissue levels were reported in murine studies (270), drug was not detected in the CSF of a patient with coccidioidomycosis (303), and progression of brain abscess due to C. albicans occurred in another patient (597). In the case of micafungin, work in a rabbit model suggests that adequate tissue penetration might occur in neonates given substantial doses of micafungin (295). No data are available on anidulafungin.
Much less commonly, patients with one more risk factors for hematogenous candidiasis present with the clinical picture of a chronic meningitis that otherwise would suggest tuberculosis or one of the endemic mycoses (112, 121, 775). The small number of patients with this form of infection have been reviewed, and amphotericin B, sometimes with flucytosine, and sometimes followed by a course of fluconazole were variously used (112, 121, 775).
Finally, Candida can produce meningitis following neurosurgical procedures, especially in association with cerebrospinal fluid devices such as shunts or drains (121, 124, 233, 498, 649). The findings are quite similar to those of bacterial meningitis, and device removal plus antifungal therapy is required. Distinguishing between specimen contamination and true infection can be difficult, as neither increased CSF cellularity nor hypoglycorrhachia are consistently present (233). Patients with true infections do, however, more often have repeatedly positive cultures (233). Intravenous amphotericin B is usually effective, but some patients require addition of flucytosine or intrathecal amphotericin B to their regimen. Regimens of 0.5 mg/kg/d amphotericin B and > 75 mg/kg/d flucytosine for three or more weeks have been recommended (498). Both failures and successes have been reported with fluconazole (121, 142, 498), thus precluding any judgment on its utility in this setting. However, the excellent penetration of fluconazole into the cerebrospinal fluid suggests that might be a useful agent in this setting.
As noted above, caspofungin has relatively limited brain penetration and its utility in this setting is unknown (160).
In an anecdotal report, therapy with liposomal amphotericin B at 3 mg/kg/d produced CSF sterilization in a patient whose external ventricular shunt had become infected with C. albicans, but the cerebrospinal fluid levels were only 0.09–0.24 micrograms/ml and the patient ultimately died (154).
In addition to these forms of Candida meningitis, Candida brain abscess (75, 103), epidural abscess (83), and intramedullary abscess (405) have been described. Treatment of these rare conditions has been with amphotericin B and flucytosine, sometimes followed by oral azole therapy.
Candida Pneumonia
The most common form of respiratory candidiasis is colonization of the upper airways, especially in intubated patients. Finding Candida in cultures of respiratory secretions does, not, however, usually mean that the patient has Candida pneumonia (190,608). Rather, such cultures usually represent colonization alone and should be interpreted in the context of the patient’s overall status—in afebrile patients they may be ignored, while they increase the likelihood of disseminated candidiasis in patients with unexplained fever (see section on Empirical Therapy of Disseminated Candidiasis, above). Indeed, it has been suggested that a policy of reporting such results as “yeasts, not Cryptococcus” and thus discouraging active therapy may be appropriate (53).
Primary (or bronchogenic) Candida pneumonia appears to be quite uncommon and was documented in only 0.2–0.4% of patients in two large autopsy series (278, 438). The syndrome of primary Candida pneumonia is principally defined based on autopsy results and little certain knowledge about suitable therapy is available. As these patients tend to be quite ill, treatment that follows the guidelines for acute disseminated candidiasis given above would appear suitable.
Candida may also seed the lung during hematogenous dissemination and thus produce pneumonia. This appears to occur most often in neutropenic patients and therapy follows the general guidelines for treatment of disseminated candidiasis given in the section entitled “Candidemia and Acute Disseminated Candidiasis.”
Finally, laryngeal candidiasis associated with respiratory stridor has been described. Therapy with Amphotericin B (214, 786) and fluconazole (797) has been successful.
![]()
Alternative Therapies
Augmentation of host defenses is an intriguing approach to the problem of refractory Candida infections, but the work in this area is still preliminary at best. Combining such cytokines as inteferon-γ (374), G-CSF (273, 776), and GM-CSF (441) with an antifungal agent has been shown to lessen the course of the infection in animal models of disseminated candidiasis. The experience in animals with M-CSF has been mixed (116). The published experience in man is extremely limited and focuses on use of inteferon-γ in patients with chronic granulomatous disease (269).
Use of white blood cell transfusions in persistently neutropenic patients has long been of interest for refractory infections of all types. However, problems with obtaining sufficient numbers of cells for transfusion and with transfusion-related side-effects lead to loss of interest in this technique (728). Studies in which white cell donors are treated with G-CSF in order to augment the number and function of the collected cells are intriguing (165), as are studies in which ex vivo manipulation of neutrophils with cytokines has been shown to extend their functional lifetime (355, 615). The broad application of these tools awaits, however, much additional work (666).
Transfer of Candida-specific immunity to patients with chronic mucocutaneous candidiasis by administration of Candida-specific transfer factor has been associated with long-lasting remissions of that disease and suggests that highly focused manipulations of the immune system may be helpful in specific situations (353).
Finally, experimental therapy with an anti-Candida antibody has produced interesting early results (523), but our understanding of the potential role of this novel therapy is currently limited (111).
![]()
ENDPOINTS FOR MONITORING THERAPY
Candida is not a fastidious organism, and is readily grown from most sites of local infection with any standard culture technique. The notable exception to this rule is the blood, and it is now clear that blood culture technologies differ in their ability to detect candidemia. Estimates of the sensitivity of blood culture systems have been derived from retrospective analyses of the frequency of fungemia in patients (usually with cancer) that are proven by other means (often autopsy) to have disseminated candidiasis. These estimates range from 4–35% (307). The lysis-centrifugation system (also known as the “Isolator” system) is clearly superior to older systems and is probably the most sensitive of the currently available techniques (74). This system is, however, expensive and the automated BACTEC high-blood-volume fungal media (HBV-FM) has been shown to be equivalent to lysis-centrifugation for recovery of Candida spp (816). Finally, the automated BacT/Alert system also appears to have good sensitivity for candidemia (634).
Unfortunately, even these newer blood culture systems do not detect all patients with disseminated infection. For example, Berenguer et al. demonstrated that while the sensitivity of the lysis-centrifugation on invasive candidiasis rose with the number of organs found to be involved at autopsy, positive cultures were obtained from only 58% percent of 19 patients with disseminated candidiasis (68). To augment culture-based approaches, a great deal of effort has been directed towards development of non-culture based tools for diagnosis and monitoring. Unfortunately, no simple solution to this problem has emerged. Antibody detection systems have low sensitivity and specificity. While a series of older techniques have failed to achieve widespread acceptance (87, 234, 255), approaches based on new antigens are intriguing (491, 759, 760). Detection of antigens released by the organism works well for other fungi, but while some of the systems developed to date have good specificity, none of them have had the excellent sensitivity seen for other fungal antigen detection systems (235). Detection of the Candida metabolite D-arabinitol is a promising approach, but further work is needed before the method is widely used (792). Finally, PCR for Candida DNA has been extensively studied (785), but its place in diagnosis still remains uncertain. A system based on detection of fungal glucan may also prove useful (503, 505, 515). At present, however, use of any of these methods must be regarded as experimental. None of these tools have yet become a part of routine clinical practice — clinical judgment remains the critical factor in determining the intensity and duration of anti-Candida therapy.
![]()
PROPHYLAXIS
General Principles
Prophylaxis may refer both to prevention of colonization/asymptomatic infection or to prevention of symptomatic disease. Since Candida spp. are such ubiquitous organisms and are often part of the human microbial flora, prevention of colonization is difficult, impractical, and rarely considered. However, there are specific circumstances where prevention of acquisition of Candida may be important, most notably in nosocomial settings. Aggressive infection control measures (especially hand-washing) and, on occasion, selective decontamination of colonized individuals using oral nystatin, has been shown to control outbreaks (145). However, in most circumstances, prophylaxis for candidiasis refers to the use of antifungal agents to protect individual patients from disease and the remainder of this section will focus on such uses.
Specific Situations
HIV-Infected Patients
Although Candida infections are the most common opportunistic infection in AIDS, the associated costs, possibility of inducing resistance, and the relatively low morbidity associated with the initial episodes of oropharyngeal candidiasis seen in these patients makes primary prevention unnecessary. Rather, work has focused on secondary prevention of recurrences in patients who have had several prior episodes of oropharyngeal candidiasis. Most studies have used fluconazole in varying dosages for this purpose and several have clearly shown that doses ranging from 150 mg once weekly to 100 mg daily are associated with success rates of 60-100% in preventing relapses of oropharyngeal candidiasis over a short period of time (393, 431, 726). Itraconazole at 200 mg daily is also effective (691). Breakthrough infections do, however, appear likely to occur during prolonged suppressive therapy and one study found breakthrough disease more likely at 400 mg fluconazole/week than 200 mg/day (280). In a study of fluconazole (200 mg/d) as prophylaxis for cryptococcal meningitis, symptomatic oropharyngeal candidiasis occurred during the three-year study in 15% of patients in the fluconazole group and in almost 50% of patients who took clotrimazole troches regularly (595). A placebo-controlled trial found that the rate of breakthrough disease was no different for patients treated with itraconazole 200 mg daily than for those patients given placebo (445). An increased rate of vaginal carriage of non-albicans species was seen in HIV-infected women who used fluconazole over extended periods, but the clinical relevance of this observation is not clear (769). This is in part because of the reduced clinical attack rate of vaginitis due to non-albicans species.
The optimum drug, drug dose, and dosing frequency for long-term suppression have not been established, nor have clear indications for selecting patients for suppressive therapy. In advanced AIDS, the consequences of recurrent oropharyngeal disease (symptoms may interfere with eating and compound an already poor nutritional state) must be weighed against the risk (usually low) of toxicity or drug interaction, the cost of chronic suppressive therapy, and the ~5-10% risk of developing azole-resistant disease. The risk of developing azole-resistant disease appears to be the same with continuous and intermittent therapy (92, 245). Patients with esophageal candidiasis clearly merit long-term suppressive therapy due to the almost 100% risk of recurrence (383). Prophylactic therapy for patients with symptomatic recurrences limited to the oral mucosa should be tailored to suit the clinical situation and either intermittent or continuous therapy can be considered. Fluconazole will usually be the agent of choice due to its lack of interactions with the other medications that are commonly used as therapy for advanced AIDS, and doses of 100–400 mg/day can be used. As has already been stated however, both primary and secondary prevention of HIV-associated candidiasis is best accomplished by providing effective antiretroviral therapy with the consequent recovery of immune function (594).
Neutropenic Patients
Measures to decrease the frequency of Candida infections in patients with neutropenia have included local therapy designed to decrease colonization and systemic chemoprophylaxis (138, 179, 390). In general, oral regimens that are designed to reduce the amount of Candida in the gastrointestinal system by using polyenes (nystatin or amphotericin B) or non-absorbed azoles such as clotrimazole have had moderate activity in the prevention of oropharyngeal infection but little or no effect on rates of systemic candidiasis (144, 158). Compliance is also a major problem with these regimens. As the risk of symptomatic infections associated with the mild neutropenia seen in AIDS patients is considerably lower than the risk for leukopenic and transplant patients, antifungal prophylaxis is not warranted in leukopenic AIDS patients who lack these additional risk factors.
Fluconazole at dosages of 50-400 mg/daily has been very effective in preventing oropharyngeal candidiasis and decreasing colonization with Candida. At the higher doses, fluconazole has been shown to decrease systemic candidiasis in adult patients undergoing bone-marrow transplantation as well as to reduce the need for systemic amphotericin B (250, 688). The utility of fluconazole is less clear in other neutropenic patients (662, 824), but adults undergoing therapy for acute myelogenous leukemia also would appear to benefit (612). Because fluconazole is less active against C. glabrata and inactive against C. krusei, increased colonization, and at some centers, increased infection with these species has been reported as a consequence of prophylactic use of fluconazole (118, 821, 822). In addition, fluconazole lacks activity against Aspergillus species, and this may further limit its usefulness in certain high-risk patient groups.
Data on the utility of itraconazole in this setting suggests that it might be able to prevent both Candida and Aspergillusinfections in high-risk patients (241, 471). The availability of newer formulations that more reliably produce adequate blood levels appears to be the key to using this compound effectively. Glasmacher et al. reviewed data on 3,597 patients from 13 trials of itraconazole prophylaxis and found a consistent and statistically supported protective effect only in those trials that used the cyclodextrin solution during periods of oral therapy. For example, in a randomized open-label comparisons of fluconazole (400 mg/day intravenously or by mouth) with itraconazole (200 mg intravenously every 12 hours for two days follow by 200 mg intravenously daily or 200 mg oral solution twice daily), the rate of proven fungal infections during the first 180 days following bone marrow transplantation was reduced from 25% to 9% (826). Although not statistically significant for any one fungal species and limited by the trial’s open-label nature, by a higher rate of unmatched donors and graft-versus-host disease in the patients randomized to fluconazole, and by the counting as successes those patients who required empirical amphotericin B or who died (333, 475, 596), the data from this trial showed a trend towards reduced rates of candidiasis and aspergillosis in the group randomized to receive itraconazole. Taken with similar data from six other trials using cyclodextrin (241), itraconazole cyclodextrin oral solution at 400 mg/d or the IV formulation at 200 mg/d do appear to reduce effectively rates of invasive fungal infections, however patient tolerance of itraconazole solution is a frequent limiting factor.
Similarly, data on posaconazole suggest a role in prophylaxis of invasive fungal infections. In a convincing randomized comparison with standard azole prophylaxis (fluconazole or itraconazole), posaconazole at 200 mg three times daily reduced the rate of proven & probably fungal infections from 8% to 2% in patients with prolonged neutropenia (139). Survival was also increased in the subjects randomized to posaconazole. In a randomized trial conducted among patients with severe graft-versus-host disease, posaconazole was similar to fluconazole for prophylaxis against fungal infections and reduced overall mortality from invasive fungal infections (751). Survival was also increased in the subjects randomized to posaconazole.
Data comparing voriconazole (200 mg BID) with fluconazole (400 mg QD) as prophylaxis during allogeneic bone marrow transplantation have been reported (818). Microbiologically document invasive fungal infections were somewhat less common in the voriconazole arm but event-free and overall survival rates were similar at 6 and 12 months.
Amphotericin B given systemically has also been evaluated as prophylaxis in bone-marrow transplant recipients. Low doses of amphotericin B deoxycholate (0.1 mg/kg/day) have been reported to reduce the incidence of serious fungal infections (548), but a study that used a lipid-associated amphotericin B preparation at 1 mg/kg/day demonstrated decreased rates of fungal colonization but not of fungal infections (743). By far the greatest experience with amphotericin B in this setting is not as true prophylaxis but rather as early empiric treatment of febrile neutropenic episodes in which the fever persists despite antibacterial agents. When used in this fashion, amphotericin B has been shown in prospective trials to reduce the incidence and morbidity of fungal, and especially candidal, infections. Such therapy is very commonly used in managing patients with prolonged neutropenia and new or persistent fever (308,789).
Prophylaxis with echinocandins is also logical due to their spectrum of activity. However, this has not been explored systematically except in one study of micafungin (756).
Despite these data, selection of patients who should receive antifungal prophylaxis remains somewhat controversial. As a general rule, patients who are likely to be severely neutropenic for 14 or more days would appear to receive the most benefit from prophylaxis. While this would include many bone marrow transplant recipients, it is important to understand that not all antineoplastic regimens are associated with equal levels of risk (787, 812). Available data suggest that the type of chemotherapy is important in predicting relative risk of invasive candidiasis and thus likely benefit from prophylaxis, with regimens that produce large amounts of damage to the gastrointestinal mucosa being associated with the highest rates of invasive candidiasis (90, 91). In addition, heavy oral and fecal colonization with Candida also predicts an increased likelihood of invasive candidiasis, and such patients have benefited from prophylaxis (264).
Solid Organ Transplantation
Certain patients undergoing liver transplantation have been identified as being of high risk forCandida infections, especially candidemia (132, 310, 500, 539, 589). The consistently observed relevant risk factors in these studies appear similar to those for candidemia in general and have included increased creatinine (or dialysis), need for retransplantation, and use of antibacterial antibiotics. Low doses (10–20 mg/d) of amphotericin B deoxycholate, lipid-associated amphotericin B, and fluconazole have been evaluated as prophylaxis in this setting and have been shown to reduce fungal colonization and the risk of serious Candida infections (376, 403, 742, 827). A meta-analysis by Playford et al. concluded that fluconazole prophylaxis reduced invasive fungal infections by about 75% and was appropriate for patients at increased risk of infection (589). Itraconazole has been shown to reduce rates of superficial fungal infections and the rate of suspected systemic infections (676). It must be kept in mind, however, that low dose amphotericin B therapy may be inadequate to prevent other fungal infections such as aspergillosis. Pancreatic transplant recipients may also be at increased risk for invasive candidiasis and one study has demonstrated a reduced frequency of intraabdominal candidiasis in patients treated post-transplant with fluconazole 400 mg/d (60). There are no conclusive data on the value of routine antifungal prophylaxis in other groups of solid organ transplant recipients.
Other Settings
Because of the high attributable mortality associated with invasive candidiasis, there has been considerable interest in prevention of infection in other high-risk settings such as adults in intensive care units or after abdominal surgery (624, 709) or in neonates (344, 424, 426). The potential utility of this concept in adults was demonstrated by a trial in which the rate of peritonitis due toCandida in patients with refractory gastrointestinal perforation was decreased from 35% to 4% (P < 0.02) by use of fluconazole at 400 mg/day (184). This study is particularly of interest as the rule for study entry was based on clinical data (refractory perforation) rather than microbiological data. Although small and applicable only to a small subset of patients, this study does show that suitably targeted prophylaxis can be of value. Antifungal prophylaxis with oral polyenes has been reported to be of benefit in patients after severe burns and also in patients undergoing continuous ambulatory peritoneal dialysis (161, 838).
Randomized trial data to support these ideas have begun to emerge for two care areas. First, Pelz et al. reported results from a single center randomized study in which fluconazole at 400 mg/day by mouth trended strongly towards reduction in the rate of invasive candidiasis in a series of 260 adults admitted to a surgical intensive care unit for at least 3 days (545). Similar data were reported in a single-center study reported by Garbino et al. in which adults expected to remain on mechanical ventilation for at least 72h were all given a regimen for selective bowel decontamination along with being randomized to receive fluconazole (400 mg/day) or placebo (227). In further support of these data, a prospective open-label single-center study that targeted SICU patients with elevated candidal colonization indices showed a reduction in proven candidal infections relative to an historical comparison cohort from 7% to 3.8% (582).
In a parallel demonstration in neonates, Kaufman et al. reported that fluconazole therapy reduced the rate of invasive candidiasis from 20% to 0% (P = 0.008) in a series of 100 preterm infants with birth weights of less than 1000 g (345). In this study, fluconazole was given for six weeks at 3 mg/kg iv every 3rd day x 2 weeks, every other day x 2 weeks, and then every day. A 6-year observational dataset from a single center suggested a similar result and concluded that all very low birth weight infants may benefit from prophylaxis (424, 425). These results have also been supported by a multicenter study comparing 6 or 3 mg/kg fluconazole q3d x 2 weeks then q.o.d. with placebo for neonates weighing less than 1500 g at birth (426). The incidence of invasive fungal infection was reduced by fluconazole from 13% to < 4% in the two treatment arms.
Although these demonstrations are intriguing, the special features of the patients in the adult ICU studies (including significant rates of liver transplantation in the study from Pelz et al. (545)) and the single center nature of some of the studies (344, 424, 582) or their lack of concurrent control group (582) suggest that further validation would be relevant (143, 519, 529, 611). Unfortunately, validation of highly sensitive and specific rules for the adult ICU has proven difficult (521) and the decision to use prophylaxis should be guided by local epidemiology and rates of invasive candidiasis. However, and supported by several meta-analyses (681, 765) as well as the more recent large multicenter study (426), fluconazole prophylaxis of all infants weighing less than 1000g or aged < 27 weeks has been recommended, as has targeted prophylaxis for infants weight 1000-1500g are high risk due to use of a central venous catheter or antibiotics for more than 3 days (346). In addition, centers that already experience high rates of invasive candidiasis might consider these approaches in addition to standard infection control measures.
![]()
REFERENCES
1. Aaron L, Therby A, Viard JP, Lahoulou R, Dupont B. Successful medical treatment of Candida albicans in mechanical prosthetic valve endocarditis. Scand J Infec Dis 2003;35:351-352. [PubMed]
2. Abdel-Rahman SM, Jacobs RF, Massarella J, Kauffman RE, Bradley JS, Kimko HC, Kearns GL, Shalayda K, Curtin C, Maldonado SD, Blumer JL. Single-dose pharmacokinetics of intravenous itraconazole and hydroxypropyl-beta-cyclodextrin in infants, children, and adolescents. Antimicrob Agents Chemother 2007;51:2668-2673. [PubMed]
3. Abel S, Allan R, Gandelman K, Tomaszewskil K, Webb DJ, Wood ND. Pharmacokinetics, safety and tolerance of voriconazole in renally impaired subjects - Two prospective, multicentre, open- label, parallel-group volunteer studies. Clin Drug Invest 2008;28:409-420. [PubMed]
4. Abi-Said D, Anaissie E, Uzun O, Raad I, Pinzcowski H, Vartivarian S. The epidemiology of hematogenous candidiasis caused by different Candida species. Clin Infect Dis 1997;24:1122-1128. [PubMed]
5. Adamson PC, Rinaldi MG, Pizzo PA, Walsh TJ. Amphotericin B in treatment of Candida cholecystitis. Pediatr Infect Dis J 1989;8:408-411. [PubMed]
6. Aguado JM, Hidalgo M, Ridriguez-Tudela JL. Successful treatment of Candida peritonitis with fluconazole. J Antimicrob Chemother 1994;34:847. [PubMed]
7. Agustin J, Lacson S, Raffalli J, Aguero-Rosenfeld ME, Wormser GP. Failure of a lipid amphotericin B preparation to eradicate candiduria: preliminary findings based on three cases. Clin Infect Dis 1999;29:686-7. [PubMed]
8. Aisner J, Schimpff SC, Sutherland JC, Young VM, Wiernik PH. Torulopsis glabrata infections in patients with cancer: Increasing incidence and relationship to colonization. Am J Med 1976;61:23-28. [PubMed]
9. Akler ME, Vellend H, McNeely DM, Walmsley SL, Gold WL. Use of fluconazole in the treatment of candidal endophthalmits. Clin Infect Dis 1995;20:657-664. [PubMed]
10. Alden SM, Frank E, Flancbaum L. Abdominal candidiasis in surgical patients. Amer Surg 1989;55:45-9. [PubMed]
11. Alexander BD, Ashley ED, Reller LB, Reed SD. Cost savings with implementation of PNA FISH testing for identification of Candida albicans in blood cultures. Diagn Microbiol Infect Dis 2006;54:277-82. [PubMed]
12. Ally R, Schurmann D, Kreisel W, Carosi G, Aguirrebengoa K, Dupont B, Hodges M, Troke P, Romero AJ. A randomized, double-blind, double-dummy, multicenter trial of voriconazole and fluconazole in the treatment of esophageal candidiasis in immunocompromised patients. Clin Infect Dis 2001;33:1447-1454. [PubMed]
13. Almekinders LC, Greene WB. Vertebral Candida infections. A case report and review of the literature. Clin Orthop Related Res 1991;267:174-178.[PubMed]
14. Aloia T, Solomkin J, Fink AS, Nussbaum MS, Bjornson S, Bell RH, Sewak L, McFadden DW. Candida in pancreatic infection: a clinical experience. Amer Surg 1994;60:793-6. [PubMed]
15. Alonso-Valle H, Acha O, Garcia-Palomo JD, Farinas-Alvarez C, Fernanez-Mazarrasa C, Farinas MC. Candidemia in a tertiary care hospital: Epidemiology and factors influencing mortality. Eur J Clin Microbiol Infect Dis 2003;22:254-257. [PubMed]
16. Anaissie E, Bodey GP, Kantarjian H, David C, Barnett K, Bow E, Defelice R, Downs N, File T, Karam G, Potts D, Shelton M, Sugar A. Fluconazole therapy for chronic disseminated candidiasis in patients with leukemia and prior amphotericin B therapy. Am J Med 1991a;91:142-150. [PubMed]
17. Anaissie E, Paetznick V, Proffitt R, Adler MJ, Bodey GP. Comparison of the in vitro antifungal activity of free and liposome-encapsulated amphotericin B. Eur J Clin Microbiol Infect Dis 1991b;10:665-668. [PubMed]
18. Anaissie EJ, Rex JH, Uzun Ö, Vartivarian S. Predictors of adverse outcome in cancer patients with candidemia. Am J Med 1998;104:238-245. [PubMed]
19. Anaissie EJ, Vartivarian SE, Abi-Said D, Uzun O, Pinczowski H, Kontoyiannis D, Khoury P, Pappadakis C, Gardner A, Raad I, Gilbreath J, Bodey GP. Fluconazole versus amphotericin B in the treatment of hematogenous candidiasis: a matched cohort study. Am J Med 1996;101:170-176. [PubMed]
20. Andes D. Antifungal pharmacokinetics and pharmacodynamics: understanding the implications for antifungal drug resistance. Drug Resist Updat 2004;7:185-94. [PubMed]
21. Andes D, Marchillo K, Stamstad T, Conklin R. In vivo pharmacodynamics of a new triazole, ravuconazole, in a murine candidiasis model. Antimicrob Agents Chemother 2003a;47:1193-1199.[PubMed]
22. Andes D, Marchillo K, Stamstad T, Conklin R. In vivo pharmacokinetics and pharmacodynamics of a new triazole, voriconazole, in a murine candidiasis model. Antimicrob Agents Chemother 2003b;47:3165-3169. [PubMed]
23. Andes D, van Ogtrop H. Characterization and quantitation of the pharmacodynamics of fluconazole in a neutropenic murine disseminated candidiasis infection model. Antimicrob Agents Chemother 1999;43:2116-2120. [PubMed]
24. Ang BSP, Telenti A, King B, Steckelberg JM, Wilson WR. Candidemia from a urinary tract source: Microbiological aspects and clinical significance. Clin Infect Dis 1993;17:662-666. [PubMed]
25. Angel-Moreno A, Boronat M, Bolanos M, Carrillo A, Gonzalez S, Perez Arellano JL. Candida glabrata fungemia cured by antibiotic-lock therapy: case report and short review. J Infect 2005;51:e85-7. [PubMed]
26. Anonymous. Guidelines of care for superficial mycotic infections of the skin: Mucocutaneous candidiasis. J Amer Acad Dermatol 1996;34:110-5.[PubMed]
27. Anonymous. Sporanox (itraconazole oral solution) Product Information. Titusville, NJ: Janssen Pharmaceutica, 1997. [PubMed]
28. Anstead GM, Martinez M, Graybill JR. Control of a Candida glabrata prosthetic endovascular infection with posaconazole. Med Mycol 2006;44:273-277. [PubMed]
29. Antoniadou A, Torres HA, Lewis RE, Thornby J, Bodey GP, Tarrand JJ, Han XY, Rolston KVI, Safdar A, Raad, II, Kontoyiannis DP. Candidemia in a tertiary care cancer center - In vitro susceptibility and its association with outcome of initial antifungal therapy. Medicine 2003;82:309-321. [PubMed]
30. Arathoon EG, Gotuzzo E, Noriega LM, Berman RS, DiNubile MJ, Sable CA. Randomized, double-blind, multicenter study of caspofungin versus amphotericin B for treatment of oropharyngeal and esophageal candidiasis. Antimicrob Agents Chemother 2002;46:451-457. [PubMed]
31. Arenas R, Dominguez-Cherit J, Fernandez LM. Open randomized comparison of itraconazole versus terbinafine in onychomycosis. Int J Dermatol 1995;34:138-43. [PubMed]
32. Arend SM, Kuijper EJ, de Vaal BJ, de Fijter JW, van't Wout JW. Successful treatment of fungus balls due to fluconazole-resistant Candida sake obstructing ureter stents in a renal transplant patient. Eur J Clin Microbiol Infect Dis 2006;25:43-45. [PubMed]
33. Arfania D, Everett ED, Nolph KD, Rubin J. Uncommon causes of peritonitis in patients undergoing peritoneal dialysis. Arch Intern Med 1981;141:61-64. [PubMed]
34. Arikan S, Lozano-Chiu M, Paetznick V, Rex JH. In vitro synergy of caspofungin and amphotericin B against Aspergillus and Fusarium spp. Antimicrob Agents Chemother 2002;46:245-247. [PubMed]
35. Arikan S, Rex JH. Resistance to antifungal agents. In: Collier L, Balows A, Sussman M, Ajello L, Hay RJ, eds. Topley & Wilson's Microbiology and Microbial Infections. 10th ed. London: Arnold Publishing, 2005:168-181. [PubMed]
36. Arisoy ES, Arisoy AE, Dunne WM, Jr. Clinical significance of fungi isolated from cerebrospinal fluid in children. Pediatr Infect Dis J 1994;13:128-33. [PubMed]
37. Arnow PM, Kushner R. Malassezia furfur catheter infection cured with antibiotic lock therapy. Am J Med 1991;90:128-30.[PubMed]
38. Arranz-Caso JA, Lopez-Pizarro VM, Gomez-Herruz P, Garcia-Altozano J, Martinez-Martinez J. Candida albicans osteomyelitis of the zygomatic bone. A distinctive case with a possible peculiar mechanism of infection and therapeutic failure with fluconazole. Diagn Microbiol Infect Dis 1996;24:161-164.[PubMed]
39. Arrieta A, Queiroz-Telles F, Berezin E, Freire A, Diekmann S, Koblinger S. Micafungin versus liposomal amphotericin B (AmBisome®) in paediatric patients with invasive candidiasis or candidaemia. 17th European Congress of Clinical Microbiology and Infectious Diseases. Munich, Germany, 2007, Abstract No. 1732_85. [PubMed]
40. Ashley ESD, Lewis R, Lewis JS, Martin C, Andes D. Pharmacology of systemic antifungal agents. Clin Infect Dis 2006;43 (Suppl. 1):S28-S39. PubMed]
41. Atkinson AJ, Bennett JE. Amphotericin B pharmacokinetics in humans. Antimicrob Agents Chemother 1978;13:271-6. [PubMed]
42. Babula O, Lazdane G, Kroica J, Ledger WJ, Witkin SS. Relation between recurrent vulvovaginal candidiasis, vaginal concentrations of mannose-binding lectin, and a mannose-binding lectin gene polymorphism in latvian women. Clin Infect Dis 2003;37:733-737.[PubMed]
43. Babula O, Lazdane G, Kroica J, Linhares IM, Ledger WJ, Witkin SS. Frequency of interleukin-4 (IL-4)-589 gene polymorphism and vaginal concentrations of IL-4, nitric oxide, and mannose- binding lectin in women with recurrent vulvovaginal candidiasis. Clin Infect Dis 2005;40:1258-1262. [PubMed]
44. Bacak V, Biocina B, Starcevic B, Gertler S, Begovac J. Candida albicans endocarditis treatment with caspofungin in an HIV-infected patient--case report and review of literature. J Infect 2006;53:e11-4. Epub 2005 Nov 7. [PubMed]
45. Baddley JW, Benjamin DK, Jr., Patel M, Miro J, Athan E, Barsic B, Bouza E, Clara L, Elliott T, Kanafani Z, Klein J, Lerakis S, Levine D, Spelman D, Rubinstein E, Tornos P, Morris AJ, Pappas P, Fowler VG, Jr., Chu VH, Cabell C. Candida infective endocarditis. Eur J Clin Microbiol Infect Dis 2008a;27:519-529. [PubMed]
46. Baddley JW, Patel M, Bhavnani SM, Moser SA, Andes DR. Association of fluconazole pharmacodynamics with mortality in patients with candidemia. Antimicrob Agents Chemother 2008b;52:3022-3028. [PubMed]
47. Baddour LM, Bettmann MA, Bolger AF, Epstein AE, Ferrieri P, Gerber MA, Gewitz MH, Jacobs AK, Levison ME, Newburger JW, Pallasch TJ, Wilson WR, Baltimore RS, Falace DA, Shulman ST, Tani LY, Taubert KA. Nonvalvular cardiovascular device-related infections. Circulation 2003;108:2015-31. [PubMed]
48. Baddour LM, Bettmann MA, Bolger AF, Epstein AE, Ferrieri P, Gerber MA, Gewitz MH, Jacobs AK, Levison ME, Newburger JW, Pallasch TJ, Wilson WR, Baltimore RS, Falace DA, Shulman ST, Tani LY, Taubert KA. Nonvalvular cardiovascular device-related infections. Clin Infect Dis 2004;38:1128-30. [PubMed]
49. Baley JE, Meyers C, Kliegman RM, Jacobs MR, Blumer JL. Pharmacokinetics, outcome of treatment, and toxic effects of amphotericin B and 5-fluorocytosine in neonates. J Pediatr 1990;116:791-7. [PubMed]
50. Banerjee SN, Emori TG, Culver DH, Gaynes RP, Jarvis WR, Horan T, Edwards JR, Tolson J, Henderson T, Marone WJ, the National Nosocomial Infections Surveillance System. Secular trends in nosocomial primary bloodstream infections in the United States, 1980-1989. Am J Med 1991;91 (Suppl. 3B):86S-89S. [PubMed]
51. Bannatyne RM, Clarke HM. Ketoconazole in the treatment of osteomyelitis due to Candida albicans. Can J Surg 1989;32:201-202.[PubMed]
52. Barchiesi F, Colombo AL, McGough DA, Fothergill AW, Rinaldi MG. In vitro activity of itraconazole against fluconazole-susceptible and -resistant Candida albicans isolates from oral cavities of patients infected with human immunodeficiency virus. Antimicrob Agents Chemother 1994;38:1530-1533. [PubMed]
53. Barenfanger J, Arakere P, Dela Cruz R, Imran A, Drake C, Lawhorn J, Verhulst SJ, Khardori N. Improved outcomes associated with limiting identification of Candida spp. in respiratory secretions. J Clin Microbiol 2003;41:5645-5649. [PubMed]
54. Barone SR, Krilov LR. Neonatal candidal meningitis in a full-term infant with congenital cutaneous candidiasis. Clinical Pediatrics 1995;April:217-219. [PubMed]
55. Barrett JP, Vardulaki KA, Conlon C, Cooke J, Daza-Ramirez P, Evans EGV, Hawkey PM, Herbrecht R, Marks DI, Moraleda JM, Park GR, Senn SJ, Viscoli C. A systematic review of the antifungal effectiveness and tolerability of amphotericin B formulations. Clin Ther 2003;25:1295-1320.[PubMed]
56. Bates DW, Yu DT. Clinical impact of drug-drug interactions with systemic azole antifungals. Drugs Today 2003;39:801-813.[PubMed]
57. Bayer AS, Blumenkrantz MJ, Montgomerie JZ, Galpin JE, Coburn JW, Guze LB. Candida peritonitis: Report of 22 cases and review of the English literature. Am J Med 1976;61:832-840. [PubMed]
58. Bayer AS, Guze LB. Fungal arthritis. I. Candida arthritis: diagnostic and prognostic implications and therapeutic considerations. Seminars in Arthritis & Rheumatism 1978;8:142-50. [PubMed]
59. Bekersky I, Fielding RM, Dressler DE, Lee JW, Buell DN, Walsh TJ. Pharmacokinetics, excretion, and mass balance of liposomal amphotericin B (AmBisome) and amphotericin B deoxycholate in humans. Antimicrob Agents Chemother 2002;46:828-833. [PubMed]
60. Benedetti E, Gruessner AC, Troppmann C, Papalois BE, Sutherland DE, Dunn DL, Gruessner RW. Intra-abdominal fungal infections after pancreatic transplantation: incidence, treatment, and outcome. J Amer Coll Surgeons 1996;183:307-316. [PubMed]
61. Benjamin DK, Jr., Driscoll T, Seibel NL, Gonzalez CE, Roden MM, Kilaru R, Clark K, Dowell JA, Schranz J, Walsh TJ. Safety and pharmacokinetics of intravenous anidulafungin in children with neutropenia at high risk for invasive fungal infections. Antimicrob Agents Chemother 2006;50:632-638. [PubMed]
62. Benjamin DK, Jr., Miro JM, Hoen B, Steinbach WJ, Fowler VG, Jr., Olaison L, Habib G, Abrutyn E, Perfect J, Zass A, Corey GR, Eykyn S, Thuny F, Jimenez-Exposito MJ, Cabell CH. Candida endocarditis: Contemporary cases from the international collaboration of infectious endocarditis merged database (ICE-MD). Scand J Infec Dis 2004;36:453-455. [PubMed] [PubMed]
63. Bennett JE. Antimicrobial agents: Antifungal agents. In: Gilman AG, Rall TW, Nies AS, Taylor P, eds. Goodman and Gilman's the pharmacological basis of therapeutics. 8th ed. ed. Fairview Park: Pergamon Press, Inc., 1990:1165-1181. [PubMed]
64. Bennett JE. Echinocandins for candidemia in adults without neutropenia. N Engl J Med 2006;355:1154-1159. [PubMed]
65. Bennett JE, Dismukes WE, Duma RJ, Medoff G, Sande MA, Gallis H, Leonard J, Fields BT, Bradshaw M, Haywood H, McGee ZA, Cate TR, Cobbs CG, Warner JF, Alling DW. A comparison of amphotericin B alone and combined with flucytosine in the treatment of cryptococcal meningitis. N Engl J Med 1979;301:126-131. [PubMed]
66. Benoit J-L, Carandang G, Sitrin M, Arnow PM. Intraluminal antibiotic treatment of central venous catheter infections in patients receiving parenteral nutrition at home. Clin Infect Dis 1995;21:1286-1288. [PubMed]
67. Beovic B, Lejko-Zupanc T, Pretnar J. Sequential treatment of deep fungal infections with amphotericin B deoxycholate and amphotericin B colloidal dispersion. Eur J Clin Microbiol Infect Dis 1997;16:507-511. [PubMed]
68. Berenguer J, Buck M, Witebsky F, Stock F, Pizzo PA, Walsh TJ. Lysis-centrifugation blood cultures in the detection of tissue-proven invasive candidiasis. Disseminated versus single-organ infection. Diagn Microbiol Infect Dis 1993;17:103-109. [PubMed]
69. Berg RA, Stein JM. Medical management of fungal suppurative thrombosis of great central veins in a child. Pediatr Infect Dis J 1989;8:469-470. [PubMed]
70. Bergman JJ. Clinical comparison of microscopic and culture techniques in the diagnosis of Candida vaginitis. J Fam Pract 1984;18:549-553. [PubMed]
71. Berkowitz FE, Argent AC, Baise T. Suppurative thrombophlebitis: a serious nosocomial infection. Pediatric Infectious Disease Journal 1987;6:64-67. [PubMed]
72. Berkowitz ID, Robboy SJ, Karchmer AW, Kunz LJ. Torulopsis glabrata fungemia--A clinical pathological study. Medicine 1979;56:430-440. [PubMed]
73. Berry AJ, Rinaldi MG, Graybill JR. Use of high-dose fluconazole as salvage therapy for cryptococcal meningitis in patients with AIDS. Antimicrob Agents Chemother 1992;36:690-692. [PubMed]
74. Bille J, Stockman G, Roberts D, Hortmeier CD, Ilstrup DM. Evaluation of a lysis-centrifugation sustem for recovery of yeasts and filamentous fungi from blood. J Clin Microbiol 1983;18:469-471. [PubMed]
75. Black JT. Cerebral candidiasis: case report of brain abscess secondary to Candida albicans, and review of literature. J Neurol Neurosurg Psychiat 1970;33:864-870. [PubMed]
76. Black KE, Baden LR. Fungal infections of the CNS - Treatment strategies for the immunocompromised patient. CNS Drugs 2007;21:293-318. [PubMed]
77. Blinkhorn RJ, Adelstein D, Spagnuolo PJ. Emergence of a new opportunistic pathogen, Candida lusitaniae. J Clin Microbiol 1989;27:236-240. [PubMed]
78. Bliss JM, Wellington M, Gigliotti F. Antifungal pharmacotherapy for neonatal candidiasis. Semin Perinatol 2003;27:365-374. [PubMed]
79. Blumberg EA, Reboli AC. Failure of systemic empirical treatment with amphotericin B to prevent candidemia in neutropenic patients with cancer. Clin Infect Dis 1996;22:462-466. [PubMed]
80. Blyth CC, Palasanthiran P, O'Brien TA. Antifungal therapy in children with invasive fungal infections: A systematic review. Pediatrics 2007;119:772-784. [PubMed]
81. Bodey GP, Luna M. Skin lesions associated with disseminated candidiasis. JAMA 1974;229:1466-1468. [PubMed]
82. Bohme A, Ruhnke M, Buchheidt D, Karthaus M, Einsele H, Guth S, Heussel G, Heussel CP, Junghanss C, Kern WK, Kubin T, Maschmeyer G, Sezer O, Silling G, Sudhoff T, Szelenyi H, Ullmann AJ. Treatment of fungal infections in hematology and oncology - Guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Oncology (DGHO). Ann Hematol 2003;82:S133-S140. [PubMed]
83. Bonomo RA, Strauss M, Blinkhorn R, Salata RA. Torulopsis (Candida) glabrata: A new pathogen found in spinal epidural abscess. Clin Infect Dis 1996;22:588-589. [PubMed]
84. Boogaerts M, Winston DJ, Bow EJ, Garber G, Reboli AC, Schwarer AP, Novitzky N, Boehme A, Chwetzoff E, De Beule K. Intravenous and oral itraconazole versus intravenous amphotericin B deoxycholate as empirical antifungal therapy for persistent fever in neutropenic patients with cancer who are receiving broad-spectrum antibacterial therapy - A randomized, controlled trial. Ann Intern Med 2001a;135:412-422. [PubMed]
85. Boogaerts MA, Maertens J, Van der Geest R, Bosly A, Michaux JL, Van Hoof A, Cleeren M, Wostenborghs R, De Beule K. Pharmacokinetics and safety of a 7-day administration of intravenous itraconazole followed by a 14-day administration of itraconazole oral solution in patients with hematologic malignancy. Antimicrob Agents Chemother 2001b;45:981-985. [PubMed]
86. Borman AM, Petch R, Linton CJ, Palmer MD, Bridge PD, Johnson EM. Candida nivariensis, an emerging pathogenic fungus with multidrug resistance to antifungal agents. J Clin Microbiol 2008;46:933-938. [PubMed]
87. Bougnoux ME, Hill C, Moissente D, de Chauvin MF, Bonnay M, Vicens-Sprauel I, Pietri F, McNeil M, Kaufman L, Dupouy-Camet J, Bohuon C, Andremonti A. Comparison of antibody, antigen, and metabolite assays for hospitalized patients with disseminated or peripheral candidiasis. J Clin Microbiol 1990;28:905-909. [PubMed]
88. Bouza E, Alvarado N, Alcala L, Perez MJ, Rincon C, Munoz P. A randomized and prospective study of 3 procedures for the diagnosis of catheter-related bloodstream infection without catheter withdrawal. Clin Infect Dis 2007a;44:820-6. [PubMed]
89. Bouza E, Sousa D, Rodriguez-Creixems M, Lechuz JG, Munoz P. Is the volume of blood cultured still a significant factor in the diagnosis of bloodstream infections? J Clin Microbiol 2007b;45:2765-2769. [PubMed]
90. Bow EJ, Laverdiere M, Lussier N, Rotstein C, Cheang MS, Ioannou S. Antifungal prophylaxis for severely neutropenic chemotherapy recipients - A meta-analysis of randomized-controlled clinical trials. Cancer 2002;94:3230-3246. [PubMed]
91. Bow EJ, Loewen R, Cheang MS, Schacter B. Invasive fungal disease in adults undergoing remission-induction therapy for acute myeloid leukemia: the pathogenetic role of the antileukemic regimen. Clin Infect Dis 1995;21:361-369. [PubMed]
92. Bozzette SA. Fluconazole prophylaxis in HIV disease, revisited. Clin Infect Dis 2005;41:1481-2. Epub 2005 Oct 12. [PubMed]
93. Brammer KW, Coates PE. Pharmacokinetics of fluconazole in pediatric patients. Eur J Clin Microbiol Infect Dis 1994;13:325-329. [PubMed]
94. Branchini ML, Pfaller MA, Rhine-Chalberg J, Frempong T, Isenberg HD. Genotypic variation and slime production among blood and catheter isolates of Candida parapsilosis. J Clin Microbiol 1994;32:452-6. [PubMed]
95. Breit SM, Hariprasad SM, Mieler WF, Shah GK, Mills MD, Grand MG. Management of endogenous fungal endophthalmitis with voriconazole and caspofungin. Amer J Ophthalmol 2005;139:135-140. [PubMed]
96. British Society for Antimicrobial Chemotherapy Working Party. Antifungal chemotherapy in patients with acquired immunodeficiency syndrome. Lancet 1992;340:648-51. [PubMed]
97. Brod RD, Flynn HW, Jr., Clarkson JG, Pflugfelder SC, Culbertson WW, Miller D. Endogenous Candida endophthalmitis. Management without intravenous amphotericin B. Ophthalmology 1990;97:666-672. [PubMed]
98. Brooks RG. Prospective study of Candida endophthalmitis in hospitalized patients with candidemia. Arch Intern Med 1989;149:2226-2228. [PubMed]
99. Bruggemann RJM, Donnelly JP, Aarnoutse RE, Warris A, Blijlevens NMA, Mouton JW, Verweij PE, Burger DM. Therapeutic drug monitoring of voriconazole. Ther Drug Monit 2008;30:403-411. [PubMed]
100. Bruner JP, Elliott JP, Kilbride HW, Garite TJ, Knox GE. Candida chorioamnionitis diagnosis by amniocentesis with subsequent fetal infection. Amer J Perinatol 1986;3:213-218. [PubMed]
101. Buchner T, Fegeler W, Bernhardt H, Brockmeyer N, Duswald KH, Herrmann M, Heuser D, Jehn U, Just-Nubling G, Karthaus M, Maschmeyer G, Muller FM, Muller J, Ritter J, Roos N, Ruhnke M, Schmalreck A, Schwarze R, Schwesinger G, Silling G. Treatment of severe Candida infections in high-risk patients in Germany: Consensus formed by a panel of interdisciplinary investigators. Eur J Clin Microbiol Infect Dis 2002;21:337-352. [PubMed]
102. Buchs S, Pfister P. Candida meningitis: course, prognosis and mortality before and after introduction of the new antimycotics. Mykosen 1982;26:73-81. [PubMed]
103. Burgert SJ, Classen DC, Burke JP, Blatter DD. Candidal brain abscess associated with vascular invasion: a devastating complication of vascular catheter-related candidemia. Clin Infect Dis 1995;21:202-205. [PubMed]
104. Burke WA. Use of itraconazole in a patient with chronic mucocutaneous candidiasis. J Amer Acad Dermatol 1989;21:1309-1310. [PubMed]
105. Calandra T, Bille J, Schneider R, Mosimann F, Francioli P. Clinical significance of Candida isolated from peritoneum in surgical patients. Lancet 1989;2:1437-1440. [PubMed]
106. Cancelas JA, Lopez J, Cabezudo E, Navas E, Garcia Laraña J, Jimenez Mena M, Diz P, Perez de Oteyza J, Villalon L, Sanchez-Sousa A, Sastre JL, Odriozola J, Navarro JL. Native valve endocarditis due to Candida parapsilosis: a late complication after bone marrow transplantation-related fungemia. Bone Marrow Transplant 1994;13:333-334. [PubMed]
107. Canton E, Peman J, Gobernado M, Viudes A, Espinel-Ingroff A. Patterns of amphotericin B killing kinetics against seven Candida species. Antimicrob Agents Chemother 2004;48:2477-82. [PubMed]
108. Cantrill HL, Rodman WP, Ramsay RC, Knobloch WH. Postpartum Candida endophthalmitis. JAMA 1980;243:1163-1166.[PubMed]
109. Cappelletty D, Eiselstein-McKitrick K. The echinocandins. Pharmacotherapy 2007;27:369-388. [PubMed]
110. Carpenter CC, Mayer KH, Fisher A, Desai MB, Durand L. Natural history of acquired immunodeficiency syndrome in women in Rhode Island. Am J Med 1989;86:771-5. [PubMed]
111. Casadevall A. The third age of antimicrobial therapy. Clin Infect Dis 2006;42:1414-1416. [PubMed]
112. Casado JL, Quereda C, Oliva J, Navas E, Morenco A, Pintado V, Cobo J, Corral I. Candidal meningitis in HIV-infected patients: Analysis of 14 cases. Clin Infect Dis 1997;25:673-676. [PubMed]
113. Cassone A, DeBernardis F, Pontieri E, Carruba G, Girmenia C, Martino P, Fernández-Rodriguez M, Quindós G, Pontón J. Biotype diversity of Candida parapsilosis and its relationship to the clinical source and experimental pathogenicity. J Infect Dis 1995;171:967-975. [PubMed]
114. Castiglia M, Smego RA, Sames EL. Candida endocarditis and amphotericin B intolerance: Potential role for fluconazole. Infect Dis Clin Pract 1994;3:248-253. [PubMed]
115. Cauda R, Tacconelli E, Tumbarello M, Morace G, De Bernardis F, Torosantucci A, Cassone A. Role of protease inhibitors in preventing recurrent oral candidosis in patients with HIV-infection: A prospective case- control study. J Acq Immun Defic Synd Hum R 1999;21:20-25. [PubMed]
116. Cenci E, Bartocci A, Puccetti P, Mocci S, Stanley ER, Bistoni F. Macrophage colony-stimulating factor in murine candidiasis: serum and tissue levels during infection and protective effect of exogenous administration. Infect Immun 1991;59:868-72. [PubMed]
117. Chandra J, Kuhn DM, Mukherjee PK, Hoyer LL, McCormick T, Ghannoum MA. Biofilm formation by the fungal pathogen Candida albicans: Development, architecture, and drug resistance. J Bacteriol 2001;183:5385-5394. [PubMed]
118. Chandrasekar PH, Gatny CM, the Bone Marrow Transplantation Team. The effect of fluconazole prophylaxis on fungal colonization in neutropenic cancer patients. J Antimicrob Chemother 1994;33:309-318. [PubMed]
119. Chandrasekar PH, Sobel JD. Micafungin: A new echinocandin. Clin Infect Dis 2006;42:1171-1178. [PubMed]
120. Chapman RL, Faix RG. Invasive neonatal candidiasis: An overview. Semin Perinatol 2003;27:352-356. [PubMed]
121. Chen TL, Chen HP, Fung CP, Lin MY, Yu KW, Liu CY. Clinical characteristics, treatment and prognostic factors of candidal meningitis in a teaching hospital in Taiwan. Scand J Infect Dis 2004;36:124-30. [PubMed]
122. Chesney PJ, Teets KC, Mulvihill JJ, Salit IE, Marks ML. Successful treatment of Candida meningitis with amphotericin b and 5-fluorocytosine in combination. J Pediatr 1976;89:1017-1018. [PubMed]
123. Chin TW, Loeb M, Fong IW. Effects of an acidic beverage (Coca-Cola) on absorption of ketoconazole. Antimicrob Agents Chemother 1995;39:1671-1675. [PubMed]
124. Chiou CC, Wong TT, Lin HH, Hwang B, Tang RB, Wu KG, Lee BH. Fungal infection of ventriculoperitoneal shunts in children. Clin Infect Dis 1994;19:1049-1053. [PubMed]
125. Clancy CJ, Nguyen MH, Morris AJ. Candidal mediastinitis: An emerging clinical entity. Clin Infect Dis 1997;25:608-613.[PubMed]
126. Clancy CJ, Yu VL, Morris AJ, Snydman DR, Nguyen MH. Fluconazole MIC and the fluconazole dose/MIC ratio correlate with therapeutic response among patients with candidemia. Antimicrob Agents Chemother 2005;49:3171-3177. [PubMed]
127. Clark JM, Whitney RR, Olsen SJ, George RJ, Swerdel MR, Kunselman L, Bonner DP. Amphotericin B lipid complex therapy of experimental fungal infections in mice. Antimicrob Agents Chemother 1991;35:615-621. [PubMed]
128. Clemons KV, Stevens DA. Efficacy of micafungin alone or in combination against experimental pulmonary aspergillosis. Med Mycol 2006;44:69-73. [PubMed]
129. Clinical and Laboratory Standards Institute. Reference method for broth dilution antifungal susceptibility testing of yeasts; Approved standard NCCLS document M27-A3. Wayne, Pa: Clinical and Laboratory Standards Institute, 2008a. [PubMed]
130. Clinical and Laboratory Standards Institute. Reference method for broth dilution antifungal susceptibilty testing of yeasts; Third informational supplement. (M27-S3). Wayne, Pa: Clinical and Laboratory Standards Institute, 2008b. [PubMed]
131. Cohen R, Roth FJ, Delgado E, Ahearn DG, Kalser MH. Fungal flora of the normal human small and large intestine. N Engl J Med 1969;280:638-41. [PubMed]
132. Collins LA, Samore MH, Roberts MS, Luzzati R, Jenkins RL, Lewis WD, Karchmer AW. Risk factors for invasive fungal infections complicating orthotopic liver transplantation. J Infect Dis 1994;170:644-652. [PubMed]
133. Colombo AL, Melo ASA, Rosas RFC, Salomao R, Briones M, Hollis RJ, Messer SA, Pfaller MA. Outbreak of Candida rugosa candidemia: an emerging pathogen that may be refractory to amphotericin B therapy. Diagn Microbiol Infect Dis 2003a;46:253-257.[PubMed]
134. Colombo AL, Perfect J, DiNubile M, Bartizal K, Motyl M, Hicks P, Lupinacci R, Sable C, Kartsonis N. Global distribution and outcomes for Candida species causing invasive candidiasis: Results from an international randomized double-blind study of caspofungin versus amphotericin B for the treatment of invasive candidiasis. Eur J Clin Microbiol Infect Dis 2003b;22:470-474.[PubMed]
135. Cone LA, Byrd RG, Potts BE, Wuesthoff M. Diagnosis and treatment of Candida vertebral osteomyelitis: clinical experience with a short course therapy of amphotericin B lipid complex. Surg Neurol 2004;62:234-7; discussion 237. [PubMed]
136. Conrad D, Lentnek AL. Comparative evaluation of nystatin pastille and clotrimazole troche for the treatment of candidal stomatitis in immunocompromised patients. Curr Therap Res 1990;47:627-636. [PubMed]
137. Corbella X, Sirvent JM, Carratala J. Fluconazole treatment without catheter removal in Candida albicans peritonitis complicating peritoneal dialysis. Am J Med 1991;90:277. [PubMed]
138. Cornely OA, Bohme A, Buchheidt D, Glasmacher A, Kahl C, Karthaus M, Kern W, Kruger W, Maschmeyer G, Ritter J, Salwender HJ, Sandherr M, Schiel X, Schuttrumpf S, Sieniawski M, Silling G, Ullmann AJ, Wolf HH. Prophylaxis of invasive fungal infections in patients with hematological malignancies and solid tumors - Guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Oncology (DGHO). Ann Hematol 2003;82:S186-S200. [PubMed]
139. Cornely OA, Maertens J, Winston DJ, Perfect J, Ullmann AJ, Walsh TJ, Helfgott D, Holowiecki J, Stockelberg D, Goh Y, Petrini M, Hardalo C, Suresh R, Angulo-Gonzalez D. Posaconazole vs. fluconazole or itraconazole prophylaxis in patients with neutropenia. N Engl J Med 2007;356:348-359.[PubMed]
140. Cota J, Carden M, Graybill JR, Najvar LK, Burgess DS, Wiederhold NP. In vitro pharmacodynamics of anidulafungin and caspofungin against Candida glabrata isolates, including strains with decreased caspofungin susceptibility. Antimicrob Agents Chemother 2006;50:3926-3928.[PubMed]
141. Cousin L, Le Berre M, Launay-Vacher V, Izzedine H, Deray G. Dosing guidelines for fluconazole in patients with renal failure. Nephrol Dialysis Transplant 2003;18:2227-2231. [PubMed]
142. Cruciani M, DiPerri G, Molesini M, Vento S, Concia E, Bassetti D. Use of fluconazole in the treatment of Candida albicans hydrocephalus shunt infection. Eur J Clin Microbiol Infect Dis 1992;11:957. [PubMed]
143. Cruciani M, Mengoli C, Malena M, Bosco O, Serpelloni G, Grossi P. Antifungal prophylaxis in liver transplant patients: A systematic review and meta-analysis. Liver Transplant 2006;12:850-858. [PubMed]
144. Cuttner J, Troy KM, Fumaro L, Brenden R, Bottone EJ. Clotrimazole treatment for prevention of oral candidiasis in patients with acute leukemia undergoing chemotherapy. Results of a double-blind study. Am J Med 1986;81:771-774. [PubMed]
145. Damjanovic V, Connolly CM, van Saene HK, Cooke RW, Corkill, J E, van Belkum A, van Velzen D. Selective decontamination with nystatin for control of a Candida outbreak in a neonatal intensive care unit. J Hospital Infect 1993;24:245-259. [PubMed]
146. Dan M, Priel I. Failure of fluconazole therapy for sternal osteomyelitis due to Candida albicans (letter). Clin Infect Dis 1994;18:126-127. [PubMed]
147. Darling K, Singh J, Wilks D. Successful treatment of Candida glabrata endophthalmitis with amphotericin B lipid complex (ABLC). J Infection 2000;40:92-94. [PubMed]
148. De Bernardis F, Mondello F, San Millan R, Ponton J, Cassone A. Biotyping and virulence properties of skin isolates of Candida parapsilosis. J Clin Microbiol 1999;37:3481-3486. [PubMed]
149. De Bernardis F, Sullivan PA, Cassone A. Aspartyl proteinases of Candida albicans and their role in pathogenicity. Med Mycol 2001;39:303-13. [PubMed]
150. De Doncker P, Decroix J, Pierard GE, Roelant D, Woestenborghs R, Jacqmin P, Odds F, Heremans A, Dockx P, Roseeuw D. Antifungal pulse therapy for onychomycosis. A pharmacokinetic and pharmacodynamic investigation of monthly cycles of 1-week pulse therapy with itraconazole. Arch Dermatol 1996;132:34-41. [PubMed]
151. de Doncker P, van Lint J, Dockx P, Roseeuw D. Pulse therapy with one-week itraconazole monthly for three or four months in the treatment of onychomycosis. Cutis 1995;56:180-183. [PubMed]
152. de la Torre P, Reboli AC. Anidulafungin: a new echinocandin for candidal infections. Expert Rev Anti-Infect Ther 2007;5:45-52.[PubMed]
153. De Punzio C, Garutti P, Mollica G, Nappi C, Piccoli R, Genazzani AR. Fluconazole 150 mg single dose versus itraconazole 200 mg per day for 3 days in the treatment of acute vaginal candidiasis: a double-blind randomized study. Eur J Obstet Gyn Reprod Biol 2003;106:193-197. [PubMed]
154. De Socio GVL, Fiorio M, Stagni G. AmBisome administration for Candida albicans shunt infections. J Antimicrob Chemother 2003;52:1048-1049. [PubMed]
155. de Wet N, Llanos-Cuentas A, Suleiman J, Baraldi E, Krantz EF, Negra MD, Diekmann-Berndt H. A randomized, double-blind, parallel-group, dose-response study of micafungin compared with fluconazole for the treatment of esophageal candidiasis in HIV-positive patients. Clin Infect Dis 2004;39:842-9. Epub 2004 Aug 27. [PubMed]
156. de Wet NTE, Bester AJ, Viljoen JJ, Filho F, Suleiman JM, Ticona E, Llanos EA, Fisco C, Lau W, Buell D. A randomized, double blind, comparative trial of micafungin (FK463) vs. fluconazole for the treatment of oesophageal candidiasis. Aliment Pharmacol Therapeut 2005;21:899-907.[PubMed]
157. Debruyne D, Ryckelynck J-P, Moulin M, Hurault de Ligny B, Levaltier B, Bigot M-C. Pharmacokinetics of fluconazole in patients undergoing continuous ambulatory peritoneal dialysis. Clin Pharmacokinet 1990;18:491-498. [PubMed]
158. DeGregorio MW, Lee WMF, Ries CA. Candida infections in patients with acute leukemia: ineffectiveness of nystatin prophylaxis and relationship between oropharyngeal and systemic candidiasis. Cancer 1982;50:2780-2784. [PubMed]
159. Denning DW, Kibbler CC, Barnes RA. British Society for Medical Mycology proposed standards of care for patients with invasive fungal infections. Lancet Infect Dis 2003;3:230-240. [PubMed]
160. Deresinski SC, Stevens DA. Caspofungin. Clin Infect Dis 2003;36:1445-1457. [PubMed]
161. Desai MH, Rutan RL, Heggers JP, Herndon DN. Candida infection with and without nystatin prophylaxis. An 11-year experience with patients with burn injury. Arch Surg 1992;127:159-162. [PubMed]
162. DeVita VT, Utz JP, Williams T, Carbone PP. Candida meningitis. Arch Intern Med 1966;117:527-535. [PubMed]
163. Dewsnup DH, Stevens DA. Efficacy of oral amphotericin B in AIDS patients with thrush clinically resistant to fluconazole. J Med Vet Mycol 1994;32:389-393. [PubMed]
164. Dick J, Merz W, Saral R. Incidence of polyene-resistant yeasts recovered from clinical specimens. Antimicrob Agents Chemother 1980;18:158-163.[PubMed]
165. Dignani MC, Anaissie EJ, Hester JP, S OB, Vartivarian SE, Rex JH, Kantarjian H, Jendiroba DB, Lichtiger B, Andersson BS, Freireich EJ. Treatment of neutropenia-related fungal infections with granulocyte colony-stimulating factor-elicited white blood cell transfusions: a pilot study. Leukemia 1997;11:1621-1630.[PubMed]
166. Dijkmans BAC, Koolen MI, Mouton RP, Falke M, van den Broek PJ, van der Meer JWM. Hematogenous Candida vertebral osteomyelitis treated with ketoconazole. Infection 1982;10:290-292. [PubMed]
167. DiNubile MJ, Lupinacci RJ, Berman RS, Sable CA. Response and relapse rates of candidal esophagitis in HIV-infected patients treated with caspofungin. AIDS Res Hum Retrovirus 2002;18:903-908. [PubMed]
168. Dixon DL, Breeding LC, Faler TA. Microwave disinfection of denture base materials colonized with Candida albicans. J Prosthet Dent 1999;81:207-14. [PubMed]
169. Donahue SP, Greven CM, Zuravleff JJ, Eller AW, Nguyen MH, Peacock JE, Wagener MM, Yu VL. Intraocular candidiasis in patients with candidemia: Clinical implications derived from a prospective multicenter study. Ophthalmology 1994;101:1302-1309.[PubMed]
170. Donahue SP, Hein E, Sinatra RB. Ocular involvement in children with candidemia. Amer J Ophthalmol 2003;135:886-887.[PubMed]
171. Dowell JA, Stogniew M, Krause D, Damle B. Anidulafungin does not require dosage adjustment in subjects with varying degrees of hepatic or renal impairment. J Clin Pharmacol 2007;47:461-470. [PubMed]
172. Driessen M, Ellis JB, Cooper PA, Wainer S, Muwazi F, Hahn D, Gous H, De Villiers FP. Fluconazole vs. amphotericin B for the treatment of neonatal fungal septicemia: a prospective randomized trial. Pediatric Infectious Disease Journal 1996;15:1107-1112.[PubMed]
173. Drouhet E. Basic mechanisms of antifungal chemotherapy. Mod Treat 1970;7:539-564.[PubMed]
174. Drutz DJ, Lehrer RI. Development of amphotericin B-resistant Candida tropicalis in a patient with defective leukocyte function. Am J Med Sci 1978;276:77-92. [PubMed]
175. Duerr A, Heilig CM, Meikle SF, Cu-Uvin S, Klein RS, Rompalo A, Sobel JD. Incident and persistent vulvovaginal candidiasis among human immunodeficiency virus-infected women: Risk factors and severity. Obstet Gynecol 2003;101:548-556. [PubMed]
176. Duerr A, Sierra MF, Feldman J, Clarke LM, Ehrlich I, DeHovitz J. Immune compromise and prevalence of Candida vulvovaginitis in human immunodeficiency virus-infected women. Obstet Gynecol 1997;90:252-6. [PubMed]
177. Duquesnoy B, Fournier E, Berniere L, Delcambre B. Ketoconazole for treatment of Candida arthritis [letter]. J Rheumatol 1984;11:105-7. [PubMed]
178. Duswald K-H, Penk A, Pittrow L. High-dose therapy with fluconazole >= 800 mg/day. Mycoses 1997;40:267-277. [PubMed]
179. Dykewicz CA, Jaffe HW, Spira TJ, Jarvis WR, Kaplan JE, Edlin BR, Chen RT, Hibbs B, Bowden RA, Sullivan KM, Emanuel D, Longworth DL, Rowlings PA, Rubin RH, Sepkowitz KA, Wingard JR, Modlin JR, Ambrosino DM, Baylor NW, Donnenberg AD, Gardner P, Giller RH, Halsey NA, Le CT, Molrine DC. Guidelines for preventing opportunistic Infections among hematopoietic stem cell transplant recipients. Recommendations of CDC, the Infectious Disease Society of America, and the American Society of Blood and Marrow Transplantation. MMWR 2000;49 (RR10):1-128. [PubMed]
180. Edmond MB, Wallace SE, McClish DK, Pfaller MA, Jones RN, Wenzel RP. Nosocomial bloodstream infections in United States hospitals: A three-year analysis. Clin Infect Dis 1999;29:239-244.[PubMed]
181. Edwards JE. Editorial Response: Should all patients with candidemia be treated with antifungal agents? Clin Infect Dis 1992;15:422-423. [PubMed]
182. Edwards JE, Jr., Foos RY, Montgomerie JZ, Guze LB. Ocular manifestations of Candida septicemia: Review of seventy-six cases of hematogenous Candida endophthalmitis. Medicine 1974;53:47-75. [PubMed]
183. Edwards JF, Jr., Turkel S, Elder HA, Rand RW, Guze LB. Hematogenous Candida osteomyelitis: Report of three cases and review of the literature. Am J Med 1975;59:89-94. [PubMed]
184. Eggimann P, Francioli P, Bille J, Schneider R, Wu M-W, Chapuis G, Chiolero R, Pannatier A, Schilling J, Geroulanos S, Glauser MP, Calandra T. Fluconazole prophylaxis prevents intraabdominal candidiasis in high-risk surgical patients. Crit Care Med 1999;27:1066-1072. [PubMed]
185. Eggimann P, Garbino J, Pittet D. Epidemiology of Candida species infections in critically ill non-immunosuppressed patients. Lancet Infect Dis 2003a;3:685-702. [PubMed]
186. Eggimann P, Garbino J, Pittet D. Management of Candida species infections in critically ill patients. Lancet Infect Dis 2003b;3:772-785. [PubMed]
187. Eichel M, Just-Nubling G, Helm EB, Stille W. Itraconazole suspension in the treatment of HIV-infected patients with fluconazole-resistant oropharyngeal candidiasis and esophagitis. Mycoses 1996;39 (Suppl. 1):102-106. [PubMed]
188. Eisenberg ES. Intraperitoneal flucytosine in the management of fungal peritonitis in patients on continuous ambulatory peritoneal dialysis. Am J Kidney Dis 1988;11:465-7.[PubMed]
189. Eisenberg ES, Leviton I, Soeiro R. Fungal peritonitis in patients receiving peritoneal dialysis: experience with 11 patients and review of the literature. Rev Infect Dis 1986;8:309-321. [PubMed]
190. El-Ebiary M, Torres A, Fabrega N, Puig de la Bellacasa J, Gonzalez J, Ramirez J, del Bano D, Hernandez C, Jimenez de Anta MT. Significance of the isolation of Candida species from respiratory samples in critically ill, non-neutropenic patients. Am J Respir Crit Care Med 1997;156:583-590. [PubMed]
191. Elewski BE. Once-weekly fluconazole in the treatment of onychomycosis: Introduction. J Amer Acad Dermatol 1998;38:S73-S76.[PubMed]
192. Ellis ME, Al-Abdely H, Sandridge A, Greer W, Ventura W. Fungal endocarditis: Evidence in the world literature, 1965-1995. Clin Infect Dis 2001;32:50-62. [PubMed]
193. Endophthalmitis Vitrectomy Study Group. Results of the Endophthalmitis Vitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Arch Ophthalmol 1995;113:1479-1496. [PubMed]
194. Eng RHK, Sen P, Browne K, Louria DB. Candida pericarditis. Am J Med 1982;70:867-869. [PubMed]
195. Eras P, Goldstein MJ, Sherlock P. Candida infections of the gastrointestinal tract. Medicine 1972;51:367-379. [PubMed]
196. Essman TF, Flynn HW, Jr., Smiddy WE, Brod RD, Murray TG, Davis JL, Rubsamen PE. Treatment outcomes in a 10-year study of endogenous fungal endophthalmitis. Ophthalmic Surg Lasers 1997;28:185-94. [PubMed]
197. EUCAST-AFST. EUCAST Definitive Document EDef 7.1: method for the determination of broth dilution MICs of antifungal agents for fermentative yeasts. Clin Microbiol Infect 2008a;14:398-405. [PubMed]
198. EUCAST-AFST. EUCAST technical note on fluconazole. Clin Microbiol Infect 2008b;14:193-5. [PubMed]
199. Evans EGV. Causative pathogens in onychomycosis and the possibility of treatment resistance: A review. J Amer Acad Dermatol 1998;38:S32-S36. [PubMed]
200. Faix RG. Systemic Candida infections in infants in intensive care nurseries: High incidence of central nervous system involvement. J Pediatr 1984;105:616-622. [PubMed]
201. Faix RG. Invasive neonatal candidiasis: comparison of albicans and parapsilosis infection. Pediatr Infect Dis J 1992a;11:88-93. [PubMed]
202. Faix RG. Nonsurgical treatment of Candida endocarditis. J Pediatr 1992b;120:665-666. [PubMed]
203. Faix RG, Chapman RL. Central nervous system candidiasis in the high-risk neonate. Semin Perinatol 2003;27:384-392. [PubMed]
204. Faix RG, Feick HJ, Frommelt P, Snider AR. Successful medical treatment of Candida parapsilosis endocarditis in a premature infant. Am J Perinatol 1990;7:272-5.[PubMed]
205. Faix RG, Naglie RA, Barr M, Jr. Intrapleural inoculation of Candida in an infant with congenital cutaneous candidiasis. Amer J Perinatol 1986;3:119-122. [PubMed]
206. Fan-Havard P, O'Donovan C, Smith SM, Oh J, Bamberger M, Eng RHK. Oral fluconazole versus amphotericin B bladder irrigation for treatment of candidal funguria. Clin Infect Dis 1995;21:960-965. [PubMed]
207. Fatkenheuer G, Buchheidt D, Cornely OA, Fuhr HG, Karthaus M, Kisro J, Leithauser M, Salwender H, Sudhoff T, Szelenyi H, Weissinger F. Central venous catheter (CVC)-related infections in neutropenic patients - Guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Oncology (DGHO). Ann Hematol 2003;82:S149-S157. [PubMed]
208. Ferra C, Doebbeling BN, Hollis RJ, Pfaller MA, K LC, Gingrich RD. Candida tropicalis vertebral osteomyelitis: A late sequela of fungemia. Clin Infect Dis 1994;19:697-703. [PubMed]
209. Ferris DG, Nyirjesy P, Sobel JD, Soper D, Pavletic A, Litaker MS. Over-the-counter antifungal drug misuse associated with patient-diagnosed vulvovaginal candidiasis. Obstet Gynecol 2002;99:419-25. [PubMed]
210. Fichtenbaum CJ, Koletar S, Yiannoutsos C, Holland F, Pottage J, Cohn SE, Walawander A, Frame P, Feinberg J, Saag M, Van der Horst C, Powderly WG. Refractory mucosal candidiasis in advanced human immunodeficiency virus infection. Clin Infect Dis 2000;30:749-56. [PubMed]
211. Fidel PL, Jr. History and new insights into host defense against vaginal candidiasis. Trends Microbiol 2004;12:220-227. [PubMed]
212. Fidel PL, Jr., Sobel JD. Immunopathogenesis of recurrent vulvovaginal candidiasis. Clin Microbiol Rev 1996;9:335-348. [PubMed]
213. Fidel PL, Jr., Vazquez JA, Sobel JD. Candida glabrata: Review of epidemiology, pathogenesis, and clinical disease with comparison to C. albicans. Clin Microbiol Rev 1999;12:80-96,CP2. [PubMed]
214. Fisher EW, Richards A, Anderson G, Albert DM. Laryngeal candidiasis: a cause of airway obstruction in the immunocompromised child. J Laryngol Otol 1992;106:168-170. [PubMed]
215. Fisher JF, Hicks BC, Dipiro JT, Venable J, Fincher RM. Efficacy of a single intravenous dose of Amphotericin B in urinary tract infections caused by Candida. J Infect Dis 1987;156:685-686. [PubMed]
216. Fisher JF, Newman CL, Sobel JD. Yeast in the urine: solutions for a budding problem. Clin Infect Dis 1995;20:183-189. [PubMed]
217. Fisher JF, Taylor AT, Clark J, Raghunatha R. Penetration of amphotericin B into the human eye. The Journal of Infectious Diseases 1983;147:164. [PubMed]
218. Fisher JF, Woeltje K, Espinel-Ingroff A, Stanfield J, DiPiro JT. Efficacy of a single intravenous dose of amphotericin B for Candida urinary tract infections: further favorable experience. Clin Microbiol Infect 2003;9:1024-7.[PubMed]
219. Flynn PM, Cunningham CK, Kerkering T, San Jorge AR, Peters VB, Pitel PA, Harris J, Gilbert G, Catagnaro L, Robinson P, the Multicenter Fluconazole Study Group. Oropharyngeal candidiasis in immunocompromised children: a randomized, multicenter study of orally administered fluconazole suspension versus nystatin. J Pediatr 1995;127:322-328. [PubMed]
220. Fogarty M. Candidial osteomyelitis: a case report. Aust N Z J Surg 1983;53:141-143. [PubMed]
221. Fohrer C, Fornecker L, Nivoix Y, Cornila C, Marinescu C, Herbrecht R. Antifungal combination treatment: a future perspective. Int J Antimicrobial Agents 2006;27:S25-S30. [PubMed]
222. Forrest GN, Mankes K, Jabra-Rizk MA, Weekes E, Johnson JK, Lincalis DP, Venezia RA. Peptide nucleic acid fluorescence in situ hybridization-based identification of Candida albicans and its impact on mortality and antifungal therapy costs. J Clin Microbiol 2006;44:3381-3383. [PubMed]
223. Fraser VJ, Jones M, Dunkel J, Storfer S, Medoff G, Dunagan WC. Candidemia in a tertiary care hospital: epidemiology, risk factors, and predictors of mortality. Clin Infect Dis 1992;15:414-421. [PubMed]
224. Friedland IR. Peripheral thrombophlebitis caused by Candida. Pediatr Infect Dis J 1996;15:375-377. [PubMed]
225. Fuhrmann V, Schenk P, Jaeger W, Miksits M, Kneidinger N, Warszawska J, Holzinger U, Kitzberger R, Thalhammer F. Pharmacokinetics of voriconazole during continuous venovenous haemodiafiltration. J Antimicrob Chemother 2007;60:1085-1090. [PubMed]
226. Gallo WJ, Shapiro DN, Moss M. Suppurative candidiasis: review of the literature and report of case. Journal of the American Dental Association 1976;92:936-939.[PubMed]
227. Garbino J, Lew DP, Romand JA, Hugonnet S, Auckenthaler R, Pittet D. Prevention of severe Candida infections in nonneutropenic, high- risk, critically ill patients: a randomized, double-blind, placebo-controlled trial in patients treated by selective digestive decontamination. Intens Care Med 2002;28:1708-1717. [PubMed]
228. Garcia-Effron G, Katiyar SK, Park S, Edlind TD, Perlin DS. A naturally occurring proline-to-alanine amino acid change in Fks1p in Candida parapsilosis, Candida orthopsilosis, and Candida metapsilosis accounts for reduced echinocandin susceptibility. Antimicrob Agents Chemother 2008;52:2305-2312. [PubMed]
229. Garey KW, Rege M, Pai MP, Mingo DE, Suda KJ, Turpin RS, Bearden DT. Time to initiation of fluconazole therapy impacts mortality in patients with candidemia: A multi-institutional study. Clin Infect Dis 2006;43:25-31. [PubMed]
230. Garzoni C, Nobre VA, Garbino J. Candida parapsilosis endocarditis: a comparative review of the literature. Eur J Clin Microbiol Infect Dis 2007;26:915-926. [PubMed]
231. Gathe JGJ, Harris RL, Garland B, Bradshaw MW, Williams TW. Candida osteomyelitis: report of five cases and review of the literature. Am J Med 1987;82:927-937.[PubMed]
232. Gaur AH, Flynn PM, Giannini MA, Shenep JL, Hayden RT. Difference in time to detection: A simple method to differentiate catheter-related from non-catheter-related bloodstream infection in immunocompromised pediatric patients. Clin Infect Dis 2003;37:469-475. [PubMed]
233. Geers TA, Gordon SM. Clinical significance of Candida species isolated from cerebrospinal fluid following neurosurgery. Clin Infect Dis 1999;28:1139-1147. [PubMed]
234. Gentry LO, McNitt TR, Kaufman L. Use and value of serologic tests for the diagnosis of systemic candidiasis in cancer patients: a prospective study of 146 patients. Current Microbiology 1978;1:239-242. [PubMed]
235. Gentry LO, Wilkinson ID, Lea AS, Price MF. Latex agglutination test for detection of Candida antigen in atients with disseminated disease. Eur J Clin Microbiol Infect Dis 1983;2:122-128. [PubMed]
236. Ghannoum MA, Fu Y, Ibrahim AS, Mortara LA, Shafiq MC, Edwards JE, Jr., Criddle RS. In vitro determination of optimal antifungal combinations against Cryptococcus neoformans and Candida albicans. Antimicrob Agents Chemother 1995;39:2459-2465. [PubMed]
237. Gilbert HM, Peters ED, Lang SJ, Hartman BJ. Successful treatment of fungal prosthetic valve endocarditis: Case report and review. Clin Infect Dis 1996;22:348-354.[PubMed]
238. Girmenia C, Martino P, De Bernardis F, Gentile G, Boccanera M, Monaco M, Antonucci G, Cassone A. Rising incidence of C. parapsilosis fungemia in patients with hematologic malignancies: Clinical aspects, predisposing factors, and differential pathogenicity of the causative strains. Clin Infect Dis 1996;23:506-514. [PubMed]
239. Glasmacher A, Hahn C, Molitor E, Marklein G, Sauerbruch T, Schmidt-Wolf IGH. Itraconazole trough concentrations in antifungal prophylaxis with six different dosing regimens using hydroxypropyl-beta- cyclodextrin oral solution or coated-pellet capsules. Mycoses 1999;42:591-600. [PubMed]
240. Glasmacher A, Hahn C, Molitor E, Sauerbruch T, Marklein G, Schmidt-Wolf IGH. Definition of an itraconazole target concentration for antifungal prophylaxis. 40th Interscience Conference on Antimicrobial Agents and Chemotherapy. Toronto, CA, 2000, Abstract No. 700. [PubMed]
241. Glasmacher A, Prentice A, Gorschluter M, Engelhart S, Hahn C, Djulbegovic B, Schmidt-Wolf IGH. Itraconazole prevents invasive fungal infections in neutropenic patients treated for hematologic malignancies: Evidence from a meta-analysis of 3,597 patients. J Clin Oncol 2003;21:4615-4626. [PubMed]
242. Glassman BD, Muglia JJ. Widespread erythroderma and desquamation in a neonate. Congenital cutaneous candidiasis (CCC). Arch Dermatol 1993;129:897-902. [PubMed]
243. Goicoechea M, Fierer J, Johns S. Treatment of candidal cholangitis with caspofungin therapy in a patient with a liver transplant: Documentation of biliary excretion of caspofungin. Clin Infect Dis 2004;38:1040-1041. [PubMed]
244. Goldie SJ, Kiernan-Tridle L, Torres C, Gorban-Brennan N, Dunne D, Kliger AS, Finkelstein FO. Fungal peritonitis in a large chronic peritoneal dialysis population: a report of 55 episodes. Am J Kidney Dis 1996;28:86-91. [PubMed]
245. Goldman M, Cloud GA, Wade KD, Reboli AC, Fichtenbaum CJ, Hafner R, Sobel JD, Powderly WG, Patterson TF, Wheat LJ, Stein DK, Dismukes WE, Filler SG. A randomized study of the use of fluconazole in continuous versus episodic therapy in patients with advanced HIV infection and a history of oropharyngeal candidiasis: AIDS Clinical Trials Group Study 323/Mycoses Study Group Study 40. Clin Infect Dis 2005;41:1473-80. [PubMed]
246. Goldman M, Filler SG, Cloud GA, ACTG 323 and MSG 40 Study Group. Randomized study of long-term chronic suppressive fluconazole vs. episodic fluconazole for patients with advanced HIV infection and a history of oropharyngeal candidiasis. 42th Interscience Conference on Antimicrobial Agents and Chemotherapy. San Diego, CA, 2002, Abstract No. M-1241. [PubMed]
247. Goldman M, Pottage JC, Weaver DC. Candida krusei fungemia. Medicine (Baltimore) 1993;72:143-150. [PubMed]
248. Goldman RD, Ong M, Wolpin J, Doyle J, Parshuram C, Koren G. Pharmacological risk factors for amphotericin B nephrotoxicity in children. J Clin Pharmacol 2007;47:1049-1054. [PubMed]
249. Goodman DF, Stern WH. Oral ketoconazole and intraocular amphotericin B for treatment of postoperative Candida parapsilosis endophthalmitis [letter]. Arch Ophthalmol 1987;105:172-3. [PubMed]
250. Goodman JL, Winston DJ, Greenfield RA, Chandrasekar PH, Fox B, Kaizer H, Shadduck FK, Shea TC, Stiff P, Friedman DJ, Powderly WG, Silber JL, Horowitz H, Lichtin A, Wolff SN, Mangan KF, Silver SM, Weisdorf D, Ho WG, Gilbert G, Buell D. A controlled trial of fluconazole to prevent fungal infections in patients undergoing bone marrow transplantation. N Engl J Med 1992;326:845-851. [PubMed]
251. Graninger W, Presteril E, Schneeweiss B, Teleky B, Georgopoulos A. Treatment of Candida albicans fungaemia with fluconazole. J Infect 1993;16:133-146. [PubMed]
252. Grant SM, Clissold SP. Fluconazole. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic potential in superficial and systemic mycoses. Drugs 1990;39:877-916. [PubMed]
253. Graybill JR, Bocanegra R, Najvar LK, Hernandez S, Larsen RA. Addition of caspofungin to fluconazole does not improve outcome in murine candidiasis. Antimicrob Agents Chemother 2003;47:2373-2375. [PubMed]
254. Graybill JR, Vazquez J, Darouiche RO, Morhart R, Greenspan D, Tuazon C, Wheat LJ, Carey J, Leviton I, Hewitt RG, MacGregor RR, Valenti W, Restrepo M, Moskovitz BL. Randomized trial of itraconazole oral solution for oropharyngeal candidiasis in HIV/AIDS patients. Am J Med 1998;104:33-39. [PubMed]
255. Greenfield RA, Bussey MJ, Stephens JL, Jones JM. Serial enzyme-linked immunosorbent assays for antibody to Candida antigens during induction chemotherapy for acute leukemia. J Infect Dis 1983;148:275-283. [PubMed]
256. Greenspan D. Treatment of oropharyngeal candidiasis in HIV-positive patients. J Amer Acad Dermatol 1994;31 (Suppl. 2):S51-S55. [PubMed]
257. Grewe M, Tsiotos GG, de-Leon EL, Sarr MG. Fungal infection in acute necrotizing pancreatitis. J Amer Coll Surgeons 1999;188:408-414. [PubMed]
258. Gripshover BM, Valdez H, Salata RA, Lederman MM. Withdrawal of fluconazole suppressive therapy for thrush in patients responding to combination antiviral therapy including protease inhibitors. Aids 1998;12:2513-2514. [PubMed]
259. Groll AH, Giri N, Petraitis V, Petraitiene R, Candelario M, Bacher JS, Piscitelli SC, Walsh TJ. Comparative efficacy and distribution of lipid formulations of amphotericin B in experimental Candida albicans infection of the central nervous system. J Infec Dis 2000;182:274-282. [PubMed]
260. Groll AH, Piscitelli SC, Walsh TJ. Antifungal pharmacodynamics: Concentration-effect relationships in vitro and in vivo. Pharmacotherapy 2001;21:133S-148S. [PubMed]
261. Gronemeyer PS, Weissfeld AS, Sonnenwirth AC. Purulent pericarditis complicating systemic infection with Candida tropicalis. Am J Clin Path 1982;77:471-475. [PubMed]
262. Gudlaugsson O, Gillespie S, Lee K, Berg JV, Hu JF, Messer S, Herwaldt L, Pfaller M, Diekema D. Attributable mortality of nosocomial candidemia, revisited. Clin Infect Dis 2003;37:1172-1177. [PubMed]
263. Guinet R, Chanas J, Goullier A, Bennefoy G, Ambroise-Thomas P. Fatal septicemia due to amphotericin B-resistant Candida lusitaniae. J Clin Microbiol 1983;18:443-444.[PubMed]
264. Guiot HFL, Fibbe WE, van't Wout JW. Prevention of invasive candidiasis by fluconazole in patients with malignant hematological disorders and a high grade of Candida. 36th Interscience Conference on Antimicrobial Agents and Chemotherapy. New Orleans, LA, 1996, Abstract No. LM33. [PubMed]
265. Gumbo T. Impact of pharmacodynamics and pharmacokinetics on echinocandin dosing strategies. Curr Opin Infect Dis 2007;20:587-591. [PubMed]
266. Gupta NM, Chaudhary A, Talwar P. Candidial obstruction of the common bile duct. British Journal of Surgery 1985;72:13. [PubMed]
267. Gupta TP, Ehrinpreis MN. Candida-associated diarrhea in hospitalized patients. Gastroenterology 1990;98:780-785. [PubMed]
268. Gurses N, Kalayci AG. Fluconazole monotherapy for candidal meningitis in a premature infant. Clin Infect Dis 1996;23:645-646. [PubMed]
269. Hague RA, Eastham EJ, Lee RE, Cant AJ. Resolution of hepatic abscess after interferon gamma in chronic granulomatous disease [see comments]. Archives of Disease in Childhood 1993;69:443-5. [PubMed]
270. Hajdu R, Thompson R, Sundelof JG, Pelak BA, Bouffard FA, Dropinski JF, Kropp H. Preliminary animal pharmacokinetics of the parenteral antifungal agent MK-0991 (L-743,872). Antimicrob Agents Chemother 1997;41:2339-2344. [PubMed]
271. Hakki M, Staab JF, Marr MA. Emergence of a Candida krusei isolate with reduced susceptibility to caspofungin during therapy. Antimicrob Agents Chemother 2006;50:2522-2524. [PubMed]
272. Hallum JL, Williams TW, Jr. Candida endocarditis. In: Bodey GP, ed. Candidiasis: Pathogenesis, diagnosis, and treatment. New York: Raven Press, Ltd., 1993:357-369.[PubMed]
273. Hamood M, Bluche PF, De Vroey C, Corazza F, Bujan W, Fondu P. Effects of recombinant human granulocyte-colony stimulating factor on neutropenic mice infected with Candida albicans: acceleration of recovery from neutropenia and potentiation of anti-C. albicans resistance. Mycoses 1994;37:93-9. [PubMed]
274. Hamory BH, Wenzel RP. Hospital-associated candiduria: predisposing factors and review of the literature. J Urol 1978;120:444-448. [PubMed]
275. Hardin TC, Graybill JR, Fetchick R, Woestenborghs R, Rinaldi MG, Kuhn JG. Pharmacokinetics of itraconazole following oral administration to normal volunteers. Antimicrob Agents Chemother 1988;32:1310-1313. [PubMed]
276. Hariprasad SM, Mieler WF, Lin TK, Sponsel WE, Graybill JR. Voriconazole in the treatment of fungal eye infections: a review of current literature. Brit J Ophthalmol 2008;92:871-878. [PubMed]
277. Haron E, Feld R, Tuffnell P, Patterson B, Hasselback R, Matlow A. Hepatic candidiasis: An increasing problem in immunocompromised patients. Am J Med 1987;83:17-26.[PubMed]
278. Haron E, Vartivarian S, Anaissie E, Dekmezian R, Bodey GP. Primary Candida pneumonia. Medicine 1993;72:137-142. [PubMed]
279. Haubrich RH, Haghighat D, Bozzette SA, Tilles J, McCutchan JA, the California Collaborative Treatment Group. High-dose fluconazole for treatment of cryptococcal disease in patients with human immunodeficiency virus infection. J Infect Dis 1994;170:238-242. [PubMed]
280. Havlir DV, Dube MP, McCutchan JA, Forthal DN, Kemper CA, Dunne MW, Parenti DM, Kumar PN, White AC, Witt MD, Nightingale SD, Sepkowitz KA, MacGregor RR, Cheeseman SH. Prophylaxis with weekly versus daily fluconazole for fungal infections in patients with AIDS. Clin Infect Dis 1998;27:1369-1375. [PubMed]
281. Hawser SP, Douglas LJ. Biofilm formation by Candida species on the surface of catheter materials in vitro. Infect Immun 1994;62:915-21. [PubMed]
282. Hay RJ, Clayton YM, Moore MK, Midgely G. An evaluation of itraconazole in the management of onychomycosis. Br J Dermatol 1988;119:359-66. [PubMed]
283. Hegener P, Troke PF, Fatkenheuer G, Diehl V, Ruhnke M. Treatment of fluconazole-resistant candidiasis with voriconazole in patients with AIDS. AIDS 1998;12:2227-2228. [PubMed]
284. Hendrickx L, Van Wijngaerden E, Samson I, Peetermans WE. Candidal vertebral osteomyelitis: Report of 6 patients, and a review. Clin Infect Dis 2001;32:527-533.[PubMed]
285. Hennequin C, Bouree P, Hiesse C, Dupont B, Charpentier B. Spondylodiskitis due to Candida albicans: Report of two patients who were successfully treated with fluconazole and review of the literature. Clin Infect Dis 1996;23:176-178. [PubMed]
286. Hepburn MJ, Pennick GJ, Sutton DA, Crawford GE, Jorgensen JH. Candida krusei renal cyst infection and measurement of amphotericin B levels in cystic fluid in a patient receiving AmBisome. Med Mycol 2003;41:163-5. [PubMed]
287. Heresi GP, Gerstmann DR, Reed MD, van den Anker JN, Blumer JL, Kovanda L, Keirns JJ, Buell DN, Kearns GL. The pharmacokinetics and safety of micafungin, a novel echinocandin, in premature infants. Pediat Inf Dis J 2006;25:1110-1115. [PubMed]
288. Hernandez JA, Gonzalez-Moreno M, Llibre JM, Aloy A, Casan JM. Candidal mitral endocarditis and long-term treatment with fluconazole in a patient with human immunodeficiency virus infection. Clin Infect Dis 1992;15:1062-1063.[PubMed]
289. Hernandez S, Lopez-Ribot JL, Najvar LK, McCarthy DI, Bocanegra R, Graybill JR. Caspofungin resistance in Candida albicans: Correlating clinical outcome with laboratory susceptibility testing of three is genic isolates serially obtained from a patient with progressive Candida esophagitis. Antimicrob Agents Chemother 2004;48:1382-1383. [PubMed]
290. Heykants J, Van Peer A, Van de Velde V, Van Rooy P, Meuldermans W, Kavrijsen K, Woestenborghs R, Van Cutsem J, Cauwenbergh G. The clinical pharmacokinetics of itraconazole: An overview. Mycoses 1989;32 (Suppl. 1):67-87. [PubMed]
291. Hmoud J, Chiu L, Carver P, Bielaczyc A, Kauffman CA. Candida glabrata fungemia over 9 years in a tertiary care medical center. 41st Annual Meeting of the Infectious Diseases Society of America. San Diego, 2003, Abstract No. 348. [PubMed]
292. Hoerauf A, Hammer S, Muller-Myhsok B, Rupprecht H. Intra-abdominal Candida infection during acute necrotizing pancreatitis has a high prevalence and is associated with increased mortality. Crit Care Med 1998;26:2010-2015. [PubMed]
293. Hogeweg M, de Jong PT. Candida endophthalmitis in heroin addicts. Documenta Ophthalmologica 1983;55:63-71. [PubMed]
294. Hong Y, Shaw PJ, Nath CE, Yadav SP, Stephen KR, Earl JW, McLachlan AJ. Population pharmacokinetics of liposomal amphotericin B in pediatric patients with malignant diseases. Antimicrob Agents Chemother 2006;50:935-942. [PubMed]
295. Hope WW, Mickiene D, Petraitis V, Petraitiene R, Kelaher AM, Hughes JE, Cotton MP, Bacher J, Keirns JJ, Buell D, Heresi G, Benjamin DK, Jr., Groll AH, Drusano GL, Walsh TJ. The pharmacokinetics and pharmacodynamics of micafungin in experimental hematogenous Candida meningoencephalitis: Implications for echinocandin therapy in neonates. J Infec Dis 2008;197:163-171. [PubMed]
296. Hope WW, Seibel NL, Schwartz CL, Arrieta A, Flynn P, Shad A, Albano E, Keirns JJ, Buell DN, Gumbo T, Drusano GL, Walsh TJ. Population pharmacokinetics of micafungin in pediatric patients and implications for antifungal dosing. Antimicrob Agents Chemother 2007a;51:3714-3719. [PubMed]
297. Hope WW, Warn PA, Sharp A, Reed P, Keevil B, Louie A, Walsh TJ, Denning DW, Drusano GL. Optimization of the dosage of flucytosine in combination with amphotericin B for disseminated candidiasis: a pharmacodynamic rationale for reduced dosing. Antimicrob Agents Chemother 2007b;51:3760-3762. [PubMed]
298. Horn R, Wong B, Kiehn TE, Armstrong D. Fungemia in a cancer hospital: changing frequency, earlier onset, and results of therapy. Rev Infect Dis 1985;7:646-655.[PubMed]
299. Horowitz BJ. Topical flucytosine therapy for chronic recurrent Candida tropicalis infections. J Reprod Med 1996;31:821-824. [PubMed]
300. Horowitz BJ, Biaquista D, Ito S. Evolving pathogenesis of vulvovaginal candidiasis: Implications for patient care. J Clin Pharmacol 1992;32:248-255. [PubMed]
301. Horsburgh CR, Kirkpatrick CH. Long-term therapy of chronic mucocutaneous candidiasis with ketoconazole: Experience with twenty-one patients. Am J Med 1983;74:23-29. [PubMed]
302. Horvath LL, George BJ, Hospenthal DR. Detection of fifteen species of Candida in an automated blood culture system. J Clin Microbiol 2007;45:3062-3064. [PubMed]
303. Hsue G, Napier JT, Prince RA, Chi J, Hospenthal DR. Treatment of meningeal coccidioidomycosis with caspofungin. J Antimicrob Chemother 2004;54:292-4. Epub 2004 Jun 09. [PubMed]
304. Huang YC, Lin TY, Leu HS, Peng HL, Wu JH, Chang HY. Outbreak of Candida parapsilosis fungemia in neonatal intensive care units: Clinical implications and genotyping analysis. Infection 1999;27:97-102. [PubMed]
305. Huang YC, Lin TY, Lien RI, Chou YH, Kuo CY, Yang PH, Hsieh WS. Candidaemia in special care nurseries: Comparison of albicans and parapsilosis infection. J Infection 2000a;40:171-175. [PubMed]
306. Huang YC, Lin TY, Lien RI, Chou YH, Kuo CY, Yang PH, Hsieh WS. Fluconazole therapy in neonatal candidemia. Amer J Perinatol 2000b;17:411-415. [PubMed]
307. Hughes JM, Remington JS. Systemic candidiasis: A diagnostic challenge. Calif Med 1972;116:8-17. [PubMed]
308. Hughes WT, Armstrong D, Bodey GP, Bow EJ, Brown AE, Calandra T, Feld R, Pizzo PA, Rolston KVI, Shenep JL, Young LS. 2002 guidelines for the use of antimicrobial agents in neutropenic patients with cancer. Clin Infect Dis 2002;34:730-751. [PubMed]
309. Hurley R, DeLouvois J. Candida vaginitis. Postgrad Med J 1979;55:645-647. [PubMed]
310. Husain S, Tollemar J, Dominguez EA, Baumgarten K, Humar A, Paterson DL, Wagener MM, Kusne S, Singh N. Changes in the spectrum and risk factors for invasive candidiasis in liver transplant recipients: Prospective, multicenter, case-controlled study. Transplantation 2003;75:2023-2029. [PubMed]
311. Hymes SR, Duvic M. Cutaneous candidiasis. In: Body GP, ed. Candidiasis: Pathogenesis, diagnosis, and treatment. New York: Raven Press, Ltd., 1993:159-166. [PubMed]
312. Ibrahim AS, Mirbod F, Filler SG, Banno Y, Cole GT, Kitajima Y, Edwards JE, Jr., Nozawa Y, Ghannoum MA. Evidence implicating phospholipase as a virulence factor of Candida albicans. Infect Immun 1995;63:1993-1998. [PubMed]
313. Imam N, Carpenter CCJ, Mayer KH, Fisher A, Stein M, Danforth SB. Hierarchical pattern of mucosal Candida infections in HIV-seropositive women. Am J Med 1990;89:142-146. [PubMed]
314. Imhof A, Balajee SA, Fredricks DN, Englund JA, Marr KA. Breakthrough fungal infections in stem cell transplant recipients receiving voriconazole. Clin Infect Dis 2004;39:743-6. Epub 2004 Aug 13.[PubMed]
315. Isenmann R, Schwarz M, Rau B, Trautmann M, Schober W, Beger HG. Characteristics of infection with Candida species in patients with necrotizing pancreatitis. World J Surgery 2002;26:372-376.PubMed]
316. Jarrett F, Maki DG, Chan C-K. Management of septic thrombosis of the inferior vena cava caused by Candida. Arch Surg 1978;113:637-639. [PubMed]
317. Jimenez-Exposito MJ, Torres G, Baraldes A, Benito N, Marco F, Pare JC, Moreno A, Claramonte X, Mestres CA, Almela M, Garcia de la Maria C, Perez N, Schell WA, Corey GR, Perfect J, Jimenez de Anta MT, Gatell JM, Miro JM. Native valve endocarditis due to Candida glabrata treated without valvular replacement: a potential role for caspofungin in the induction and maintenance treatment. Clin Infect Dis 2004;39:e70-3. Epub 2004 Sep 08. [PubMed]
318. Jin Y, Endo A, Shimada M, Minato M, Takada M, Takahashi S, Harada K. Congenital systemic candidiasis. Pediatric Infectious Disease Journal 1995;14:818-820.[PubMed]
319. Johnson DC, Johnson FL, Goldman S. Preliminary results treating persistent central venous catheter infections with the antibiotic lock technique in pediatric patients. Pediatr Infect Dis J 1994;13:930-1. [PubMed]
320. Johnson DE, Thompson TR, Ferrieri P. Congenital candidiasis. Am J Dis Child 1981;135:273-275.
321. Johnson MD, MacDougall C, Ostrosky-Zeichner L, Perfect JR, Rex JH. Combination antifungal therapy. Antimicrob Agents Chemother 2004;48:693-715. [PubMed]
322. Johnston P, Lee J, Demanski M, Dressler F, Tucker E, Rothenberg M, Pizzo PA, Walsh TJ. Late recurrent Candida endocarditis. Chest 1991;99:1531-1533. [PubMed]
323. Jokela JA, Kaur P. Caspofungin-resistant oral and esophageal candidiasis in a patient with AIDS. Aids 2007;21:118-119. [PubMed]
324. Joly V, Belmatoug N, Leperre A, Robert J, Jault F, Carbon C, Yeni P. Pacemaker endocarditis due to Candida albicans: Case report and review. Clin Infect Dis 1997;25:1359-1362. [PubMed]
325. Jones JM. Granulomatous hepatitis due to Candida albicans in patients with acute leukemia. Ann Intern Med 1981;94:475-477. [PubMed]
326. Jones JM, Sarsam MA, Clarke MAR, Hedderwick SA. Candida parapsilosis: Two cases of endocarditis in association with the Toronto stentless porcine valve. J Infection 2002;44:196-198. [PubMed]
327. Juster-Reicher A, Flidel-Rimon O, Amitay M, Even-Tov S, Shinwell E, Leibovitz E. High-dose liposomal amphotericin B in the therapy of systemic candidiasis in neonates. Eur J Clin Microbiol Infect Dis 2003;22:603-607. [PubMed]
328. Juster-Reicher A, Leibovitz E, Linder N, Amitay M, Flidel-Rimon O, Even-Tov S, Mogilner B, Barzilai A. Liposomal amphotericin B (AmBisome) in the treatment of neonatal candidiasis in very low birth weight infants. Infection 2000;28:223-226. [PubMed]
329. Kam LA, Giacoia GP. Congenital cutaneous candidiasis. Am J Dis Child 1975;129:1215-1218. [PubMed]
330. Kane JG, Chretien JH, Garagusi VF. Diarrhoea caused by Candida. Lancet 1976;1:335-36. [PubMed]
331. Karlowicz MG. Candidal renal and urinary tract infection in neonates. Semin Perinatol 2003;27:393-400. [PubMed]
332. Karlowicz MG, Hashimoto LN, Kelly RE, Jr., Buescher ES. Should central venous catheters be removed as soon as candidemia is detected in neonates? Pediatrics 2000;106:e63. [PubMed]
333. Karthaus M, Cornely OA, Ullmann AJ. Itraconazole versus fluconazole for antifungal prophylaxis. Ann Intern Med 2004;140:579-580. [PubMed]
334. Kartsonis N, Dinubile M, Bradshaw S, Lipka J, Sable C. Caspofungin for treatment of Candida urinary tract infections: Review of the caspofungin clinical database. 41st Annual Meeting of the Infectious Diseases Society of America. San Diego, 2003, Abstract No. 135. [PubMed]
335. Kartsonis N, DiNubile MJ, Bartizal K, Hicks PS, Ryan D, Sable CA. Efficacy of caspofungin in the treatment of esophageal candidiasis resistant to fluconazole. J Acq Immune Defic Syndrome Hum Retrovirol 2002;31:183-187. [PubMed]
336. Kartsonis NA, Saah A, Lipka CJ, Taylor A, Sable CA. Second-line therapy with caspofungin for mucosal or invasive candidiasis: results from the caspofungin compassionate-use study. J Antimicrob Chemother 2004;53:878-881. [PubMed]
337. Karyotakis NC, Anaissie EJ. Efficacy of escalating doses of liposomal amphotericin B (AmBisome) against hematogenous Candida lusitaniae and Candida krusei infection in neutropenic mice. Antimicrob Agents Chemother 1994;38:2660-2662. [PubMed]
338. Katiyar S, Pfaller M, Edlind T. Candida albicans and Candida glabrata clinical isolates exhibiting reduced echinocandin susceptibility. Antimicrob Agents Chemother 2006;50:2892-2894. [PubMed]
339. Katiyar SK, Edlind TD. Echinocandin resistance associated with sphingolipid pathway mutations and phytospingosine addition. 44th Interscience Conference on Antimicrobial Agents and Chemotherapy. Washington, DC, 2004, Abstract No. M-1771. [PubMed]
340. Katzenstein D. Isolated Candida arthritis: report of a case and definition of a distinct clinical syndrome. Arthritis & Rheumatism 1985;28:1421-4. [PubMed]
341. Kauffman CA, Bradley SF, Ross SC, Weber DR. Hepatosplenic candidiasis: Successful treatment with fluconazole. Am J Med 1991;91:137-141. [PubMed]
342. Kauffman CA, Bradley SF, Vine AK. Candida endophthalmitis associated with intraocular lens implantation: Efficacy of fluconazole therapy. Mycoses 1993;36:13-17.[PubMed]
343. Kauffman CA, Vazquez JA, Sobel JD, Gallis HA, McKinsey DS, Karchmer AW, Sugar AM, Sharkey PK, Wise GJ, Mangi R, Mosher A, Lee JY, Dismukes WE. Prospective multicenter surveillance study of funguria in hospitalized patients. Clin Infect Dis 2000;30:14-18. [PubMed]
344. Kaufman D. Strategies for prevention of neonatal invasive candidiasis. Semin Perinatol 2003;27:414-424. [PubMed]
345. Kaufman D, Boyle R, Hazen KC, Patrie JT, Robinson M, Donowitz LG. Fluconazole prophylaxis against fungal colonization and infection in preterm infants. N Engl J Med 2001;345:1660-1666. [PubMed]
346. Kaufman DA. Prevention of invasive Candida infections in preterm infants: the time is now. Expert Rev Anti-Infect Ther 2008;6:393-399. [PubMed]
347. Kedzierska A, Kochan P, Pietrzyk A, Kedzierska J. Current status of fungal cell wall components in the immunodiagnostics of invasive fungal infections in humans: galactomannan, mannan and (1 -> 3)-beta-D-glucan antigens. Eur J Clin Microbiol Infect Dis 2007;26:755-766. [PubMed]
348. Keiser P, Keay S. Candidal pancreatic abscesses: report of two cases and review. Clin Infect Dis 1992;14:884-888. [PubMed]
349. Kent HL. Epidemiology of vaginitis. Am J Obstet Gynecol 1991;165:1168-1176. [PubMed]
350. Khan FA, Slain D, Khakoo RA. Candida endophthalmitis: Focus on current and future antifungal treatment options. Pharmacotherapy 2007;27:1711-1721. [PubMed]
351. Kim JO, Garofalo L, Blecker-Shelly D, McGowan KL. Candida dubliniensis infections in a pediatric population: Retrospective identification from clinical laboratory isolates of Candida albicans. J Clin Microbiol 2003;41:3354-3357. [PubMed]
352. Kirkpatrick CH. Chronic mucucutaneous candidiasis. Eur J Clin Microbiol Infect Dis 1989;8:448-456. [PubMed]
353. Kirkpatrick CH. Chronic mucocutaneous candidiasis. J Amer Acad Dermatol 1994;31 (Suppl. 2):S14-S17. [PubMed]
354. Kirkpatrick WR, Perea S, Coco BJ, Patterson TF. Efficacy of caspofungin alone and in combination with voriconazole in a guinea pig model of invasive aspergillosis. Antimicrob Agents Chemother 2002;46:2564-2568. [PubMed]
355. Klebanoff SJ, Ozszowski S, van Voorhis WC, Ledbetter JA, Waltersdorph AM, Schlechte KG. Effects of interferon-gamma on human neutrophils: protection from deterioration on storage. Blood 1992;80:225-234. [PubMed]
356. Klein JJ, Watanakunakorn C. Hospital-acquired fungemia: Its natural course and clinical significance. Am J Med 1979;67:51-58. [PubMed]
357. Kleinpeter MA. Successful treatment of Candida infections in peritoneal dialysis patients: case reports and review of the literature. Adv Perit Dial 2004;20:58-61. [PubMed]
358. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: A severity of disease classification system. Crit Care Med 1985;13:818-829. [PubMed]
359. Kojic EM, Darouiche RO. Candida infections of medical devices. Clin Microbiol Rev 2004;17:255-267. [PubMed]
360. Koletar SL, Russell JA, Fass RJ, Plouffe JF. Comparison of oral fluconazole and clotrimazole troches as treatment for oral Candidiasis in patients infected with human immunodeficiency virus. Antimicrob Agents Chemother 1990;34:2267-2268. [PubMed]
361. Komshian SV, Uwaydah AK, Sobel JD, Crane LR. Fungemia caused by Candida species and Torulopsis glabrata in the hospitalized patient: frequency, characteristics, and evaluation of factors influencing outcome. Rev Infect Dis 1989;11:379-390. [PubMed]
362. Korting HC, Schafer-Korting M, Zienicke H, Georgii A, Ollert MW. Treatment of tinea unguium with medium and high doses of ultramicrosize griseofulvin compared with that with itraconazole. Antimicrob Agents Chemother 1993;37:2064-8. [PubMed]
363. Korting HC, Schaller M, Eder G, Hamm G, Bohmer U, Hube B. Effects of the human immunodeficiency virus (HIV) proteinase inhibitors saquinavir and indinavir on in vitro activities of secreted aspartyl proteinases of Candida albicans isolates from HIV-Infected patients. Antimicrob Agents Chemother 1999;43:2038-2042. [PubMed]
364. Krause DS, Reinhardt J, Vazquez JA, Reboli A, Goldstein BP, Wible M, Henkel T. Phase 2, randomized, dose-ranging study evaluating the safety and efficacy of anidulafungin in invasive candidiasis and candidemia. Antimicrob Agents Chemother 2004a;48:2021-2024. [PubMed]
365. Krause DS, Simjee AE, Rensburg C, Viljoen J, Walsh TJ, Goldstein BP, Wible M, Henkel T. A randomized, double-blind trial of anidulafungin versus fluconazole for the treatment of esophageal candidiasis. Clin Infect Dis 2004b;39:770-5. Epub 2004 Aug 27. [PubMed]
366. Krause R, Schwab E, Bachhiesl D, Daxbock F, Wenisch C, Krejs GJ, Reisinger EC. Role of Candida in antibiotic-associated diarrhea. J Infec Dis 2001;184:1065-1069.[PubMed]
367. Krcmery V, Barnes AJ. Non-albicans Candida spp. causing fungaemia: pathogenicity and antifungal resistance. J Hosp Infect 2002;50:243-260. [PubMed]
368. Krishna R, Amuh D, Lowder CY, Gordon SM, Adal KA, Hall G. Should all patients with candidaemia have an ophthalmic examination to rule out ocular candidiasis? Eye 2000;14:30-34. [PubMed]
369. Krogh-Madsen M, Arendrup MC, Heslet L, Knudsen JD. Amphotericin B and caspofungin resistance in Candida glabrata isolates recovered from a critically ill patient. Clin Infect Dis 2006;42:938-944. [PubMed]
370. Krzywda EA, Andris DA, Edmiston CE, Jr., Quebbeman EJ. Treatment of Hickman catheter sepsis using antibiotic lock technique. Infect Control Hosp Epidemiol 1995;16:596-8. [PubMed]
371. Kujath P, Lerch K, Dammrich J. Fluconazole monitoring in Candida peritonitis based on histological control. Mycoses 1990;33:441-448. [PubMed]
372. Kullberg BJ, Pappas P, Ruhnke M, Viscoli C, Cleary JD, Rubinstein E, Church LWP, Brown JM, Rex JH, Hilton F, Oborska I, Hodge M, Schlamm HT, Sobel J. Voriconazole compared with a strategy of amphotericin B followed by fluconazole for treatment of candidaemia in non-neutropenic patients. 14th European Conference of Clinical Microbiology and Infectious Diseases. Prague, Czech Republic, 2004, Abstract No. O245. [PubMed]
373. Kullberg BJ, Sobel JD, Ruhnke M, Pappas PG, Viscoli C, Rex JH, Cleary JD, Rubinstein E, Church LWP, Brown JM, Schlamm HT, Oborska IT, Hilton F, Hodges MR. Voriconazole versus a regimen of amphotericin B followed by fluconazole for candidaemia in non-neutropenic patients: a randomised non-inferiority trial. Lancet 2005;366:1435-1442. [PubMed]
374. Kullberg B-J, Van't wout JW, Hoogstraten C, Van furth R. Recombinant interferon-g enhances resistance to acute disseminated Candida albicans infections in mice. J Infect Dis 1993;168:436-443. [PubMed]
375. Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, Suppes R, Feinstein D, Zanotti S, Taiberg L, Gurka D, Cheang M. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 2006;34:1589-96. [PubMed]
376. Kung N, Fisher N, Gunson B, Hastings M, Mutimer D. Fluconazole prophylaxis for high-risk liver transplant recipients. Lancet 1995;349:1234-1235. [PubMed]
377. Kunová A, Trupl J, Diuholucky S, Galová G, Krcmery V, Jr. Use of fluconazole is not associated with a higher incidence of Candida krusei and other non-albicans Candida species. Clin Infect Dis 1995;21:226-227. [PubMed]
378. Kurtz MB, Rex JH. Glucan synthase inhibitors as antifungal agents. Advances In Protein Chemistry 2001;56:463-475. [PubMed]
379. Kuse ER, Chetchotisakd P, da Cunha CA, Ruhnke M, Barrios C, Raghunadharao D, Sekhon JS, Freire A, Ramasubramanian V, Demeyer I, Nucci M, Leelarasamee A, Jacobs F, Decruyenaere J, Pittet D, Ullmann AJ, Ostrosky-Zeichner L, Lortholary O, Koblinger S, Diekmann-Berndt H, Cornely OA. Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomised double-blind trial. Lancet 2007;369:1519-1527. [PubMed]
380. Kwon-Chung KJ, Bennett JE. Medical Mycology. Philadelphia: Lea & Febiger, 1992. [PubMed]
381. Lafont A, Olive A, Gelman M, Roca-Burniols J, Cots R, Carbonell J. Candida albicans spondylodiscitis and vertebral osteomyelitis in patients with intravenous heroin drug addiction. Report of 3 new cases. J Rheumatol 1994;21:953-956. [PubMed]
382. Lain A, Elguezabal N, Moragues MD, Garcia-Ruiz JC, del Palacio A, Ponon J. Contribution of serum biomarkers to the diagnosis of invasive candidiasis. Expert Rev Mol Diagn 2008;8:315-325. [PubMed]
383. Laine L. The natural history of esophageal candidiasis after successful treatment in patients with AIDS. Gastroenterology 1994;107:744-746. [PubMed]
384. Laine L, Dretler RH, Conteas CN, Tuazon C, Koster FM, Sattler F, Squires K, Islan MZ. Fluconazole compared with ketoconazole for the treatment of Candida esophagitis in AIDS: A randomized trial. Ann Intern Med 1992;117:655-660. [PubMed]
385. Lake DE, Kunzweiler J, Beer M, Buell DN, Islam MZ. Fluconazole versus amphotericin B in the treatment of esophageal candidiasis in cancer patients. Chemotherapy 1996;42:308-314. [PubMed]
386. Landman D, Suarina G, Quale JM. Failure of all antifungal therapy for infection due to Candida albicans: A new AIDS-related problem? Clin Infect Dis 1998;26:183-184.[PubMed]
387. Laverdiere M, Lalonde RG, Baril JG, Sheppard DC, Park S, Perlin DS. Progressive loss of echinocandin activity following prolonged use for treatment of Candida albicans oesophagitis. J Antimicrob Chemother 2006;57:705-708.[PubMed]
388. Law D, Moore CB, Denning DW. Amphotericin B resistance testing of Candida spp.: A comparison of methods. J Antimicrob Chemother 1997;40:109-112. [PubMed]
389. Lazzarini L, Manfrin V, De Lalla F. Candidal prosthetic hip infection in a patient with previous candidal septic arthritis. J Arthroplasty 2004;19:248-52. [PubMed]
390. Leather HL, Wingard JR. Prophylaxis, empirical therapy, or pre-emptive therapy of fungal infections in immunocompromised patients: which is better for whom? Curr Opin Infect Dis 2002;15:369-375. [PubMed]
391. Lecciones JA, Lee JW, Navarro EE, Witebsky FG, Marshall D, Steinberg SM, Pizzo PA, Walsh TJ. Vascular catheter-associated fungemia in patients with cancer: analysis of 155 episodes. Clin Infect Dis 1992;14:875-883. [PubMed]
392. Lee SC, Fung CP, Huang JS, Tsai CJ, Chen KS, Chen HY, Lee N, See LC, Shieh WB. Clinical correlates of antifungal macrodilution susceptibility test results for non-AIDS patients with severe Candida infections treated with fluconazole. Antimicrob Agents Chemother 2000;44:2715-2718. [PubMed]
393. Leen CL, Dunbar EM, Ellis ME, Mandal BK. Once-weekly fluconazole to prevent recurrence of oropharyngeal candidiasis in patients with AIDS and AIDS-related complex: a double-blind placebo-controlled study. J Infect 1990;21:55-60. [PubMed]
394. Lephart P, Ferrieri P, van Burik JA. Reservoir of Candida albicans infection in a vascular bypass graft demonstrates a stable karyotype over six months. Med Mycol 2004;42:255-60. [PubMed]
395. Lerch K, Kalteis T, Schubert T, Lehn N, Grifka J. Prosthetic joint infections with osteomyelitis due to Candida albicans. Mycoses 2003;46:462-466. [PubMed]
396. Leu H-S, Huang C-T. Clearance of funguria with short-course antifungal regimens: A prospective, randomized, controlled study. Clin Infect Dis 1995;20:1152-1157.[PubMed]
397. Levin AS, Costa SF, Mussi NS, Basso M, Sinto SI, Machado C, Geiger DC, Villares MCB, Schreiber AZ, Barone AA, Branchini MLM. Candida parapsilosis fungemia associated with implantable and semi-implantable central venous catheters and the hands of healthcare workers. Diagn Microbiol Infect Dis 1998;30:243-249. [PubMed]
398. Levine J, Bernard DB, Idelson BA, Farnham H, Saunders C, Sugar AM. Fungal peritonitis complicating continuous ambulatory peritoneal dialysis: Successful treatment with fluconazole, a new orally active antifungal agent. Am J Med 1989;86:825-829. [PubMed]
399. Levine J, Dykoski RK, Janoff EN. Candida-associated diarrhea: a syndrome in search of credibility. Clin Infect Dis 1995;21:881-886. [PubMed]
400. Lewis JH, Zimmerman HJ, Benton GD, Ishak KG. Hepatic injury associated with ketoconazole therapy: Analysis of 33 cases. Gastroenterology 1984;86:503-513.[PubMed]
401. Lewis RE. What is the "Therapeutic Range" for voriconazole? Clin Infect Dis 2008;46:212-214. [PubMed]
402. Lin D, Wu L-C, Rinaldi MG, Lehmann PF. Three distinct genotypes with Candida parapsilosis from clinical sources. J Clin Microbiol 1995;33:1815-1821. [PubMed]
403. Linden P, Kramer DJ, Mazariegos G, Marsh W, Casavilla A, Pinna A, Fung J, Kusen S. Low-dose amphotericin B for the prophylaxis of serious Candida infections in high-risk liver recipients. 36th Interscience Conference on Antimicrobial Agents and Chemotherapy. New Orleans, 1996, Abstract No. J47. [PubMed]
404. Linder N, Klinger G, Shalit I, Levy I, Ashkenazi S, Haski G, Levit O, Sirota L. Treatment of candidaemia in premature infants: comparison of three amphotericin B preparations. J Antimicrob Chemother 2003;52:663-667. [PubMed]
405. Lindner A, Becker G, Warmuth-Metz M, Schalke BCG, Bogdahn U, Tyoka KV. Magnetic resonance image findings of spinal intramedullary abscess caused by Candida albicans: Case report. Neurosurgery 1995;36:411-412. [PubMed]
406. Lipton SA, Hickey WF, Morris JH, Loscalzo J. Candidal infection in the central nervous system. Am J Med 1984;76:101-108. [PubMed]
407. Liu KH, Wu CJ, Chou CH, Lee HC, Lee NY, Hung ST, Ko WC. Refractory candidal meningitis in an immunocompromised patient cured by caspofungin. J Clin Microbiol 2004;42:5950-3. [PubMed]
408. Lott TJ, Kuykendall RJ, Reiss E. Nucleotide sequence analysis of the 5.8S rDNA and adjacent ITS2 region of Candida albicans and related species. Yeast 1993;9:1199-206.[PubMed]
409. Lunardi LW, Aquino VR, Zimerman RA, Goldani LZ. Epidemiology and outcome of Rhodotorula fungemia in a tertiary care hospital. Clin Infect Dis 2006;43:E60-E63.[PubMed]
410. Lundstrom T, Sobel J. Nosocomial candiduria: A review. Clin Infect Dis 2001;32:1602-1607. [PubMed]
411. Lupetti A, Tavanti A, Davini P, Ghelardi E, Corsini V, Merusi I, Boldrini A, Campa M, Senesi S. Horizontal transmission of Candida parapsilosis candidemia in a neonatal intensive care unit. J Clin Microbiol 2002;40:2363-2369. [PubMed]
412. Lutsar I, Roffey S, Troke P. Voriconazole concentrations in the cerebrospinal fluid and brain tissue of guinea pigs and immunocompromised patients. Clin Infect Dis 2003;37:728-732. [PubMed]
413. Luzzati R, Amalfitano G, Lazzarini L, Soldani F, Bellino S, Solbiati M, Danzi MC, Vento S, Todeschini G, Vivenza C, Concia E. Nosocomial candidemia in non-neutropenic patients at an Italian tertiary care hospital. Eur J Clin Microbiol Infect Dis 2000;19:602-607. [PubMed]
414. Lye DCB, Hughes A, O'Brien D, Athan E. Candida glabrata prosthetic valve endocarditis treated successfully with fluconazole plus caspofungin without surgery: a case report and literature review. Eur J Clin Microbiol Infect Dis 2005;24:753-755. [PubMed]
415. Maertens J, Deeren D, Dierickx D, Theunissen K. Preemptive antifungal therapy: still a way to go. Curr Opin Infect Dis 2006a;19:551-556. [PubMed]
416 Maertens J, Glasmacher A, Herbrecht R, Thiebaut A, Cordonnier C, Segal BH, Killar J, Taylor A, Kartsonis N, Patterson TF. Multicenter, noncomparative study of caspofungin in combination with other antifungals as salvage therapy in adults with invasive aspergillosis. Cancer 2006b;107:2888-2897. [PubMed]
417. Maertens J, Theunissen K, Deeren D, Meersseman W, Van Eldere J. Defining a case of invasive aspergillosis by serum galactomannan. Med Mycol 2006c;44:S173-S178.[PubMed]
418. Magill SS, Shields C, Sears CL, Choti M, Merz WG. Triazole cross-resistance among Candida spp.: Case report, occurrence among bloodstream isolates, and implications for antifungal therapy. J Clin Microbiol 2006;44:529-535. [PubMed]
419. Magnussen CR, Olson JP, Ona FV, Graziani AJ. Candida fungus balls in the common bile duct. Unusual manifestation of disseminated candidiasis. Arch Intern Med 1979;139:821-2. [PubMed]
420. Malani A, Hmoud J, Chiu L, Carver PL, Bielaczyc A, Kauffman CA. Candida glabrata fungemia: Experience in a tertiary care center. Clin Infect Dis 2005;41:975-981.[PubMed]
421. Malani AN, Kauffman CA. Candida urinary tract infections: treatment options. Expert Rev Anti-Infect Ther 2007;5:277-284. [PubMed]
422. Malani PN, McNeil SA, Bradley SF, Kauffman CA. Candida albicans sternal wound infections: A chronic and recurrent complication of median sternotomy. Clin Infect Dis 2002;35:1316-1320. [PubMed]
423. Malik IA, Moid I, Aziz Z, Khan S, Suleman M. A randomized comparison of fluconazole with amphotericin B as empiric anti-fungal agents in cancer patients with prolonged fever and neutropenia. Amer J Med 1998;105:478-483. [PubMed]
424. Manzoni P, Arisio R, Mostert M, Leonessa M, Farina D, Latino MA, Gomirato G. Prophylactic fluconazole is effective in preventing fungal colonization and fungal systemic infections in preterm neonates: A single-center, 6-year, retrospective cohort study. Pediatrics 2006a;117:E22-E32. [PubMed]
425. Manzoni P, Leonessa ML, Monetti C, Farina D, Gomirato G. Prevention strategies in patients at high-risk for Candida infections: data from a neonatal intensive care setting. Intens Care Med 2006b;32:936. [PubMed]
426. Manzoni P, Stolfi I, Pugni L, Decembrino L, Magnani C, Vetrano G, Tridapalli E, Corona G, Giovannozzi C, Farina D, Arisio R, Merletti F, Maule M, Mosca F, Pedicino R, Stronati M, Mostert M, Gomirato G. A multicenter, randomized trial of prophylactic fluconazole in preterm neonates. N Engl J Med 2007;356:2483-2495. [PubMed]
427. Marr B, Gross S, Cunningham C, Weiner L. Candidal sepsis and meningitis in a very-low-birth-weight infant successfully treated with fluconazole and flucytosine. Clin Infect Dis 1994;19:795-796. [PubMed]
428. Marr KA, Boeckh M, Carter RA, Kim HW, Corey L. Combination antifungal therapy for invasive aspergillosis. Clin Infect Dis 2004;39:797-802. [PubMed]
429. Marr KA, White TC, van Burik JAH, Bowden RA. Development of fluconazole resistance in Candida albicans causing disseminated infection in a patient undergoing marrow transplantation. Clin Infect Dis 1997;25:908-910. [PubMed]
430. Marra F, Robbins GM, Masri BA, Duncan C, Wasan KM, Kwong EH, Jewesson PJ. Amphotericin B-loaded bone cement to treat osteomyelitis caused by Candida albicans. Can J Surg 2001;44:383-386.[PubMed]
431. Marriott DJ, Jones PD, Hoy JF, Speed BR, Harkness JL. Fluconazole once a week as secondary prophylaxis against oropharyngeal candidiasis in HIV-infected patients. Med J Aust 1993;158:312-316. [PubMed]
432. Martinez-Suarez JV, Rodriguez-Tudela JL. Patterns of in vitro activity of itraconazole and imidazole antifungal agents against Candida albicans with decreased susceptibility to fluconazole from Spain. Antimicrob Agents Chemother 1995;39:1512-1516. [PubMed]
433. Martinez-Vasquez C, Fernandez-Ulloa J, Bordon J, Sopena B, de la Fuente J, Ocampo A, Rubianes M. Candida albicans endophthalmitis in brown heroin addicts: Response to early vitrectomy preceded and followed by antifungal therapy. Clin Infect Dis 1998;27:1130-1133. [PubMed]
434. Martino P, Girmenia C, Micozzi A, Raccah R, Gentile G, Venditto M, Mandelli F. Fungemia in patients with leukemia. Am J Med Sci 1993;306:225-232. [PubMed]
435. Martins MD, Lozano-Chiu M, Rex JH. Declining rates of oropharyngeal candidiasis and carriage of Candida albicans associated with trends toward reduced rates of carriage of fluconazole-resistant C. albicans in human immunodeficiency virus-infected patients. Clin Infect Dis 1998;27:1291-1294. [PubMed]
436. Martins MD, Rex JH. Fluconazole suspension for oropharyngeal candidiasis unresponsive to tablets. Ann Intern Med 1997;126:332-333. [PubMed]
437. Mascarenas CA, Hardin TC, Pennick GJ, Rinaldi MG, Graybill JR. Treatment of thrush with itraconazole solution: Evidence for topical effect. Clin Infect Dis 1998;26:1242-1243. [PubMed]
438. Masur H, Rosen PP, Armstrong D. Pulmonary disease caused by Candida species. Am J Med 1977;63:914-925. [PubMed]
439. Matthieu L, De Doncker P, Cauwenbergh G, Woestenborghs R, van de Velde V, Janssen PA, Dockx P. Itraconazole penetrates the nail via the nail matrix and the nail bed--an investigation in onychomycosis. Clinical & Experimental Dermatology 1991;16:374-376. [PubMed]
440. Mayayo E, Moralejo J, Camps J, Guarro J. Fungal endocarditis in premature infants: Case report and review. Clin Infect Dis 1996;22:366-368. [PubMed]
441. Mayer P, Schutze E, Lam C, Kricek F, Liehl E. Recombinant murine granulocyte-macrophage colony-stimulating factor augments neutrophil recovery and enhances resistance to infections in myelosuppressed mice. J Infect Dis 1991;163:584-90. [PubMed]
442. McCormack PL, Perry CM. Caspofungin: a review of its use in the treatment of fungal infections. Drugs 2005;65:2049-68. [PubMed]
443. McCullers JA, Vargas SL, Flynn PM, Razzouk BI, Shenep JL. Candidal meningitis in children with cancer. Clin Infect Dis 2000;31:451-457. [PubMed]
444. McGinnis MR, Rinaldi MG. Selected medically important fungi and some common synonyms and obsolete names. Clin Infect Dis 1995;21:277-278. [PubMed]
445. McKinsey DS, Wheat LJ, Cloud GA, Pierce M, Black JR, Bamberger DM, Goldman M, Thomas CJ, Gutsch HM, Moskovitz B, Dismukes WE, Kauffman CA. Itraconazole prophylaxis for fungal infections in patients with advanced human immunodeficiency virus infection: Randomized, placebo-controlled, double-blind study. Clin Infect Dis 1999;28:1049-1056. [PubMed]
446. McMullan R, Metwally L, Coyle PV, Hedderwick S, McCloskey B, O'Neill HJ, Patterson CC, Thompson G, Webb CH, Hay RJ. A prospective clinical trial of a real-time polymerase chain reaction assay for the diagnosis of candidemia in nonneutropenic, critically ill adults. Clin Infect Dis 2008;46:890-896. [PubMed]
447. McNeil MM, Nash SL, Hajjeh RA, Phelan MA, Conn LA, Plikaytis BD, Warnock DW. Trends in mortality due to invasive mycotic diseases in the United States, 1980-1997. Clin Infect Dis 2001;33:641-647. [PubMed]
448. Meiller TF, Kelley JI, Jabra-Rizk MA, DePaola LG, Baqui A, Falkler WA, Jr. In vitro studies of the efficacy of antimicrobials against fungi. Oral Surg Oral Med Oral Patho 2001;91:663-670. [PubMed]
449. Melamed R, Leibovitz E, Abramson O, Levitas A, Zucker N, Gorodisher R. Successful non-surgical treatment of Candida tropicalis endocarditis with liposomal amphotericin-B (AmBisome). Scand J Infec Dis 2000;32:86-89.[PubMed]
450. Merlin E, Galambrun C, Ribaud P, Blanc T, Michel G, Auvrignon A, Stephan JL. Efficacy and safety of caspofungin therapy in children with invasive fungal infections. Pediat Inf Dis J 2006;25:1186-1188. [PubMed]
451. Mermel LA, Farr BM, Sherertz RJ, Raad, II, O'Grady N, Harris JS, Craven DE. Guidelines for the management of intravascular catheter-related infections. Clin Infect Dis 2001;32:1249-1272. [PubMed]
452. Merrer J, Dupont B, Nieszkowska A, De Jonghe B, Outin H. Candida albicans prosthetic arthritis treated with fluconazole alone. J Infection 2001;42:208-209. [PubMed]
453. Merz WG. Candida lusitaniae: frequency of recovery, colonization, infection, and amphotericin B resistance. J Clin Microbiol 1984;20:1194-1195. [PubMed]
454. Merz WG, Karp JE, Schron D, Saral R. Increased incidence of fungemia caused by Candida krusei. J Clin Microbiol 1986;24:581-584. [PubMed]
455. Merz WG, Sanford GR. Isolation and characterization of a polyene-resistant variant of Candida tropicalis. J Clin Microbiol 1979;9:677-680. [PubMed]
456. Meunier F. Management of candidemia. N Engl J Med 1994;331:1371-1372. [PubMed]
457. Meunier F, Aoun M, Gerard M. Therapy for oropharyngeal candidiasis in the immunocompromised host: A randomized double-blind study of fluconazole vs. ketoconazole. Rev Infect Dis 1990;12 (Suppl. 3):S364-S368. [PubMed]
458. Meunier-Carpentier F, Kiehn TE, Armstrong D. Fungemia in the immunocompromised host: changing patterns, antigenemia, high mortality. Am J Med 1981;71:363-370. [PubMed]
459. Miceli MH, Jackson LBJ, Walker RC, Talamo G, Barlogie B, Anaissie EJ. Diagnosis of infection of implantable central venous catheters by [F-18]fluorodeoxyglucose positron emission tomography. Nucl Med Commun 2004;25:813-818. [PubMed]
460. Michalopoulos AS, Geroulanos S, Mentzelopoulos SD. Determinants of candidemia and candidemia-related death in cardiothoracic ICU patients. Chest 2003;124:2244-2255. [PubMed]
461. Michel C, Courdavault L, al Khayat R, Viron B, Roux P, Mignon F. Fungal peritonitis in patients on peritoneal dialysis. American Journal of Nephrology 1994;14:113-20.[PubMed]
462. Miller DJ, Mejicano GC. Vertebral osteomyelitis due to Candida species: Case report and literature review. Clin Infect Dis 2001;33:523-530. [PubMed]
463. Minari A, Hachem R, Raad I. Candida lusitaniae: A cause of breakthrough fungemia in cancer patients. Clin Infect Dis 2001;32:186-190. [PubMed]
464. Mohr JF, Finkel KW, Rex JH, Rodriguez JR, Leitz GJ, Ostrosky-Zeichner L. Pharmacokinetics of intravenous itraconazole in stable hemodialysis patients. Antimicrob Agents Chemother 2004;48:3151-3. [PubMed]
465. Mohr JF, Hall AC, Ericsson CD, Ostrosky-Zeichner L. Fatal amphotericin B overdose due to administration of nonlipid formulation instead of lipid formulation. Pharmacotherapy 2005;25:426-428. [PubMed]
466. Montenegro J, Aguirre R, Gonzalez O, Martinze I, Saracho R. Fluconazole treatment of Candida peritonitis with delayed removal of the peritoneal dialysis catheter. Clin Nephrol 1995;44:60-63. [PubMed]
467. Montoya JG, Rosso F. Is combination therapy indicated for invasive fungal infections? Yes and no. Curr Opin Infect Dis 2006;19:357-359. [PubMed]
468. Montravers P, Gauzit R, Muller C, Marmuse JP, Fichelle A, Desmonts JM. Emergence of antibiotic-resistant bacteria in cases of peritonitis after intraabdominal surgery affects the efficacy of empirical antimicrobial therapy. Clin Infect Dis 1996;23:486-94. [PubMed]
469. Mora-Duarte J, Betts R, Rotstein R, Lopes-Colombo A, Thompson-Moya L, Smietana J, Lupinacci R, Sable C, Kartsonis N, Perfect J, Caspofungin Invasive Candidiasis Study Group. Comparison of caspofungin and amphotericin B for invasive candidiasis. N Engl J Med 2002;347:2020-9. [PubMed]
470. Moran GP, Sullivan DJ, Henman MC, McCreary CE, Harrington BJ, Shanley DB, Coleman DC. Antifungal drug susceptibilities of oral Candida dublinensis isolates from human immunodeficiency virus (HIV)-infected and non-HIV-infected subjects and generation of stable fluconazole-resistant derivatives in vitro. Antimicrob Agents Chemother 1997;41:617-623. [PubMed]
471. Morgenstern GR, Prentice AG, Prentice HG, Ropner JE, Schey SA, Warnock DW, U.K. Multicentre Antifungal Prophylaxis Study Group. A randomised controlled trial of itraconazole versus fluconazole for the prevention of fungal infections in patients with haematological malignancies. Br J Haematol 1999;105:901-911. [PubMed]
472. Mori T, Matsumura M, Kanamaru Y, Miyano S, Hishikawa T, Irie S, Oshimi K, Saikawa T, Oguri T. Myelofibrosis complicated by infection due to Candida albicans: Emergence of resistance to antifungal agents during therapy. Clin Infect Dis 1997;25:1470-1471. [PubMed]
473. Morrell M, Fraser VJ, Kollef MH. Delaying the empiric treatment of Candida bloodstream infection until positive blood culture results are obtained: a potential risk factor for hospital mortality. Antimicrob Agents Chemother 2005;49:3640-3645. [PubMed]
474. Morrison VA. Caspofungin: an overview. Expert Rev Anti Infect Ther 2005;3:697-705. [PubMed]
475. Mossad SB. Itraconazole versus fluconazole for antifungal prophylaxis. Ann Intern Med 2004;140:580-581. [PubMed]
476. Moudgal V, Little T, Boikov D, Vazquez JA. Multiechinocandin- and multiazole-resistant Candida parapsilosis isolates serially obtained during therapy for prosthetic valve endocarditis. Antimicrob Agents Chemother 2005;49:767-769. [PubMed]
477. Moudgal VV, Sobel JD. Antifungal drugs in pregnancy: a review. Expert Opin Drug Saf 2003;2:475-83. [PubMed]
478. Moudgal VV, Sobel JD. Selecting antifungal agents for the treatment of invasive fungal infections in patients with renal failure. Curr Opin Investig Drugs 2004;5:873-8.[PubMed]
479. Moylett EH. Neonatal Candida meningitis. Semin Pediatr Infect Dis 2003;14:115-22. [PubMed]
480. Mrowczynski W, Wojtalik M. Caspofungin for Candida endocarditis. Pediat Inf Dis J 2004;23:376. [PubMed]
481. Muehrcke DD, Lytle BW, Cosgrove DM, 3rd. Surgical and long-term antifungal therapy for fungal prosthetic valve endocarditis. Annals of Thoracic Surgery 1995;60:538-43. [PubMed]
482. Muhl E, Martens T, Iven H, Rob P, Bruch HP. Influence of continuous veno-venous haemodiafiltration and continuous veno-venous haemofiltration on the pharmacokinetics of fluconazole. Eur J Clin Pharmacol 2000;56:671-678. [PubMed]
483. Munoz P, Singh N, Bouza E. Treatment of solid organ transplant patients with invasive fungal infections: should a combination of antifungal drugs be used? Curr Opin Infect Dis 2006;19:365-370. [PubMed]
484. Nagappan V, Deresinski S. Posaconazole: A broad-spectrum triazole antifungal agent. Clin Infect Dis 2007a;45:1610-1617. [PubMed]
485. Nagappan V, Deresinski S. Reviews of anti-infective agents: Posaconazole: a broad-spectrum triazole antifungal agent. Clin Infect Dis 2007b;45:1610-7. [PubMed]
486. Narendran N, Balasubramaniam B, Johnson E, Dick A, Mayer E. Five-year retrospective review of guideline-based management of fungal endophthalmitis. Acta Ophthalmol 2008;86:525-532.[PubMed]
487. Natarajan G, Lulic-Botica ML, Pappas A, Rongkavilit C, Bedard MP. Experience with caspofungin in the treatment of fungal infections in neonates. Pediat Res 2004;55:394A-395A. [PubMed]
488. National Committee for Clinical Laboratory Standards. Reference method for broth dilution antifungal susceptibility testing of yeasts; tentative standard. NCCLS document M27-T. Wayne, Pa: National Committee for Clinical Laboratory Standards, 1995. [PubMed]
489. National Committee for Clinical Laboratory Standards. Reference method for broth dilution antifungal susceptibility testing of yeasts; Approved standard NCCLS document M27-A. Wayne, Pa: National Committee for Clinical Laboratory Standards, 1997. [PubMed]
490. National Committee for Clinical Laboratory Standards. Methods for antifungal disk diffusion susceptibility testing of yeasts; Approved Guideline M44-A. Wayne, Pa: National Committee for Clinical Laboratory Standards, 2004. [PubMed]
491. Navarro D, Monzonis E, Lopez-Ribot JL, Sepulveda P, Casanova M, Nogueira JM, Martinez JP. Diagnosis of systemic candidiasis by enzyme immunoassay detection of specific antibodies to mycelial phase cell wall and cytoplasmic candidal antigens. Eur J Clin Microbiol Infect Dis 1993;12:839-846. [PubMed]
492. Navarro EE, Almario JS, Schaufele RL, Bacher J, Walsh TJ. Quantitative urine cultures do not reliably detect renal candidiasis in rabbits. J Clin Microbiol 1997;35:3292-3297. [PubMed]
493. Ng TT, Denning DW. Liposomal amphotericin B (AmBisome) therapy in invasive fungal infections. Evaluation of United Kingdom compassionate use data. Arch Intern Med 1995;155:1093-1098. [PubMed]
494. Nguyen MH, Clancy CJ, Yu VL, Yu YV, Morris AJ, Snydman DR, Sutton DA, Rinaldi MG. Do in vitro susceptibility data predict the microbiologic response to amphotericin B? Results of a prospective study of patients with Candida fungemia. J Infect Dis 1998;177:425-430. [PubMed]
495. Nguyen MH, Nguyen ML, Yu VL, McMahon D, Keys TF, Amidi M. Candida prosthetic valve endocarditis: Prospective study of six cases and review of the literature. Clin Infect Dis 1996a;22:262-267. [PubMed]
496. Nguyen MH, Peacock JE, Jr., Morris AJ, Tanner DC, Nguyen ML, Snydman DR, Wagener MM, Rinaldi MG, Yu VL. The changing face of candidemia: Emergence of non-C. albicans species and antifungal resistance. Am J Med 1996b;100:617-623. [PubMed]
497. Nguyen MH, Peacock JE, Jr., Tanner DC, Morris AJ, Nguyen ML, Snydman DR, Wagener MM, Yu VL. Therapeutic approaches in patients with candidemia. Evaluation in a multicenter, prospective, observational study. Arch Intern Med 1995a;155:2429-2435. [PubMed]
498. Nguyen MH, Yu VL. Meningitis caused by Candida species: an emerging problem in neurosurgical patients. Clin Infect Dis 1995b;21:323-327. [PubMed]
499. Nguyen MH, Yu VL, Morris AJ. Candida infection of the arteriovenous fistula used for hemodialysis. Am J Kidney Dis 1996c;27:596-598. [PubMed]
500. Nieto-Rodriguez JA, Kusne S, Manez R, Irish W, Linden P, Magnone M, Wing EJ, Fung JJ, Starzl TE. Factors associated with the development of candidemia and candidemia-related death among liver transplant recipients. Ann Surg 1996;223:70-76. [PubMed]
501. Nucci M, Anaissie E. Revisiting the source of candidemia: Skin or gut? Clin Infect Dis 2001;33:1959-1967. [PubMed]
502. Nucci M, Anaissie E. Should vascular catheters be removed from all patients with candidemia? An evidence-based review. Clin Infect Dis 2002;34:591-599. [PubMed]
503. Obayashi T, Yoshida M, Mori T, Goto H, Yasuoka A, Iwasaki H, Teshima H, Kohno S, Horiuchi A, Ito A, Yamaguchi H, Shimada K, Kawai T. Plasma (1->3)-beta-D-glucan measurement in diagnosis of invasive deep mycosis and fungal febrile episodes. Lancet 1995;345:17-20. [PubMed]
504. Odabasi Z, Mattiuzzi G, Estey E, Kantarjian H, Saeki F, Ridge RJ, Ketchum PA, Finkelman MA, Rex JH, Ostrosky-Zeichner L. Beta-D-glucan as a diagnostic adjunct for invasive fungal infections: Validation, cutoff development, and performance in patients with acute myelogenous leukemia and myelodysplastic syndrome. Clin Infect Dis 2004;39:199-205. [PubMed]
505. Odabasi Z, Mattiuzzi G, Ostrosky-Zeichner L, Estey E, Kantarjian H, Rex JH. Detection of (1->3)-beta-D-Glucan in the serum of leukemia patients with invasive fungal infections. 42nd Interscience Conference on Antimicrobial Agents and Chemotherapy, 2002, Abstract No. M-902. [PubMed]
506. O'Day DM, Foulds G, Williams TE, Robinson RD, Allen RH, Head WS. Ocular uptake of fluconazole following oral administration. Arch Ophthalmol 1990;108:1006-8.[PubMed]
507. O'Day DM, Head WS, Robinson RD, Stern WH, Freeman JM. Intraocular penetration of systemically administered antifungal agents. Current Eye Research 1985;4:131-134. [PubMed]
508. Odds FC. Fluconazole plus amphotericin B combinations are not contraindicated and may add benefit for the treatment of candidemia. Clin Infect Dis 2003;36:1229-1231.[PubMed]
509. Odds FC, Motyl M, Andrade R, Bille J, Canton E, Cuenca-Estrella M, Davidson A, Durussel C, Ellis D, Foraker E, Fothergill AW, Ghannoum MA, Giacobbe RA, Gobernado M, Handke R, Laverdiere M, Lee-Yang W, Merz WG, Ostrosky-Zeichner L, Peman J, Perea S, Perfect JR, Pfaller MA, Proia L, Rex JH, Rinaldi MG, Rodriguez-Tudela JL, Schell WA, Shields C, Sutton DA, Verweij PE, Warnock DW. Interlaboratory comparison of results of susceptibility testing with caspofungin against Candida and Aspergillus species. J Clin Microbiol 2004;42:3475-82. [PubMed]
510. Odds FC, Van Nuffel L, Dams G. Prevalence of Candida dubliniensis isolates in a yeast stock collection. J Clin Microbiol 1998;36:2869-2873. [PubMed]
511. Odio CM, Araya R, Pinto LE, Castro CE, Vasquez S, Alfaro B, Saenz A, Herrera ML, Walsh TJ. Caspofungin therapy of neonates with invasive candidiasis. Pediatr Infect Dis J 2004;23:1093-7. [PubMed]
512. Oleinik EM, Della-Latta P, Rinaldi MG, Saiman L. Candida lusitaniae osteomyelitis in a premature infant. American Journal of Perinatology 1993;10:313-5. [PubMed]
513. Oliveira K, Haase G, Kurtzman C, Hyldig-Nielsen JJ, Stender H. Differentiation of Candida albicans and Candida dubliniensis by fluorescent in situ hybridization with peptide nucleic acid probes. J Clin Microbiol 2001;39:4138-4141.[PubMed]
514. O'Meeghan T, Varcoe R, Thomas M, Ellis-Pegler R. Fluconazole concentration in joint fluid during successful treatment of Candida albicans septic arthritis [letter]. J Antimicrob Chemother 1990;26:601-602. [PubMed]
515. Ostrosky-Zeichner L, Alexander BD, Kett DH, Vazquez J, Pappas PG, Saeki F, Ketchum PA, Wingard J, Schiff R, Tamura H, Finkelman MA, Rex JH. Multicenter clinical evaluation of the (1 -> 3) beta-D-glucan assay as an aid to diagnosis of fungal infections in humans. Clin Infect Dis 2005;41:654-659. [PubMed]
516. Ostrosky-Zeichner L, Kontoyiannis D, Raffalli J, Mullane KM, Vazquez J, Anaissie EJ, Lipton J, Jacobs P, van Rensburg JHJ, Rex JH, Lau W, Facklam D, Buell DN. International, open-label, noncomparative, clinical trial of micafungin alone and in combination for treatment of newly diagnosed and refractory candidemia (vol 24, pg 654, 2005). Eur J Clin Microbiol Infect Dis 2006a;25:69. [PubMed]
517. Ostrosky-Zeichner L, Lashof A, Kullberg BJ, Rex JH. Voriconazole salvage treatment of invasive candidiasis. Eur J Clin Microbiol Infect Dis 2003a;22:651-655. [PubMed]
518. Ostrosky-Zeichner L, Marr KA, Rex JH, Cohen SH. Amphotericin B: Time for a new "gold standard". Clin Infect Dis 2003b;37:415-425. [PubMed]
519. Ostrosky-Zeichner L, Pappas PG. Invasive candidiasis in the intensive care unit. Crit Care Med 2006b;34:857-863. [PubMed]
520. Ostrosky-Zeichner L, Rex JH, Pappas PG, Hamill RJ, Larsen RA, Horowitz HW, Powderly WG, Hyslop N, Kauffman CA, Cleary J, Mangino JE, Lee J. Antifungal susceptibility survey of 2,000 bloodstream Candida isolates in the United States. Antimicrob Agents Chemother 2003c;47:3149-3154. [PubMed]
521. Ostrosky-Zeichner L, Sable C, Sobel J, Alexander BD, Donowitz G, Kan V, Kauffman CA, Kett D, Larsen RA, Morrison V, Nucci M, Pappas PG, Bradley ME, Major S, Zimmer L, Wallace D, Dismukes WE, Rex JH. Multicenter retrospective development and validation of a clinical prediction rule for nosocomial invasive candidiasis in the intensive care setting. Eur J Clin Microbiol Infect Dis 2007;26:271-276. [PubMed]
522. Oude Lashof AML, De Bock R, Herbrecht R, de Pauw BE, Krcmery V, Aoun M, Akova M, Cohen J, Siffnerova H, Egyed M, Ellis M, Marinus A, Sylvester R, Kullberg BJ. An open multicentre comparative study of the efficacy, safety and tolerance of fluconazole and itraconazole in the treatment of cancer patients with oropharyngeal candidiasis. Eur J Cancer 2004;40:1314-1319. [PubMed]
523. Pachl J, Svoboda P, Jacobs F, Vandewoude K, van der Hoven B, Spronk P, Masterson G, Malbrain M, Aoun M, Garbino J, Takala J, Drgona L, Burnie J, Matthews R. A randomized, blinded, multicenter trial of lipid-associated amphotericin B alone versus in combination with an antibody- based inhibitor of heat shock protein 90 in patients with invasive candidiasis. Clin Infect Dis 2006;42:1404-1413. [PubMed]
524. Paderu P, Garcia-Effron G, Balashov S, Delmas G, Park S, Perlin DS. Serum differentially alters the antifungal properties of echinocandin drugs. Antimicrob Agents Chemother 2007;51:2253-2256. [PubMed]
525. Pai MP, Turpin RS, Garey KW. Association of fluconazole area under the concentration-time curve/MIC and dose/MIC ratios with mortality in nonneutropenic patients with candidemia. Antimicrob Agents Chemother 2007;51:35-39. [PubMed]
526. Panackal AA, Gribskov JL, Staab JF, Kirby KA, Rinaldi M, Marr KA. Clinical significance of azole antifungal drug cross-resistance in Candida glabrata. J Clin Microbiol 2006;44:1740-1743. [PubMed]
527. Pannaraj PS, Walsh TJ, Baker CJ. Advances in antifungal therapy. Pediatr Infect Dis J 2005;24:921-2. [PubMed]
528. Papanicolaou GA, Meyers BR, Fuchs WS, Guillory SL, Mendelson MH, Sheiner P, Emre S, Miller C. Infectious ocular complications in orthotopic liver transplant patients. Clin Infect Dis 1997;24:1172-1177. [PubMed]
529. Paphitou NI, Ostrosky-Zeichner L, Rex JH. Rules for identifying patients at increased risk for candidal infections in the surgical intensive care unit: approach to developing practical criteria for systematic use in antifungal prophylaxis trials. Med Mycol 2005;43:235-243. [PubMed]
530. Pappagianis D, Collins MS, Hector R, Remington J. Development of reistance to amphotericin B in Candida lusitaniae infecting a human. Antimicrob Agents Chemother 1979;16:123-126. [PubMed]
531. Pappas PG, Rex JH, Lee J, Hamill RJ, Larsen RA, Powderly W, Kauffman CA, Hyslop N, Mangino JE, Chapman S, Horowitz HW, Edwards JE, Dismukes WE. A prospective observational study of candidemia: Epidemiology, therapy, and influences on mortality in hospitalized adult and pediatric patients. Clin Infect Dis 2003;37:634-643.[PubMed]
532. Pappas PG, Rex JH, Sobel JD, Filler SG, Dismukes WE, Walsh TJ, Edwards JE. Guidelines for treatment of candidiasis. Clin Infect Dis 2004;38:161-189. [PubMed]
533. Pappas PG, Rotstein CMF, Betts RF, Nucci M, Talwar D, De Waele JJ, Vazquez JA, Dupont BF, Horn DL, Ostrosky-Zeichner L, Reboli AC, Suh B, Digumarti R, Wu C, Kovanda LL, Arnold LJ, Buell DN. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis 2007;45:883-893.[PubMed]
534. Park BJ, Arthington-Skaggs BA, Sofair A, Harrison LH, Phelan DM, Hajjeh RA, Warnock DW. Lack of correlation of amphotericin B MICs with clinical outcome in Candida bloodstream infections. 41st Annual Meeting of the Infectious Diseases Society of America. San Diego, 2003, Abstract No. 134. [PubMed]
535. Park S, Kelly R, Kahn JN, Robles J, Hsu MJ, Register E, Li W, Vyas V, Fan H, Abruzzo G, Flattery A, Gill C, Chrebet G, Parent SA, Kurtz M, Teppler H, Douglas CM, Perlin DS. Specific substitutions in the echinocandin target Fks1p account for reduced susceptibility of rare laboratory and clinical Candida sp. isolates. Antimicrob Agents Chemother 2005;49:3264-73. [PubMed]
536. Parker JC, McCloskey JJ, Lee RS. The emergence of candidosis: The dominant postmortem cerebral mycosis. Am J Clin Path 1978;70:31-36. [PubMed]
537. Pascual A, Calandra T, Bolay S, Buclin T, Bille J, Marchetti O. Voriconazole therapeutic drug monitoring in patients with invasive mycoses improves efficacy and safety outcomes. Clin Infect Dis 2008;46:201-211. [PubMed]
538. Pasqualotto AC, Shah M, Wynn R, Denning DW. Voriconazole plasma monitoring. Arch Dis Child 2008. [PubMed]
539. Patel R, Portela D, Badley AD, Harmsen WS, Larson-Keller JJ, Ilstrup DM, Keating MR, Wiesner RH, Krom RA, Paya CV. Risk factors of invasive Candida and non-Candida fungal infections after liver transplantation. Transplantation 1996;62:926-934. [PubMed]
540. Paugam A, Baixench MT, Viguie C. An update on Candida dubliniensis. Med Mal Infec 2008;38:1-7. [PubMed]
541. Paul N, Mathai E, Abraham OC, Michael JS, Mathai D. Factors associated with candiduria and related mortality. J Infection 2007;55:450-455. [PubMed]
542. Paya CV, Guerra L, Marsh HM, Farnell MB, Washington J, Thompson RL. Limited usefulness of quantitative culture of blood drawn through the device for diagnosis of intravascular-device-related bacteremia. J Clin Microbiol 1989;27:1431-1433. [PubMed]
543. Pelletier R, Alarie I, Lagace R, Walsh TJ. Emergence of disseminated candidiasis caused by Candida krusei during treatment with caspofungin: Case report and review of literature. Med Mycol 2005;43:559-564. [PubMed]
544. Pelletier R, Peter J, Antin C, Gonzalez C, Wood L, Walsh TJ. Emergence of resistance of Candida albicans to clotrimazole in human immunodeficiency virus-infected children: In vitro and clinical correlations. J Clin Microbiol 2000;38:1563-8. [PubMed]
545. Pelz RK, Hendrix CW, Swoboda SM, Diener-West M, Merz WG, Hammond J, Lipsett PA. Double-blind placebo-controlled trial of fluconazole to prevent candidal infections in critically ill surgical patients. Ann Surg 2001;233:542-548. [PubMed]
546. Perea S, Gonzalez G, Fothergill AW, Kirkpatrick WR, Rinaldi MG, Patterson TF. In vitro interaction of caspofungin acetate with voriconazole against clinical isolates of Aspergillus spp. Antimicrob Agents Chemother 2002;46:3039-3041. [PubMed]
547. Perfect JR. Fungal virulence genes as targets for antifungal chemotherapy. Antimicrob Agents Chemother 1996;40:1577-1583. [PubMed]
548. Perfect JR, Klotman ME, Gilbert CC, Crawford DD, Rosner GL, Wright KA, Peters WP. Prophylactic intravenous amphotericin B in neutropenic autologous bone marrow transplant recipients. J Infect Dis 1992;165:891-897. [PubMed]
549. Perfect JR, Marr KA, Walsh TJ, Greenberg RN, DuPont B, de la Torre-Cisneros J, Just-Nubling G, Schlamm HT, Lutsar I, Espinel-Ingroff A, Johnson E. Voriconazole treatment for less-common, emerging, or refractory fungal infections. Clin Infect Dis 2003;36:1122-1131. [PubMed]
550. Perlin DS. Resistance to echinocandin-class antifungal drugs. Drug Resist Update 2007;10:121-30. [PubMed]
551. Perraut LE, Jr., Perraut LE, Bleiman B, Lyons J. Successful treatment of Candida albicans endophthalmitis with intravitreal amphotericin B. Arch Ophthalmol 1981;99:1565-7. [PubMed]
552. Petraitis V, Petraitiene R, Sarafandi AA, Keleher AM, Lyman CA, Casler HE, Sein T, Groll AH, Becher J, Avila NA, Walsh TJ. Combination therapy in treatment of experimental pulmonary aspergillosis: Synergistic interaction between an antifungal triazole and an echinocandin. J Infec Dis 2003;187:1834-1843. [PubMed]
553. Petranyi G, Meingassner JG, Mieth H. Antifungal activity of the allylamine derivative terbinafine in vitro. Antimicrob Agents Chemother 1987;31:1365-1368. [PubMed]
554. Petrikkos G, Skiada A, Sabatakou H, Antoniadou A, Dosios T, Giamarellou H. Case report. Successful treatment of two cases of post-surgical sternal osteomyelitis, due to Candida krusei and Candida albicans, respectively, with high doses of triazoles (fluconazole, itraconazole). Mycoses 2001;44:422-5. [PubMed]
555. Pfaller M, Cabezudo I, Koontz F, Bale M, Gingrich R. Predictive value of surveillance cultures for systemic infection due to Candida species. Eur J Clin Microbiol Infect Dis 1987;6:628-633. [PubMed]
556. Pfaller MA, Bale MJ, Buschelman B, Rhomberg P. Antifungal activity of a new triazole, D0870, compared with four other antifungal agents tested against clinical isolates of Candida and Torulopsis glabrata. Diagn Microbiol Infect Dis 1994;19:75-80. [PubMed]
557. Pfaller MA, Boyken L, Hollis RJ, Kroeger J, Messer SA, Tendolkar S, Diekema DJ. In vitro susceptibility of invasive isolates of Candida spp. to anidulafungin, caspofungin, and micafungin: Six years of global surveillance. J Clin Microbiol 2008a;46:150-156. [PubMed]
558. Pfaller MA, Boyken L, Hollis RJ, Messer SA, Tendolkar S, Diekema DJ. In vitro activities of anidulafungin against more than 2,500 clinical isolates of Candida spp., including 315 isolates resistant to fluconazole. J Clin Microbiol 2005;43:5425-5427.
559. Pfaller MA, Boyken L, Hollis RJ, Messer SA, Tendolkar S, Diekema DJ. Global surveillance of in vitro activity of micafungin against Candida: a comparison with caspofungin by CLSI-recommended methods. J Clin Microbiol 2006a;44:3533-3538. [PubMed]
560. Pfaller MA, Boyken L, Hollis RJ, Messer SA, Tendolkar S, Diekema DJ. In vitro susceptibilities of Candida spp. to caspofungin: Four years of global surveillance. J Clin Microbiol 2006b;44:760-763. [PubMed]
561. Pfaller MA, Diekema DJ. Rare and emerging opportunistic fungal pathogens: Concern for resistance beyond Candida albicans and Aspergillus fumigatus. J Clin Microbiol 2004;42:4419-4431. [PubMed]
562. Pfaller MA, Diekema DJ. Epidemiology of invasive candidiasis: A persistent public health problem. Clin Microbiol Rev 2007a;20:133-163. [PubMed]
563. Pfaller MA, Diekema DJ, Colombo AL, Kibbler C, Ng KP, Gibbs DL, Newell VA. Candida rugosa, an emerging fungal pathogen with resistance to azoles: Geographic and temporal trends from the ARTEMIS DISK antifungal surveillance program. J Clin Microbiol 2006c;44:3578-3582. [PubMed]
564. Pfaller MA, Diekema DJ, Gibbs DL, Newell VA, Ng KP, Colombo A, Finquelievich J, Barnes R, Wadula J. Geographic and temporal trends in isolation and antifungal susceptibility of Candida parapsilosis: a global assessment from the ARTEMIS DISK Antifungal Surveillance Program, 2001 to 2005. J Clin Microbiol 2008b;46:842-849.[PubMed]
565. Pfaller MA, Diekema DJ, Jones RN, Messer SA, Hollis RJ. Trends in antifungal susceptibility of Candida spp. isolated from pediatric and adult patients with bloodstream infections: SENTRY Antimicrobial Surveillance Program, 1997 to 2000. J Clin Microbiol 2002a;40:852-856. [PubMed]
566. Pfaller MA, Diekema DJ, Mendez M, Kibbler C, Erzsebet P, Chang SC, Gibbs DL, Newell VA. Candida guilliermondii, an opportunistic fungal pathogen with decreased susceptibility to fluconazole: Geographic and temporal trends from the ARTEMIS DISK antifungal surveillance program. J Clin Microbiol 2006d;44:3551-3556. [PubMed]
567. Pfaller MA, Diekema DJ, Messer SA, Hollis RJ, Jones RN. In vitro activities of caspofungin compared with those of fluconazole and itraconazole against 3,959 clinical isolates of Candida spp., including 157 fluconazole-resistant isolates. Antimicrob Agents Chemother 2003;47:1068-1071. [PubMed]
568. Pfaller MA, Diekema DJ, Ostrosky-Zeichner L, Rex JH, Alexander BD, Andes D, Brown SD, Chaturvedi V, Ghannoum MA, Knapp CC, Sheehan DJ, Walsh TJ. Correlation of MIC with outcome for Candida species tested against caspofungin, anidulafungin, and micafungin: Analysis and proposal for interpretive MIC breakpoints. J Clin Microbiol 2008c;46:2620-2629. [PubMed]
569. Pfaller MA, Diekema DJ, Rex JH, Espinel-Ingroff A, Johnson EM, Andes D, Chaturvedi V, Ghannoum MA, Odds FC, Rinaldi MG, Sheehan DJ, Troke P, Walsh TJ, Warnock DW. Correlation of MIC with outcome for Candida species tested against voriconazole: Analysis and proposal for interpretive breakpoints. J Clin Microbiol 2006e;44:819-826. [PubMed]
570. Pfaller MA, Diekema DJ, Sheehan DJ. Interpretive breakpoints for fluconazole and Candida revisited: a blueprint for the future of antifungal susceptibility testing. Clin Microbiol Rev 2006f;19:435-447,CP3,CP4. [PubMed]
571. Pfaller MA, Messer SA, Boyken L, Huynh H, Hollis RJ, Diekema DJ. In vitro activities of 5-fluorocytosine against 8,803 clinical isolates of Candida spp.: Global assessment of primary resistance using National Committee for Clinical Laboratory Standards susceptibility testing methods. Antimicrob Agents Chemother 2002b;46:3518-3521. [PubMed]
572. Pfaller MA, Messer SA, Boyken L, Rice C, Tendolkar S, Hollis RI, Diekema DJ. Use of fluconazole as a surrogate marker to predict susceptibility and resistance to voriconazole among 13,338 clinical isolates of Candida spp. tested by clinical and laboratory standards institute-recommended broth microdilution methods. J Clin Microbiol 2007b;45:70-75. [PubMed]
573. Pfaller MA, Messer SA, Gee S, Joly S, Pujol C, Sullivan DJ, Coleman DC, Soll DR. In vitro susceptibilities of Candida dubliniensis isolates tested against the new triazole and echinocandin antifungal agents. J Clin Microbiol 1999;37:870-872. [PubMed]
574. Pfaller MA, Messer SA, Hollis RJ. Variations in DNA subtype, antifungal susceptibility, and slime production among clinical isolates of Candida parapsilosis. Diagn Microbiol Infect Dis 1995a;21:9-14. [PubMed]
575. Pfaller MA, Messer SA, Mills K, Bolmstrom A, Jones RN. Evaluation of Etest method for determining caspofungin (MK-0991) susceptibilities of 726 clinical isolates of Candida species. J Clin Microbiol 2001a;39:4387-4389. [PubMed]
576. Pfaller MA, Rex JH, Rinaldi MG. Antifungal susceptibility testing: Technical advances and potential clinical applications. Clin Infect Dis 1996;24:776-784. [PubMed]
577. Pfaller MA, Rhine-Chalberg J, Barry AL, Rex JH, NIAID Mycoses Study Group, the Candidemia Study Group. Strain variation and antifungal susceptibility among bloodstream isolates of Candida species from 21 different medical institutions. Clin Infect Dis 1995b;21:1507-1509. [PubMed]
578. Pfaller MA, Yu WL. Antifungal susceptibility testing - New technology and clinical applications. Infect Dis Clin N Amer 2001b;15:1227-1261.[PubMed]
579. Phillips P, De Beule K, Frechette G, Tchamouroff S, Vandercam B, Weitner L, Hoepelman A, Stingl G, Clotet B. A double-blind comparison of itraconazole oral solution and fluconazole capsules for the treatment of oropharyngeal candidiasis in patients with AIDS. Clin Infect Dis 1998;26:1368-1373. [PubMed]
580. Phillips P, Shafran S, Garber G, Rotstein C, Smaill F, Fong I, Salit I, Miller M, Williams K, Conly JM, Singer J, Ioannou S, Canadian Candidemia Study Group. Multicenter randomized trial of fluconazole versus amphotericin B for treatment of candidemia in non-neutropenic patients. Eur J Clin Microbiol Infect Dis 1997;16:337-345. [PubMed]
581. Phillips P, Zemcov J, Mahmood W, Montaner JS, Craib K, Clarke AM. Itraconazole cyclodextrin solution for fluconazole-refractory oropharyngeal candidiasis in AIDS: correlation of clinical response with in vitro susceptibility. AIDS 1996;10:1369-1376. [PubMed]
582. Piarroux R, Grenouillet F, Balvay P, Tran W, Blasco G, Millon L, Boillot A. Assessment of preemptive treatment to prevent severe candidiasis in critically ill surgical patients. Crit Care Med 2004;32:2443-2449. [PubMed]
583. Pierrotti LC, Baddour LM. Fungal endocarditis, 1995-2000. Chest 2002;122:302-310. [PubMed]
584. Pirotta M, Gunn J, Chondros P, Grover S, O'Malley P, Hurley S, Garland S. Effect of lactobacillus in preventing post-antibiotic vulvovaginal candidiasis: a randomised controlled trial. Brit Med J 2004;329:548-551. [PubMed]
585. Pittard WBI, Thullen JD, Fanaroff AA. Neonatal septic arthritis. J Pediatr 1976;88:621-624. [PubMed]
586. Pittet D, Li N, Woolson RF, Wenzel RP. Microbiological factors influencing the outcome of nosocomial bloodstream infections: A 6-year validated, population-based model. Clin Infect Dis 1997;24:1068-1078. [PubMed]
587. Pittet D, Monod M, Suter PM, Frenk E, Auckenthaler R. Candida colonization and subsequent infections in critically ill surgical patients. Ann Surg 1994;220:751-758.[PubMed]
588. Pizzo PA, Robichaud KJ, Gill FA, Witebsky FG. Empiric antibiotics and antifungal therapy for cancer patients with prolonged fever and granulocytopenia. Am J Med 1982;72:101-111. [PubMed]
589. Playford EG, Webster AC, Sorrell TC, Craig JC. Antifungal agents for preventing fungal infections in non- neutropenic critically ill and surgical patients: systematic review and meta-analysis of randomized clinical trials. J Antimicrob Chemother 2006;57:628-638. [PubMed]
590. Plouffe JF, Brown DG, Silva J, Eck T, Stricof RL, Fekety FR. Nosocomial outbreak of Candida parapsilosis fungemia related to intravenous infusions. Arch Intern Med 1977;137:1686-1689. [PubMed]
591. Polak A. 5-Fluorocytosine--current status with special references to mode of action and drug resistance. Contrib Microbiol Immunol 1977;4:158-167. [PubMed]
592. Polak A. Combination therapy of experimental candidiasis, cryptococcosis, aspergillosis and wangiellosis in mice. Chemotherapy 1987;33:381-395. [PubMed]
593. Pons V, Greenspan D, Lozada-Nur F, McPhail L, Gallant JE, Tunkel A, Johnson CC, McCarty J, Panzer H, Levenstein M, Barranco A, Green S. Oropharyngeal candidiasis in patients with AIDS: Randomized comparison of fluconazole versus nystatin oral suspensions. Clin Infect Dis 1997;27:1204-1207. [PubMed]
594. Powderly WG. Prophylaxis for opportunistic infections in an era of effective antiretroviral therapy. Clin Infect Dis 2000;31:597-601. [PubMed]
595. Powderly WG, Finkelstein DM, Feinberg J, Frame P, He W, van der Horst C, Koletar SL, Eyster ME, Carey J, Waskin H, Hooton TM, Hyslop N, Specton SA, Bozzette SA, the NIAID AIDS Clinical Trials Group. A randomized trial comparing fluconazole with clotrimazole troches for the prevention of fungal infections in patients with advanced human immunodeficiency virus infection. N Engl J Med 1995;332:700-705. [PubMed]
596. Powers JH, Higgins KM. Itraconazole versus fluconazole for antifungal prophylaxis. Ann Intern Med 2004;140:580. [PubMed]
597. Prabhu RM, Orenstein R. Failure of caspofungin to treat brain abscesses secondary to Candida albicans prosthetic valve endocarditis. Clin Infect Dis 2004;39:1253-4.[PubMed]
598. Price MF, LaRocco MT, Gentry LO. Fluconazole susceptibilities of Candida species and distribution of species recovered from blood cultures over a 5-year period. Antimicrob Agents Chemother 1994;38:1422-1424. [PubMed]
599. Pujol C, Pfaller MA, Soll DR. Flucytosine resistance is restricted to a single genetic clade of Candida albicans. Antimicrob Agents Chemother 2004;48:262-266. [PubMed]
600. Raad I, Hanna H, Boktour M, Girgawy E, Danawi H, Mardani M, Kontoyiannis D, Darouiche R, Hachem R, Bodey GP. Management of central venous catheters in patients with cancer and candidemia. Clin Infect Dis 2004;38:1119-1127. [PubMed]
601. Rabinovici R, Szewczyk D, Ovadia P, Greenspan JR, Sivalingam JJ. Candida pericarditis: clinical profile and treatment. Ann Thorac Surg 1997;63:1200-1204. [PubMed]
602. Rajendram R, Alp NJ, Mitchell AR, Bowler I, Forfar JC. Candida prosthetic valve endocarditis cured by caspofungin therapy without valve replacement. Clin Infect Dis 2005;40:E72-E74. [PubMed]
603. Rantala A, Lehtonen OP, Kuttila K, Havia T, Niinikoski J. Diagnostic factors for postoperative candidosis in abdominal surgery. Annales Chirurgiae et Gynaecologiae 1991;80:323-328. [PubMed]
604. Reboli AC, Rotstein C, Pappas PG, Chapman SW, Kett DH, Kumar D, Betts R, Wible M, Goldstein BP, Schranz J, Krause DS, Walsh TJ, Van Wijngaerden E, Bow E, Garber G, Laverdiere M, Libman M, Pelletier R, Sanche S, Cornely O, Kern W, Ruhnke M, Carosi G, Verweij P, Anaissie E, Bochan M, Carpenter C, Cicogna C, Cleary J, Finley N, Fetchick R, Friedman B, Graham D, Graybill R, Hsiao C, Jones R, Kerkering T, Kurtz T, McClain D, Nowakowski J, Ostrosky-Zeichner L, Perfect J, Pullman J, Quartin A, Reinhardt J, Segal B, Shahryar S, Shoham S, Sioson P, Sloan L, Solomkin J, Vazquez J, Zapata-Molina N. Anidulafungin versus fluconazole for invasive candidiasis. N Engl J Med 2007;356:2472-2482. [PubMed]
605. Redding S, Smith J, Farinacci G, Rinaldi M, Fothergill A, Rhine-Chalberg J, Pfaller M. Resistance of Candida albicans to fluconazole during treatment of oropharyngeal candidiasis in a patient with AIDS: documentation by in vitro susceptibility testing and DNA subtype analysis. Clin Infect Dis 1994;18:240-242. [PubMed]
606. Reed C, Bryant R, Ibrahim AS, Edwards J, Jr., Filler SG, Goldberg R, Spellberg B. Combination polyene-caspofungin treatment of rhino-orbital- cerebral mucormycosis. Clin Infect Dis 2008;47:364-371. [PubMed]
607. Reller ME, Mallonee AB, Kwiatkowski NP, Merz WG. Use of peptide nucleic acid-fluorescence in situ hybridization for definitive, rapid identification of five common Candida species. J Clin Microbiol 2007;45:3802-3803. [PubMed]
608. Rello J, Esandi ME, Diaz E, Mariscal D, Gallego M, Valles J. The role of Candida sp. isolated from bronchoscopic samples in nonneutropenic patients. Chest 1998;114:146-149.[PubMed]
609. Rennert G, Rennert HS, Pitlik S, Finkelstein R, Kitzes-Cohen R. Epidemiology of candidemia - A nationwide survey in Israel. Infection 2000;28:26-29. [PubMed]
610. Revankar SG, Kirkpatrick WR, McAtee RK, Fothergill AW, Redding SW, Rinaldi MG, Hilsenbeck SG, Patterson TF. A randomized trial of continuous or intermittent therapy with fluconazole for oropharyngeal candidiasis in HIV-infected patients: Clinical outcomes and development of fluconazole resistance. Am J Med 1998;105:7-11.[PubMed]
611. Rex JH. Antifungal prophylaxis in the intensive care unit: Who should get it? Crit Care Med 2006;34:1286-1287. [PubMed]
612. Rex JH, Anaissie EJ, Boutati E, Estey E, Kantarjian H. Systemic antifungal prophylaxis reduces invasive fungal infections in acute myelogenous leukemia: a retrospective review of 833 episodes of neutropenia in 322 adults. Leukemia 2002a;16:1197-1199. [PubMed]
613. Rex JH, Bennett JE, Sugar AM, Pappas PG, Serody J, Edwards JE, Washburn RG, the NIAID Mycoses Study Group, the Candidemia Study Group. Intravascular catheter exchanges and the duration of candidemia. Clin Infect Dis 1995a;21:994-996. PubMed]
614. Rex JH, Bennett JE, Sugar AM, Pappas PG, Van der Horst CM, Edwards JE, Washburn RG, Scheld WM, Karchmer AW, Dine AP, Levenstein MJ, Webb CD, the Candidemia Study Group, the NIAID Mycoses Study Group. A randomized trial comparing fluconazole with amphotericin B for the treatment of candidemia in patients without neutropenia. N Engl J Med 1994;331:1325-1330. [PubMed]
615. Rex JH, Bhalla SC, Cohen DM, Hester JP, Vartivarian SE, Anaissie EJ. Protection of human polymorphonuclear leukocyte function from the deleterious effects of isolation, irradiation, and storage by interferon-g and granulocyte colony-stimulating factor. Transfusion 1995b;35:605-611. [PubMed]
616. Rex JH, Cooper CR, Jr., Merz WG, Galgiani JN, Anaissie EJ. Detection of amphotericin B-resistant Candida isolates in a broth-based system. Antimicrob Agents Chemother 1995c;39:906-909. [PubMed]
617. Rex JH, Pappas PG, Karchmer AW, Sobel J, Edwards JE, Hadley S, Brass C, Vazquez JA, Chapman SW, Horowitz HW, Zervos M, McKinsey D, Lee J, Babinchak T, Bradsher RW, Cleary JD, Cohen DM, Danziger L, Goldman M, Goodman J, Hilton E, Hyslop NE, Kett DH, Lutz J, Rubin RH, Scheld WM, Schuster M, Simmons B, Stein DK, Washburn RG, Mautner L, Chu TC, Panzer H, Rosenstein RB, Booth J. A randomized and blinded multicenter trial of high-dose fluconazole plus placebo versus fluconazole plus amphotericin B as therapy for candidemia and its consequences in nonneutropenic subjects. Clin Infect Dis 2003;36:1221-8. [PubMed]
618. Rex JH, Pfaller MA. Has antifungal susceptibility testing come of age? Clin Infect Dis 2002b;35:982-989. [PubMed]
619. Rex JH, Pfaller MA, Barry AL, Nelson PW, Webb CD, the NIAID Mycoses Study Group and the Candidemia Study Group. Antifungal susceptibility testing of isolates from a randomized, multicenter trial of fluconazole vs. amphotericin B as treatment of non-neutropenic patients with candidemia. Antimicrob Agents Chemother 1995d;39:40-44.[PubMed]
620. Rex JH, Pfaller MA, Galgiani JN, Bartlett MS, Espinel-Ingroff A, Ghannoum MA, Lancaster M, Odds FC, Rinaldi MG, Walsh TJ, Barry AL, Subcommittee on Antifungal Susceptibility Testing of the National Committee for Clinical Laboratory Standards. Development of interpretive breakpoints for antifungal susceptibility testing: conceptual framework and analysis of in vitro-in vivo correlation data for fluconazole, itraconazole, and Candida infections. Clin Infect Dis 1997;24:235-247. [PubMed]
621. Rex JH, Pfaller MA, Rinaldi MG, Polak A, Galgiani JN. Antifungal susceptibility testing. Clin Microbiol Rev 1993;6:367-381. [PubMed]
622. Rex JH, Pfaller MA, Walsh TJ, Chaturvedi V, Espinel-Ingroff A, Ghannoum MA, Gosey LL, Odds FC, Rinaldi MG, Sheehan DJ, Warnock DW. Antifungal susceptibility testing: Practical aspects and current challenges. Clin Microbiol Rev 2001a;14:643-658. [PubMed]
623. Rex JH, Rinaldi MG, Pfaller MA. Resistance of Candida species to fluconazole. Antimicrob Agents Chemother 1995e;39:1-8. [PubMed]
624. Rex JH, Sobel JD. Prophylactic antifungal therapy in the intensive care unit. Clin Infect Dis 2001b;32:1191-1200. [PubMed]
625. Rhoads JL, Wright DC, Redfield RR, Burke DS. Chronic vaginal candidiasis in women with human immunodeficiency virus infection. JAMA 1987;257:3105-7. [PubMed]
626. Richter JM, Jacoby GA, Schapiro H, Warshaw AL. Pancreatic abscess due to Candida albicans. Ann Intern Med 1982;97:221-2. [PubMed]
627. Rigby S, Procop GW, Haase G, Wilson D, Hall G, Kurtzman C, Oliveira K, Von Oy S, Hyldig-Nielsen JJ, Coull J, Stender H. Fluorescence in situ hybridization with peptide nucleic acid probes for rapid identification of Candida albicans directly from blood culture bottles. J Clin Microbiol 2002;40:2182-2186. [PubMed]
628. Roberts DT. Oral therapeutic agents in fungal nail disease. J Amer Acad Dermatol 1994;31:S78-81. [PubMed]
629. Rodriguez D, Park BJ, Almirante B, Cuenca-Estrella M, Planes AM, Mensa J, Gimenez M, Saballs P, Fridkin SK, Rodriguez-Tudela JL, Pahissa A. Impact of early central venous catheter removal on outcome in patients with candidaemia. Clin Microbiol Infect 2007;13:788-793. [PubMed]
630. Rodriguez-Adrian LJ, King RT, Tamayo-Derat LG, Miller JW, Garcia CA, Rex JH. Retinal lesions as clues to disseminated bacterial and candidal infections - Frequency, natural history, and etiology. Medicine 2003;82:187-202.[PubMed]
631. Rodriguez-Tudela JL, Almirante B, Rodriguez-Pardo D, Laguna F, Donnelly JP, Mouton JW, Pahissa A, Cuenca-Estrella M. Correlation of the MIC and Dose/MIC ratio of fluconazole to the therapeutic response of patients with mucosal candidiasis and candidemia. Antimicrob Agents Chemother 2007a;51:3599-3604. [PubMed]
632. Rodriguez-Tudela JL, Donnelly JP, Arendrup MC, Arikan S, Barchiesi F, Bille J, Chryssanthou E, Cuenca-Estrella M, Dannaoui E, Denning D, Fegeler W, Gaustad P, Lass-Flori C, Moore C, Richardson M, Schmalreck A, Velegraki JA, Verweij P. EUCAST Technical Note on voriconazole - Subcommittee on antifungal susceptibility testing (AFST) of the ESCMID European committee for antimicrobial susceptibility testing (EUCAST). Clin Microbiol Infect 2008;14:985-987. [PubMed]
633. Rodriguez-Tudela JL, Donnelly JP, Pfaller MA, Chryssantou E, Warn P, Denning DW, Espinel-Ingroff A, Barchiesi F, Cuenca-Estrella M. Statistical analyses of correlation between fluconazole MICs for Candida spp. assessed by standard methods set forth by the European Committee on Antimicrobial Susceptibility Testing (E.Dis. 7.1) and CLSI (M27-A2). J Clin Microbiol 2007b;45:109-111.
634. Rohner P, Pepey B, Auckenthaler R. Comparison of BacT/Alert with Signal blood culture system. J Clin Microbiol 1995;33:313-317. [PubMed]
635. Roseeuw D, De Doncker P. New approaches to the treatment of onychomycosis. J Amer Acad Dermatol 1993;29:S45-S50. [PubMed]
636. Roupie E, Darmon J-Y, Brochard L, Saada M, Rekik N, Brun-Buisson C. Fluconazole therapy of candidal native valve endocarditis. Eur J Clin Microbiol Infect Dis 1991;10:458-459. [PubMed]
637. Rowen JL. Mucocutaneous candidiasis. Semin Perinatol 2003;27:406-413. [PubMed]
638. Roy B, Meyer SA. Confirmation of the distinct genotype groups within the form species Candida parapsilosis. J Clin Microbiol 1998;36:216-218. [PubMed]
639. Ruhnke M, Bohme A, Buchheidt D, Donhuijsen K, Einsele H, Enzensberger R, Glasmacher A, Gumbel H, Heussel CP, Karthaus M, Lambrecht E, Sudhoff T, Szelenyi H. Diagnosis of invasive fungal infections in hematology and oncology - Guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Oncology (DGHO). Ann Hematol 2003;82:S141-S148. [PubMed]
640. Ruhnke M, Kuse E, Chetchotisakd P, Arns da cunha C, Diekmann-Berndt H. Comparison of micafungin and liposomal amphotericin B for invasive candidiasis. 45th Interscience Conference on Antimicrobial Agents and Chemotherapy. Washington, DC, 2005, Abstract No. M-722c. [PubMed]
641. Ryder NS, Wagner S, Leitner I. In vitro activities of terbinafine against cutaneous isolates of Candida albicans and other pathogenic yeasts. Antimicrob Agents Chemother 1998;42:1057-1061. [PubMed]
642. Saag MS, Fessel WJ, Kaufman CA, Merrill KW, Ward DJ, Moskovitz BL, Thomas C, Oleka N, Guarnieri JA, Lee J, Brenner-Gati L, Klausner M. Treatment of fluconazole-refractory oropharyngeal candidiasis with itraconazole oral solution in HIV-positive patients. AIDS Res Hum Retroviruses 1999;15:1413-7. [PubMed]
643. Safdar A, Hanna HA, Boktour M, Kontoyiannis DP, Hachem R, Lichtiger B, Freireich EJ, Raad, II. Impact of high-dose granulocyte transfusions in patients with cancer with candidemia - Retrospective case-control analysis of 491 episodes of Candida species bloodstream infections. Cancer 2004;101:2859-2865. [PubMed]
644. Safdar N, Slattery WR, Knasinski V, Gangnon RE, Li ZH, Pirsch JD, Andes D. Predictors and outcomes of candiduria in renal transplant recipients. Clin Infect Dis 2005;40:1413-1421. [PubMed]
645. Samaranayake LP, Holmstrup P. Oral candidiasis and human immunodeficiency virus infection. Journal of Oral Pathology & Medicine 1989;18:554-564. [PubMed]
646. Sancak B, Rex JH, Chen E, Marr K. Comparison of PCR- and HinfI restriction endonuclease-based methods for typing of Candida krusei isolates. J Clin Microbiol 2004;42:5889-91. [PubMed]
647. Sanchez PJ, Siegel JD, Fishbein J. Candida endocarditis: successful medical management in three preterm infants and review of the literature. Pediatr Infect Dis J 1991;10:239-43. [PubMed]
648. Sanchez V, Vazquez JA, Barth-Jones D, Dembry L, Sobel JD, Zervos MJ. Nosocomial acquisition of Candida parapsilosis: an epidemiologic study. Am J Med 1993;94:577-82. [PubMed]
649. Sanchez-Portocarrero J, Martin-Rabadan P, Saldana CJ, Perez-Cecilia E. Candida cerebrospinal fluid shunt infection. Report of two new cases and review of the literature. Diagn Microbiol Infect Dis 1994;20:33-40. [PubMed]
650. Sanchez-Portocarrero J, Perez-Cecilia E, Corral O, Romero-Vivas J, Picazo JJ. The central nervous system and infection by Candida species. Diagn Microbiol Infect Dis 2000;37:169-179. [PubMed]
651. Sandven P, Giercksky KE. Yeast colonization in surgical patients with intra-abdominal perforations. Eur J Clin Microbiol Infect Dis 2001;20:475-481. [PubMed]
652. Sandven P, Qvist H, Skovlund E, Giercksky KE. Significance of Candida recovered from intraoperative specimens in patients with intra-abdominal perforations. Crit Care Med 2002;30:541-547. [PubMed]
653. Sanford JP. The enigma of candiduria: Evolution of bladder irrigation with Amphotericin B for management - from anecdote to dogma and a lesson from Machiavelli. J Infect Dis 1993;16:145-147. [PubMed]
654. Santos JA, Beceiro J, Hernandez R, Salas S, Escriba R, Frias EG, Rodriguez JP, Quero J. Congenital cutaneous candidiasis: Report of four cases and review of the literature. Eur J Pediatr 1991;150:336-338. [PubMed]
655. Sarria JC, Bradley JC, Habash R, Mitchell KT, Kimbrough RC, Vidal AM. Candida glabrata endophthalmitis treated successfully with caspofungin. Clin Infect Dis 2005;40:E46-E48. [PubMed]
656. Savani DV, Perfect JR, Cobo LM, Durack DT. Penetration of new azole compounds into the eye and efficacy in experimental Candida endophthalmitis. Antimicrob Agents Chemother 1987;31:6-10. [PubMed]
657. Sawyer RG, Adams RB, Rosenlof LK, May AK, Pruett TL. Effectiveness of fluconazole in murine Candida albicans and bacterial C. albicans peritonitis and abscess formation. J Med Vet Mycol 1995;33:131-136. [PubMed]
658. Saxen H, Hoppu K, Pohjavuori M. Pharmacokinetics of fluconazole in very low birth weight infants during the first two weeks of life. Clin Pharmacol Ther 1993;54:269-277. [PubMed]
659. Scarcella A, Pasquariello MB, Giugliano B, Vendemiia M, De Lucia A. Lipsomal amphotericin B treatment for neonatal fungal infections. Pediatr Infect Dis J 1998;17:146-148. [PubMed]
660. Schaffner A, Böhler A. Amphotericin B refractory aspergillosis after itraconazole: evidence for significant antagonism. Mycoses 1993;36:421-424. [PubMed]
661. Schaffner A, Frick PG. The effect of ketoconazole on amphotericin B in a model of disseminated aspergillosis. J Infect Dis 1985;151:902-910. [PubMed]
662. Schaffner A, Schaffner M. Effect of prophylactic fluconazole on the frequency of fungal infections, amphotericin B use, and health care costs in patients undergoing intensive chemotherapy for hematologic neoplasias. J Infect Dis 1995;172:1035-1041. [PubMed]
663. Scheven M, Scheven C, Hahn K, Senf A. Post-antibiotic effect and post-exposure polyene antagonism of azole antimycotics in Candida albicans: dependency on lipophilia. Mycoses 1995a;38 (Suppl. 1):14-21. [PubMed]
664. Scheven M, Scheven M-L. Interaction betweeen azoles and amphotericin B in the treatment of candidiasis. Clin Infect Dis 1995b;20:1079. [PubMed]
665. Scheven M, Schwegler F. Antagonistic interactions between azoles and amphotericin B with yeasts depend on azole lipophilia for special test conditions in vitro. Antimicrob Agents Chemother 1995c;39:1779-1783. [PubMed]
666. Schiffer CA. Granulocyte transfusion therapy 2006: The comeback kid? Med Mycol 2006;44:S383-S386. [PubMed]
667. Schrank JH, Jr., Dooley DP. Purulent pericarditis caused by Candida species: case report and review. Clin Infect Dis 1995;21:182-187. [PubMed]
668. Schuman P, Sobel JD, Ohmit SE, Mayer KH, Carpenter CCJ, Rompalo A, Duerr A, Smith DK, Warren D, Klein RS. Mucosal candidal colonization and candidiasis in women with or at risk for human immunodeficiency virus infection. Clin Infect Dis 1998;27:1161-1167. [PubMed]
669. Schuster MG, Edwards JE, Jr., Sobel JD, Darouiche RO, Karchmer AW, Hadley S, Slotman G, Panzer H, Biswas P, Rex JH. Empirical fluconazole versus placebo for intensive care unit patients - A randomized trial. Ann Intern Med 2008;149:83-90. [PubMed]
670. Seay RE, Larson TA, Toscano JP, Bostrom BC, O'Leary MC, Uden DL. Pharmcokinetics of fluconazole in immune-compromised children with leukemia or other hematologic disease. Pharmacotherapy 1995;15:52-58. [PubMed]
671. Sebti A, Kiehn TE, Perlin D, Chaturvedi V, Wong M, Doney A, Park S, Sepkowitz KA. Candida dubliniensis at a cancer center. Clin Infect Dis 2001;32:1034-1038.[PubMed]
672. Segal BH, Steinbach WJ. Combination antifungals: an update. Expert Rev Anti-Infect Ther 2007;5:883-892. [PubMed]
673. Seibel NL, Schwartz C, Arrieta A, Flynn P, Shad A, Albano E, Keirns J, Lau WM, Facklam DP, Buell DN, Walsh TJ. Safety, tolerability, and pharmacokinetics of micafungin (FK463) in febrile neutropenic pediatric patients. Antimicrob Agents Chemother 2005;49:3317-3324. [PubMed]
674. Senn L, Robinson JO, Schmidt S, Knaup M, Asahi N, Satomura S, Matsuura S, Duvoisin B, Bille J, Calandra T, Marchetti O. 1,3-beta-D-glucan antigenemia for early diagnosis of invasive fungal infections in neutropenic patients with acute leukemia. Clin Infect Dis 2008;46:878-885. [PubMed]
675. Seravalli L, Van Linthoudt D, Bernet C, de Torrente A, Marchetti O, Porchet F, Genne D. Candida glabrata spinal osteomyelitis involving two contiguous lumbar vertebrae: a case report and review of the literature. Diagn Microbiol Infect Dis 2003;45:137-141. [PubMed]
676. Sharpe MD, Ghent C, Grant D, Horbay GLA, McDougal J, Colby WD. Efficacy and safety of itraconazole prophylaxis for fungal infections after orthotopic liver transplantation: A prospective, randomized, double-blind study. Transplantation 2003;76:977-983. [PubMed]
677. Shechtman LB, Funaro L, Robin T, Bottone EJ, Cuttner J. Clotrimazole treatment of oral candidiasis in patients with neoplastic disease. Am J Med 1984;76:91-4. [PubMed]
678. Shepard JR, Addison RM, Alexander BD, Della-Latta P, Gherna M, Haase G, Hall G, Johnson JK, Merz WG, Peltroche-Llacsahuanga H, Stender H, Venezia RA, Wilson D, Procop GW, Wu F, Fiandaca MJ. Multicenter evaluation of the Candida albicans/Candida glabrata peptide nucleic acid fluorescent in situ hybridization method for simultaneous dual-color identification of C. albicans and C. glabrata directly from blood culture bottles. J Clin Microbiol 2008;46:50-55. [PubMed]
679. Shin JH, Kee SJ, Shin MG, Kim SH, Shin DH, Lee SK, Suh SP, Ryang DW. Biofilm production by isolates of Candida species recovered from nonneutropenic patients: Comparison of bloodstream isolates with isolates from other sources. J Clin Microbiol 2002;40:1244-1248. [PubMed]
680. Shoham S, Shaffer R, Sweet L, Cooke R, Donegan N, Boyce S. Candidemia in patients with ventricular assist devices. Clin Infect Dis 2007;44:E9-E12. [PubMed]
681. Shorr AF, Chung K, Jackson WL, Waterman PE, Kollef MH. Fluconazole prophylaxis in critically ill surgical patients: a meta-analysis. Crit Care Med 2005;33:1928-35.[PubMed]
682. Shorr AF, Lazarus DR, Sherner JH, Jackson WL, Morrel M, Fraser VJ, Kollef MH. Do clinical features allow for accurate prediction of fungal pathogenesis in bloodstream infections? Potential implications of the increasing prevalence of non-albicans candidemia. Crit Care Med 2007;35:1077-1083. [PubMed]
683. Silva-Cruz A, Andrade L, Sobral L, Francisca A. Itraconazole versus placebo in the management of vaginal candidiasis. Int J Gynaecol Obstet 1991;36:229-235. [PubMed]
684. Silveira LH, Cuellar ML, Citera G, Cabrera GE, Scopelitis E, Espinoza LR. Candida arthritis. Rheumatic Diseases Clinics of North America 1993;19:427-37. [PubMed]
685. Sim JP, Kho BC, Liu HS, Yung R, Chan JC. Candida tropicalis arthritis of the knee in a patient with acute lymphoblastic leukaemia: successful treatment with caspofungin. Hong Kong Med J 2005;11:120-3. [PubMed]
686. Singh S, Sobel JD, Bhargava P, Boikov D, Vazquez JA. Vaginitis due to Candida krusei: Epidemiology, clinical aspects, and therapy. Clin Infect Dis 2002;35:1066-1070.[PubMed]
687. Skiest DJ, Vazquez JA, Anstead GM, Graybill JR, Reynes J, Ward D, Hare R, Boparai N, Isaacs R. Posaconazole for the treatment of azole-refractory oropharyngeal and esophageal candidiasis in subjects with HIV infection. Clin Infect Dis 2007;44:607-614. [PubMed]
688. Slavin MA, Osborne B, Adams R, Levenstein MJ, Schoch HG, Feldman AR, Meyers JD, Bowden RA. Efficacy and safety of fluconazole prophylaxis for fungal infections after bone marrow transplantation--A prospective, randomized, double-blind study. J Infect Dis 1995;171:1545-1552. [PubMed]
689. Smego RA, Jr., Perfect JR, Durack DT. Combined therapy with amphotericin B and 5-fluorocytosine for Candida meningitis. Rev Infect Dis 1984;6:791-801. [PubMed]
690. Smith D, Andes D. Therapeutic drug monitoring of antifungals: Pharmacokinetic and pharmacodynamic considerations. Ther Drug Monit 2008;30:167-172. [PubMed]
691. Smith D, Midgley J, Gazzard B. A randomised, double-blind study of itraconazole versus placebo in the treatment and prevention of oral or oesophageal candidosis in patients with HIV infection. Int J Clin Pract 1999;53:349-352. [PubMed]
692. Smith DE, Midgley J, Allan M, Connolly GM, Gazzard BG. Itraconazole versus ketoconazole in the treatment of oral and oesophageal candidosis in patients infected with HIV. AIDS 1991;5:1367-1371. [PubMed]
693. Smith J, Safdar N, Knasinski V, Simmons W, Bhavnani SM, Ambrose PG, Andes D. Voriconazole therapeutic drug monitoring. Antimicrob Agents Chemother 2006;50:1570-1572. [PubMed]
694. Smith K, Youle M, Baker B, Ballinger J, Cuthbertson Z, Johnson M. Resolution of azole-resistant oesophageal candidiasis in an AIDS patient after treatment with caspofungin. Aids 2003;17:448-449. [PubMed]
695. Smith KJ, Warnock DW, Kennedy CT, Johnson EM, Hopwood V, Van Cutsem J, Vanden Bossche H. Azole resistance in Candida albicans. J Med Vet Mycol 1986;24:133-144. [PubMed]
696. Sobel JD. Recurrent vulvovaginal candidiasis. A prospective study of the efficacy of maintenance ketoconazole therapy. N Engl J Med 1986;315:1455-1458. [PubMed]
697. Sobel JD. Treatment of recurrent vulvovaginal candidiasis with maintenance fluconazole. Int J Gynecol Obstet 1992;37:17-34. [PubMed]
698. Sobel JD. Candidal vulvovaginitis. Clin Obstet Gynecol 1993;36:153-165. [PubMed]
699. Sobel JD. Changing epidemiology of invasive candidiasis in intensive care units - Much ado about nothing? Crit Care Med 2008;36:2188-2189. [PubMed]
700. Sobel JD, Bradshaw SK, Lipka CJ, Kartsonis NA. Caspofungin in the treatment of symptomatic candiduria. Clin Infect Dis 2007a;44:e46-9. Epub 2007 Jan 22. [PubMed]
701. Sobel JD, Brooker D, Stein GE, Thomason JL, Wermeling DP, Bradley B, Weinstein L, the Fluconazole Vaginitis Study Group. Single oral dose fluconazole compared with conventional clotrimazole topical therapy of Candida vaginitis. Am J Obstet Gynecol 1995;172:1263-1268. [PubMed]
702. Sobel JD, Chaim W. Treatment of torulopsis glabrata vaginitis: A retrospective review of boric acid therapy. Clin Infect Dis 1997;24:649-652. [PubMed]
703. Sobel JD, Chaim W, Nagappan V, Leaman D. Treatment of vaginitis caused by Candida glabrata: Use of topical boric acid and flucytosine. Amer J Obstet Gynecol 2003a;189:1297-1300. [PubMed]
704. Sobel JD, Haim W. Treatment of C. glabrata vaginitis with boric acid and flucytosine. Am J Obstet Gynecol 2003b;(in press). [PubMed]
705. Sobel JD, Kapernick PS, Zervos M, Reed BD, Hooton T, Soper D, Nyirjesy P, Heine MW, Willems J, Panzer H, Wittes H. Treatment of complicated Candida vaginitis: Comparison of single and sequential doses of fluconazole. Amer J Obstet Gynecol 2001a;185:363-369. [PubMed]
706. Sobel JD, Kauffman CA, McKinsey D, Zervos M, Vazquez JA, Karchmer AW, Lee J, Thomas C, Panzer H, Dismukes WE. Candiduria: A randomized, double-blind study of treatment with fluconazole and placebo. Clin Infect Dis 2000;30:19-24. [PubMed]
707. Sobel JD, Ohmit SE, Schuman P, Klein RS, Mayer K, Duerr A, Vazquez JA, Rompalo A. The evolution of Candida species and fluconazole susceptibility among oral and vaginal isolates recovered from human immunodeficiency virus (HIV)-seropositive and at-risk HIV- seronegative women. J Infec Dis 2001b;183:286-293. [PubMed]
708. Sobel JD, Revankar SG. Echinocandins - First-choice or first-line therapy for invasive candidiasis? N Engl J Med 2007b;356:2525-2526. [PubMed]
709. Sobel JD, Vazquez J. Candidiasis in the intensive care unit. Semin Respir Crit Care Med 2003c;24:99-111. [PubMed]
710. Sobel JD, Wiesenfeld HC, Martens M, Danna P, Hooton TM, Rompalo A, Sperling M, Livengood CI, Horowitz B, Von Thron J, Edwards L, Panzer H, Chu T. Maintenance fluconazole therapy for recurrent vulvovaginal candidiasis. N Engl J Med 2004;351:876-883. [PubMed]
711. Sobue S, Sekiguchi K, Nabeshima T. Intracutaneous distributions of fluconazole, itraconazole, and griseofulvin in guinea pigs and binding to human stratum corneum. Antimicrob Agents Chemother 2004;48:216-223. [PubMed]
712. Soczo G, Kardos G, Varga I, Kelentey B, Gesztelyi R, Majoros L. In vitro study of Candida tropicalis isolates exhibiting paradoxical growth in the presence of high concentrations of caspofungin. Antimicrob Agents Chemother 2007;51:4474-4476. [PubMed]
713. Soll DR. High-frequency switching in Candida albicans. Clin Microbiol Rev 1992;5:183-203. [PubMed]
714. Solomkin JS, Flohr AB, Quie PG, Simmons RL. The role of Candida in intraperitoneal infections. Surgery 1980a;88:524-530. [PubMed]
715. Solomkin JS, Simmons RL. Candida infection in surgical patients. World J Surgery 1980b;4:381-394. [PubMed]
716. Soltani M, Tobin CM, Bowker KE, Sunderland J, MacGowan AP, Lovering AM. Evidence of excessive concentrations of 5-flucytosine in children aged below 12 years: a 12-year review of serum concentrations from a UK clinical assay reference laboratory. Int J Antimicrobial Agents 2006;28:574-577. [PubMed]
717. Spellberg BJ, Filler SG, Edwards JE, Jr. Current treatment strategies for disseminated candidiasis. Clin Infect Dis 2006;42:244-251. [PubMed]
718. Spinillo A, Michelone G, Cavanna C, Colonna L, Capuzzo E, Nicola S. Clinical and microbiological characteristics of symptomatic vulvovaginal candidiasis in HIV-seropositive women. Genitourin Med 1994;70:268-72. [PubMed]
719. Stamm WE. Catheter-associated urinary tract infections: epidemiology, pathogenesis, and prevention. Am J Med 1991;91 (Suppl. 3B):65S-71S. [PubMed]
720. Steinbach WJ. Antifungal agents in children. Pediat Clin N Amer 2005a;52:895-915. [PubMed]
721. Steinbach WJ, Perfect JR, Cabell CH, Fowler VG, Corey GR, Li JS, Zaas AK, Benjamin DK, Jr. A meta-analysis of medical versus surgical therapy for Candida endocarditis. J Infection 2005b;51:230-247. [PubMed]
722. Stemmer SM, Maor Y, Hardan I. Oral fluconazole for empiric treatment of prolonged fever in neutropenic patients - Prospective study in 250 consecutive patients after stem cell transplantation. Amer J Clin Oncol-Canc Clin T 2004;27:328-332. [PubMed]
723. Sterling TR, Gasser RA, Jr., Ziegler A. Emergence of resistance to amphotericin B during therapy for Candida glabrata infection in an immunocompetent host. Clin Infect Dis 1996;23:187-188. [PubMed]
724. Stern GA, Fetkenhour CL, O'Grady RB. Intravitreal amphotericin B treatment of Candida endophthamitis. Arch Ophthalmol 1977;95:89-93. [PubMed]
725. Stevens DA. A possible mechanism for synergy between antifungal therapy and immune defenses. J Infec Dis 2008;198:159-162. [PubMed]
726. Stevens DA, Greene SI, Lang OS. Thrush can be prevented in patients with acquired immunodeficiency syndrome and the acquired immunodeficiency syndrome--related complex. Randomized, double-blind, placebo-controlled study of 100-mg oral fluconazole daily. Arch Intern Med 1991;151:2458-2464. [PubMed]
727. Stiller RL, Bennett JE, Scholer HJ, Wall M, Polak A, Stevens DA. Susceptibility to 5-fluorocytosine and prevalence of serotype in 402 Candida albicans isolates from the United States. Antimicrob Agents Chemother 1982;22:482-487. [PubMed]
728. Strauss RG. Granulocyte transfusion therapy. Hematol Oncol Clin N Amer 1994;8:1159-1166. [PubMed]
729. Strinden WD, Helgerson RB, Maki DG. Candida septic thrombosis of the great central veins associated with central catheters. Ann Surg 1985;202:653-658. [PubMed]
730. Sugar AM. Antifungal therapy in CAPD peritonitis--Do we have a choice. Seminars in Dialysis 1991;4:145-146. [PubMed]
731. Sugar AM. Use of amphotericin B with azole antifungal drugs: What are we doing? Antimicrob Agents Chemother 1995a;39:1907-1912. [PubMed]
732. Sugar AM, Hitchcock CA, Troke PF, Picard M. Combination therapy of murine invasive candidiasis with fluconazole and amphotericin B. Antimicrob Agents Chemother 1995b;39:598-601. [PubMed]
733. Sugar AM, Saunders C, Diamond RD. Successful treatment of Candida osteomyelitis with fluconazole. A noncomparative study of two patients. Diagn Microbiol Infect Dis 1990;13:517-520. [PubMed]
734. Sullivan DJ, Moran GP, Pinjon E, Al-Mosaid A, Stokes C, Vaughan C, Coleman DC. Comparison of the epidemiology, drug resistance mechanisms, and virulence of Candida dubliniensis and Candida albicans. Fems Yeast Res 2004;4:369-376. [PubMed]
735. Sullivan DJ, Westerneng TJ, Haynes KA, Bennett DE, Coleman DC. Candida dubliniensis sp. nov.: phenotypic and molecular characterization of a novel species associated with oral candidosis in HIV-infected individuals. Microbiology 1995;141:1507-1521. [PubMed]
736. Swanson H, Hughes PA, Messer SA, Lepow ML, Pfaller MA. Candida albicans arthritis one year after successful treatment of fungemia in a healthy infant. J Pediatr 1996;129:688-694. [PubMed]
737. Swenson CE, Perkins WR, Roberts P, Ahmad I, Stevens R, Stevens DA, Janoff AW. In vitro and in vivo antifungal activity of amphotericin B lipid complex: Are phospholipases important? Antimicrob Agents Chemother 1998;42:767-771. [PubMed]
738. Tang C. Successful treatment of Candida albicans osteomyelitis with fluconazole. J Infect 1993;26:89-92. [PubMed]
739. Tavanti A, Davidson AD, Gow NAR, Maiden MCJ, Odds FC. Candida orthopsilosis and Candida metapsilosis spp. nov to replace Candida parapsilosis groups II and III. J Clin Microbiol 2005;43:284-292. [PubMed]
740. Telenti A, Steckelberg JM, Stockman L, Edson RS, Roberts GD. Quantitative blood cultures in candidemia. Mayo Clin Proc 1991;66:1120-1123. [PubMed]
741. Thomas MG, Ellis-Pegler RB. Fluconazole treatment of Candida glabrata peritonitis [letter]. J Antimicrob Chemother 1989;24:94-96. [PubMed]
742. Tollemar J, Hockerstedt K, Ericzon BG, Jalanko H, Ringden O. Liposomal amphotericin B prevents invasive fungal infections in liver transplant recipients. A randomized, placebo-controlled study. Transplantation 1995;59:45-50. [PubMed]
743. Tollemar J, Ringden O, Andersson S, Sundberg B, Ljungman P, Tyden G. Randomized double-blind study of liposomal amphotericin B (Ambisome) prophylaxis of invasive fungal infections in bone marrow transplant recipients. Bone Marrow Transplant 1993;12:577-582. [PubMed]
744. Torres HA, Hachem RY, Chemaly RF, Kontoyiannis DP, Raad, II. Posaconazole: a broad-spectrum triazole antifungal. Lancet Infect Dis 2005;5:775-785. [PubMed]
745. Torres HA, Kontoyiannis DP, Rolston KVI. High-dose fluconazole therapy for cancer patients with solid tumors and candidemia: an observational, noncomparative retrospective study. Support Care Cancer 2004;12:511-516. [PubMed]
746. Torres-Rojas JR, Stratton CW, Sanders CV, A HT, Hawley HB, Dascomb HE, Vial LJ. Candida suppurative peripheral thrombophlebitis. Ann Intern Med 1982;96:431-435.[PubMed]
747. Triolo V, Gari-Toussaint M, Casagrande F, Garraffo R, Dageville C, Boutte P, Berard E. Fluconazole therapy for Candida albicans urinary tract infections in infants. Pediat Nephrol 2002;17:550-553. [PubMed]
748. Trnovsky J, Merz W, Della-Latta P, Wu F, Arendrup MC, Stender H. Rapid and accurate identification of Candida albicans isolates by use of PNA FISHFlow. J Clin Microbiol 2008;46:1537-40. [PubMed]
749. Tuil O, Cohen Y. Itraconazole IV solution in the treatment of candidemia in non-neutropenic patients [meeting abstract]. Critical Care 2003;7 (Suppl 2):S63 (Abstract P131). [PubMed]
750. Tunkel AR, Thomas CY, Wispelwey B. Candida prosthetic arthritis: report of a case treated with fluconazole and review of the literature. Am J Med 1993;94:100-103.[PubMed]
751. Ullmann AJ, Lipton JH, Vesole DH, Chandrasekar P, Langston A, Tarantolo SR, Greinix H, Morais de Azevedo W, Reddy V, Boparai N, Pedicone L, Patino H, Durrant S. Posaconazole or fluconazole for prophylaxis in severe graft- versus-host disease. N Engl J Med 2007;356:335-347. [PubMed]
752. Ullmann AJ, Sanz MA, Tramarin A, Barnes RA, Wu WC, Gerlach BA, Krobot KJ, Gerth WC. Prospective study of amphotericin B formulations in immunocompromised patients in 4 European countries. Clin Infect Dis 2006;43:E29-E38. [PubMed]
753. Urbak SF, Degn T. Fluconazole in the treatment of Candida albicans endophthalmitis. Acta Ophthalmologica 1992;70:528-9. [PubMed]
754. Utley JR, Mills J, Roe BB. The role of valve replacement in the treatment of fungal endocarditis. Journal of Thoracic & Cardiovascular Surgery 1975;69:255-8. [PubMed]
755. Uzun O, Ascioglu S, Anaissie EJ, Rex JH. Risk factors and predictors of outcome in patients with cancer and breakthrough candidemia. Clin Infect Dis 2001;32:1713-1717.[PubMed]
756. van Burik JA, Ratanatharathorn V, Stepan DE, Miller CB, Lipton JH, Vesole DH, Bunin N, Wall DA, Hiemenz JW, Satoi Y, Lee JM, Walsh TJ. Micafungin versus fluconazole for prophylaxis against invasive fungal infections during neutropenia in patients undergoing hematopoietic stem cell transplantation. Clin Infect Dis 2004;39:1407-16. [PubMed]
757. van den Anker JN, van Popele NM, Sauer PJ. Antifungal agents in neonatal systemic candidiasis. Antimicrob Agents Chemother 1995;39:1391-1397. [PubMed]
758. van der Merr JWM, Keuning JJ, Scheijgrond HW, Heykants J, van Cutsem J, Brugmans J. The influence of gastric acidity on the bioavailability of ketoconazole. J Antimicrob Chemother 1980;6:552-554. [PubMed]
759. van Deventer AJM, van Vlient HJA, Hop WCJ, Goessens WHF. Diagnostic value of anti-Candida enolase antibodies. J Clin Microbiol 1994;32:17-23. [PubMed]
760. van Deventer AJM, van Vliet HJA, Voogd L, Hop WCJ, Goessens WHF. Increased specificity of antibody detection in surgical patients with invasive candidiasis with cytoplasmic antigens depleted of mannan residues. J Clin Microbiol 1993;31:994-997. [PubMed]
761. Van Peer A, Woestenborghs R, Heykants J, Gasparini R, Gauwenbergh G. The effects of food and dose on the oral systemic availibility of itraconzole in healthy subjects. Eur J Clin Pharmacol 1989;36:423-426. [PubMed]
762. Vanden Bossche H, Marichal P, Gorrens J, Bellens D, Moereels H, Janssen AJ. Mutation in cytochrome P-450-dependent 14a-demethylase results in decreased affinity for azole antifungals. Biochem Soc Trans 1990;18:56-59. [PubMed]
763. Vandewoude K, Vogelaers D, Decruyenaere J, Jaqmin P, De Beule K, Van Peer A, Woestenborghs R, Groen K, Colardyn F. Concentrations in plasma and safety of 7 days of intravenous itraconazole followed by 2 weeks of oral itraconazole solution in patients in intensive care units. Antimicrob Agents Chemother 1997;41:2714-8. [PubMed]
764. Van't Wout JW, Raven EJ, van der Meer JW. Treatment of invasive aspergillosis with itraconazole in a patient with chronic granulomatous disease. J Infect 1990;20:147-150. [PubMed]
765. Vardakas KZ, Samonis G, Michalopoulos A, Soteriades ES, Falagas ME. Antifungal prophylaxis with azoles in high-risk, surgical intensive care unit patients: A meta-analysis of randomized, placebo-controlled trials. Crit Care Med 2006:34(4):1216-24. [PubMed]
766. Vazquez JA, Schranz JA, Clark K, Goldstein BP, Reboli A, Fichtenbaum C. A phase 2, open-label study of the safety and efficacy of intravenous anidulafungin as a treatment for azole-refractory mucosal candidiasis. Jaids 2008;48:304-309. [PubMed]
767. Vazquez JA, Skiest DJ, Nieto L, Northland R, Sanne I, Gogate J, Greaves W, Isaacs R. A multicenter randomized trial evaluating posaconazole versus fluconazole for the treatment of oropharyngeal candidiasis in subjects with HIV/AIDS. Clin Infect Dis 2006a;42:1179-1186. [PubMed]
768. Vazquez JA, Sobel JD. Anidulafungin: A novel echinocandin. Clin Infect Dis 2006b;43:215-222. [PubMed]
769. Vazquez JA, Sobel JD, Peng G, Steele-Moore L, Schuman P, Holloway W, Neaton JD. Evolution of vaginal Candida species recovered from human immunodeficiency virus-infected women receiving fluconazole prophylaxis: The emergence of Candida glabrata? Clin Infect Dis 1999;28:1025-1031. [PubMed]
770. Viale P, Petrosillo N, Signorini L, Puoti M, Carosi G. Should lock therapy always be avoided for central venous catheter-associated fungal bloodstream infections? Clin Infect Dis 2001;33:1947-1948. [PubMed]
771. Villanueva A, Arathoon EG, Gotuzzo E, Berman RS, DiNubile MJ, Sable CA. A randomized double-blind study of caspofungin versus amphotericin for the treatment of candidal esophagitis. Clin Infect Dis 2001;33:1529-1535. [PubMed]
772. Villanueva A, Gotuzzo E, Arathoon E, Noriega LM, Kartsonis NA, Lupinacci RJ, Smietana JM, DiNubile MJ, Sable CA. A randomized double-blind study of caspofungin versus fluconazole for the treatment of esophageal candidiasis. Am J Med 2002;113:294-299. [PubMed]
773. Viscoli C, Castagnola E, Van Lint MT, Moroni C, Garaventa A, Rossi MR, Fanci R, Menichetti F, Caselli D, Giacchino M, Congiu M. Fluconazole versus amphotericin B as empirical antifungal therapy of unexplained fever in granulocytopenic cancer patients: a pragmatic, multicentre, prospective and randomised clinical trial. Eur J Cancer 1996;32A:814-20. [PubMed]
774. Viscoli C, Girmenia C, Marinus A, Collette L, Martino P, Vandercam B, Doyen C, Lebeau B, Spence D, Krcmery V, De Pauw B, Meunier F. Candidemia in cancer patients: A prospective, multicenter surveillance study by the Invasive Fungal Infection Group (IFIG) of the European Organization for Research and Treatment of Cancer (EORTC). Clin Infect Dis 1999;28:1071-1079. [PubMed]
775. Voice RA, Bradley SF, Sangeorzan JA, Kauffman CA. Chronic candidal meningitis: An uncommon manifestation of candidiasis. Clin Infect Dis 1994;19:60-66. [PubMed]
776. Vonk AG, Netea MG, van Krieken JH, Verweij PE, van der Meer JWM, Kullberg BJ. Treatment of intra-abdominal abscesses caused by Candida albicans with antifungal agents and recombinant murine granulocyte colony-stimulating factor. Antimicrob Agents Chemother 2003;47:3688-3693. [PubMed]
777. Voss A, Meis JFGM, Hoogkamp-Korstanje JAA. Fluconazole in the management of fungal urinary tract infections. Infection 1994;4:247-251. [PubMed]
778. Wade J, Schreiber J, Saltzberg D, Bustamante C, Cushing D. Amphotericin B therapy of biopsy-proven Candida esophagitis: A double-blind trial. 31st Interscience Conference on Antimicrobial Agents and Chemotherapy, 1991, Abstract No. 740. [PubMed]
779. Wainer S, Cooper PA, Gouws H, Akierman A. Prospective study of fluconazole therapy in systemic neonatal fungal infection. Pediatric Infectious Disease Journal 1997;16:763-767. [PubMed]
780. Wallbridge DR, McCartney AC, Rrichardson MD. Fluconazole in the treatment of Candida prosthetic valve endocarditis. Mycoses 1993;36:259-261. [PubMed]
781. Walsh T, Whitcomb PO, Ravankar S, Shannon K, Alish S, Pizzo PA. Successful treatment of hepatosplenic candidiasis through repeated episodes of neutropenia. Cancer 1995a;76:2357-2362. [PubMed]
782. Walsh TJ, Adamson PC, Seibel NL, Flynn PM, Neely MN, Schwartz C, Shad A, Kaplan SL, Roden MM, Stone JA, Miller A, Bradshaw SK, Li SX, Sable CA, Kartsonis NA. Pharmacokinetics, safety, and tolerability of caspofungin in children and adolescents. Antimicrob Agents Chemother 2005;49:4536-45. [PubMed]
783. Walsh TJ, Bustamente CI, Vlahov D, Standiford HC. Candidal suppurative peripheral thrombophlebitis: Recognition, prevention, and management. Infect Control 1986a;7:16-22. [PubMed]
784. Walsh TJ, Finberg RW, Arndt C, Hiemenz J, Schwartz C, Bodensteiner D, Pappas P, Seibel N, Greenberg RN, Dummer S, Schuster M, Holcenberg JS. Liposomal amphotericin B for empirical therapy in patients with persistent fever and neutropenia. N Engl J Med 1999;340:764-771. [PubMed]
785. Walsh TJ, Francesconi A, Kasai M, Chanock SJ. PCR and single-strand conformational polymorphism for recognition of medically important opportunistic fungi. J Clin Microbiol 1995b;33:3216-3220. [PubMed]
786. Walsh TJ, Gray W. Candida epiglottitis in immunocompromised patients. Chest 1987;91:482-485. [PubMed]
787. Walsh TJ, Hiemenz J, Pizzo PA. Editorial response: Evolving risk factors for invasive fungal infections--All neutropenic patients are not the same. Clin Infect Dis 1994a;18:793-798. [PubMed]
788. Walsh TJ, Hutchins GM, Bulkley BH, Mendelsohn G. Fungal infections of the heart: an analysis of 51 autopsied patients. Am J Cardiol 1980;45:357-366. [PubMed]
789. Walsh TJ, Lee J, Lecciones J, Rubin M, Butler K, Francis P. Empiric therapy with amphotericin B in febrile granulocytopenic patients. Rev Infect Dis 1991;13:496-503.[PubMed]
790. Walsh TJ, Lee JW, Sien T, Schaufele R, Bacher J, Switchenko AC, Goodman TC, Pizzo PA. Serum D-arabinitol measured by automated quantitative enzymatic assay for detection and therapeutic monitoring of experimental disseminated candidiasis: correlation with tissue concentrations of Candida albicans. J Med Vet Mycol 1994b;32:205-215.[PubMed]
791. Walsh TJ, Merz WG. Pathologic features in the human alimentary tract associated with invasiveness of Candida tropicalis. Am J Clin Path 1986b;85:498-502. [PubMed]
792. Walsh TJ, Merz WG, Lee JW, Schaufele R, Sein T, Whitcomb PO, Ruddel M, Burns W, Wingard JR, Swichenko AC, Goodman T, Pizzo PA. Diagnosis and therapeutic monitoring of invasive candidiasis by rapid enzymatic detection of serum D-arabinitol. Am J Med 1995c;99:164-172. [PubMed]
793. Walsh TJ, Pappas P, Winston DJ, Lazarus HM, Petersen F, Raffalli J, Yanovich S, Stiff P, Greenberg R, Donowitz G, Lee J. Voriconazole compared with liposomal amphotericin B for empirical antifungal therapy in patients with neutropenia and persistent fever. N Engl J Med 2002a;346:225-234. [PubMed]
794. Walsh TJ, Rex JH. All catheter-related candidemia is not the same: Assessment of the balance between the risks and benefits of removal of vascular catheters. Clin Infect Dis 2002b;34:600-602. [PubMed]
795. Walsh TJ, Teppler H, Donowitz GR, Maertens JA, Baden LR, Dmoszynska A, Cornely OA, Bourque MR, Lupinacci RJ, Sable CA, dePauw BE. Caspofungin versus liposomal amphotericin B for empirical antifungal therapy in patients with persistent fever and neutropenia. N Engl J Med 2004;351:1391-1402. [PubMed]
796. Walsh TJ, Whitcomb P, Piscitelli S, Figg WD, Hill S, Chanock SJ, Jarosinski P, Gupta R, Pizzo PA. Safety, tolerance, and pharmacokinetics of amphotericin B lipid complex in children with hepatosplenic candidiasis. Antimicrob Agents Chemother 1997;41:1944-1948. [PubMed]
797. Wang JN, Liu CC, Huang TZ, Huang SS, Wu JM. Laryngeal candidiasis in children. Scand J Infect Dis 1997;29:427-429. [PubMed]
798. Wanger A, Mills K, Nelson PW, Rex JH. Comparison of Etest and National Committee for Clinical Laboratory Standards broth macrodilution method for antifungal susceptibility testing: enhanced ability to detect amphotericin B-resistant Candida isolates. Antimicrob Agents Chemother 1995;39:2520-2522. [PubMed]
799. Webb BC, Thomas CJ, Willcox MD, Harty DW, Knox KW. Candida-associated denture stomatitis. Aetiology and management: a review. Part 1. Factors influencing distribution of Candida species in the oral cavity. Aust Dent J 1998;43:45-50. [PubMed]
800. Weber DJ, Rutala WA, Samsa GP, Wilson MB, Hoffmann KK. Relative frequency of nosocomial pathogens at a university hospital during the decade 1980 to 1989. Am J Infect Control 1992;20:192-197. [PubMed]
801. Weems JJ, Jr. Candida parapsilosis: Epidemiology, pathogenicity, clinical manifestations, and antimicrobial susceptibility. Clin Infect Dis 1992;14:756-766. [PubMed]
802. Weers-Pothoff G, Havermans JF, Kamphuis J, Sinnige HA, Meis JF. Candida tropicalis arthritis in a patient with acute myeloid leukemia successfully treated with fluconazole: case report and review of the literature. Infection 1997;25:109-111. [PubMed]
803. Weigl JA. Candida arthritis in a premature infant treated successfully with oral fluconazole for six months. Ann Acad Med Singapore 2000;29:253-5. [PubMed]
804. Wertz KK, Pretzlaff RK. Caspofungin in a pediatric patient with persistent candidemia. Pediatr Crit Care Med 2004;5:181-3. [PubMed]
805. Wey SB, Mori M, Pfaller MA, Woolson RF, Wenzel RP. Hospital acquired candidemia: The attributable mortality and excess length of stay. Arch Intern Med 1988;148:2642-2645. [PubMed]
806. Whelan WL. The genetic basis of resistance to 5-fluorocytosine in Candida species and Cryptococcus neoformans. Critical Reviews in Microbiology 1987;15:45-56.[PubMed]
807. White MH. Is vulvovaginal candidiasis an AIDS-related illness? Clin Infect Dis 1996;22 Suppl 2:S124-7. [PubMed]
808. White TC, Marr KA, Bowden RA. Clinical, cellular, and molecular factors that contribute to antifungal drug resistance. Clin Microbiol Rev 1998;11:382-402. [PubMed]
809. Wiederhold NP. Attenuation of echinocandin activity at elevated concentrations: a review of the paradoxical effect. Curr Opin Infect Dis 2007;20:574-578. [PubMed]
810. Wilcox CM, Darouiche RO, Laine L, Moskovitz BL, Mallegol I, Wu J. A randomized, double-blind comparison of itraconazole oral solution and fluconazole tables in the treatment of esophageal candidiasis. J Infect Dis 1997;176:227-232. [PubMed]
811. Wilcox M, Nathwani D, Dryden M. Linezolid compared with teicoplanin for the treatment of suspected or proven Gram-positive infections. J Antimicrob Chemother 2004;53:335-344. [PubMed]
812. Wilkin A, Feinberg J. Prophylaxis against fungal infections and cytomegalovirus disease after bone marrow transplantation. Oncology 2000;14:1701-1708. [PubMed]
813. Willems L, van der Geest R, de Beule K. Itraconazole oral solution and intravenous formulations: a review of pharmacokinetics and pharmacodynamics. J Clin Pharm Ther 2001;26:159-169. [PubMed]
814. Wilson AG, Micek ST, Ritchie DJ. A retrospective evaluation of fluconazole for the treatment of Candida glabrata fungemia. Clin Ther 2005a;27:1228-1237. [PubMed]
815. Wilson DA, Joyce MJ, Hall LS, Reller LB, Roberts GD, Hall GS, Alexander BD, Procop GW. Multicenter evaluation of a Candida albicans peptide nucleic acid fluorescent in situ hybridization probe for characterization of yeast isolates from blood cultures. J Clin Microbiol 2005b;43:2909-12. [PubMed]
816. Wilson ML, Davis TE, Mirrett S, Reynolds J, Fuller D, Allen SD, Flint KK, Koontz F, Reller LB. Controlled comparison of the BACTEC high-blood-volume fungal medium, BACTEC plus 26 aerobic blood culture bottle, and 10-milliliter isolator blood culture system for detection of fungemia and bacteremia. J Clin Microbiol 1993;31:865-871.[PubMed]
817. Wingard JR. Importance of Candida species other than C. albicans as pathogens in oncology patients. Clin Infect Dis 1995;20:115-125. [PubMed]
818. Wingard JR, Carter SL, Walsh TJ, Kurtzberg J, Small TN, Gersten ID, Mendizabal AM, Leather H, Confer DL, Baden LR, Maziatz RT, Stadtmauer E, Bolanos-Meade J, Brown J, DiPersio JF, Boeckh M, Marr KA. Results of a randomized, double-blind trial of fluconazole (FLU) vs. voriconazole (VORI) for the prevention of invasive fungal infections (IFI) in 600 allogeneic blood and marrow transplant (BMT) patients. Blood 2007;110:55A-56A. [PubMed]
819. Wingard JR, Dick JD, Merz WG, Sandford GR, Saral R, Burns WH. Pathogenicity of Candida tropicalis and Candida albicans after gastrointestinal inoculation in mice. Infect Immun 1980;29:808-13. [PubMed]
820. Wingard JR, Dick JD, Merz WG, Sandford GR, Saral R, Burns WH. Differences in virulence of clinical isolates of Candida tropicalis and Candida albicans in mice. Infect Immun 1982;37:833-6. [PubMed]
821. Wingard JR, Merz WG, Rinaldi MG, Johnson TR, Karp JE, Saral R. Increase in Candida krusei infection among patients with bone marrow transplantation and neutropenia treated prophylactically with fluconazole. N Engl J Med 1991;325:1274-1277. [PubMed]
822. Wingard JR, Merz WG, Rinaldi MG, Miller CB, Karp JE, Saral R. Association of Torulopsis glabrata infections with fluconazole prophylaxis in neutropenic bone marrow transplant patients. Antimicrob Agents Chemother 1993;37:1847-1849. [PubMed]
823. Wingard JR, Merz WG, Saral R. Candida tropicalis: A major pathogen in immunocompromised patients. Ann Intern Med 1979;91:539-543. [PubMed]
824. Winston DJ, Chandrasekar PH, Lazarus HM, Goodman JL, Silber JL, Horowitz H, Shadduck RK, Rosenfeld CS, Ho WG, Islam MZ, Buell DN. Fluconazole prophylaxis of fungal infections in patients with acute leukemia. Results of a randomized placebo-controlled, double-blind, multicenter trial. Ann Intern Med 1993;118:495-503. [PubMed]
825. Winston DJ, Hathorn JW, Schuster MG, Schiller GJ, Territo MC. A multicenter, randomized trial of fluconazole versus amphotericin B for empiric antifungal therapy of febrile neutropenic patients with cancer. Am J Med 2000;108:282-289. [PubMed]
826. Winston DJ, Maziarz RT, Chandrasekar PH, Lazarus HM, Goldman M, Blumer JL, Leitz GJ, Territo MC. Intravenous and oral itraconazole versus intravenous and oral fluconazole for long-term antifungal prophylaxis in allogeneic hematopoietic stem-cell transplant recipients - A multicenter, randomized trial. Ann Intern Med 2003;138:705-713. [PubMed]
827. Winston DJ, Pakrasi A, Busuttil RW. Prophylactic fluconazole in liver transplant recipients: A randomized, double-blind, placebo-controlled trial. Ann Intern Med 1999;131:729-737. [PubMed]
828. Wise GJ, Goldberg P, Kozinn PJ. Genitourinary candidiasis: Diagnosis and treatment. J Urol 1976;116:778-780. [PubMed]
829. Witt MD, Imhoff T, Li C, Bayer AS. Comparison of fluconazole and amphotericin B for treatment of experimental Candida endocarditis cause by non-C. albicans strains. Antimicrob Agents Chemother 1993;37:2030-2032. [PubMed]
830. Wong-Beringer A, Jacobs RA, Guglielmo BJ. Treatment of funguria. JAMA 1992;267. [PubMed]
831. Wong-Beringer A, Kriengkauykiat J. Systemic antifungal therapy: New options, new challenges. Pharmacotherapy 2003;23:1441-1462. [PubMed]
832. Xu JP, Ramos AR, Vilgalys R, Mitchell TG. Clonal and spontaneous origins of fluconazole resistance in Candida albicans. J Clin Microbiol 2000;38:1214-1220.[PubMed]
833. Yagasaki K, Gando S, Matsuda N, Kameue T, Ishitani T, Hirano T, Iseki K. Pharmacokinetics and the most suitable dosing regimen of fluconazole in critically ill patients receiving continuous hemodiafiltration. Intens Care Med 2003;29:1844-1848. [PubMed]
834. Yap BS, Bodey GP. Oropharyngeal candidiasis treated with a troche form of clotrimazole. Arch Intern Med 1979;139:656-7. [PubMed]
835. Zaas AK, Dodds-Ashley ES, Alexander BD, Johnson MD, Perfect JR. Caspofungin for invasive candidiasis: Experience at DUMC 2001-2004. 44th Interscience Conference on Antimicrobial Agents and Chemotherapy. Washington, DC, 2004, Abstract No. M-1015. [PubMed]
836. Zaoutis T, Walsh TJ. Antifungal therapy for neonatal candidiasis. Curr Opin Infect Dis 2007;20:592-597.[PubMed]
837. Zaoutis TE, Benjamin DK, Steinbach WJ. Antifungal treatment in pediatric patients. Drug Resist Update 2005;8:235-245. [PubMed]
838. Zaruba K, Peters J, Jungbluth H. Successful prophylaxis for fungal peritonitis in patients on continuous ambulatory peritoneal dialysis: Six years experience. Am J Kidney Dis 1991;17:43-46. [PubMed]
839. Zenker PN, Rosenberg EM, Van Dyke RB, Rabalais GP, Daum RS. Successful medical treatment of presumed Candida endocarditis in critically ill infants. J Pediatr 1991;119:472-477. [PubMed]
840. Zhou HH, Goldman M, Wu J, Woestenborghs R, Hassell AE, Lee P, Baruch A, Pesco-Koplowitz L, Borum J, Wheat LJ. A pharmacokinetic study of intravenous itraconazole followed by oral administration of itraconazole capsules in patients with advanced human immunodeficiency virus infection. J Clin Pharmacol 1998;38:593-602.[PubMed]
841. Zingman BS. Resolution of refractory AIDS-related mucosal candidiasis after initation of didanosine plus saquinavir. N Engl J Med 1996;334:1674-1675. [PubMed]
Table 1: Medically significant Candida spp.
| Common Species | Less common Species |
|---|---|
C. albicans C. tropicalis C. glabrata (T. glabrata) C. parapsilosis C. krusei C. lusitaniae |
C. dubliniensis C. famata C. guilliermondii C. haemulonii C. kefyr (C. pseudotropicalis) C. norvegensis C. rugosa C. viswanathii |
While many other species of Candida have been isolated from clinical specimens (380), their significance is unclear. See Eggiman et al. (185) or Pfaller & Diekema (562) for discussions of rarer species. See Sullivan et al. (734) for a specific discussion of C. dubliniensis.
Table 2: Characteristics of the major Candida spp.
| Species | Frequency | Virulence | Clinical Associations |
|---|---|---|---|
C. albicans |
42%-65% |
High |
Most common in all settings |
C. tropicalis |
11%-25% |
High |
Cancer |
C. glabrata |
7%-15% |
Low |
Cancer |
C. parapsilosis |
7%-18% |
Variable |
Plastic devices, hyperalimentation |
C. krusei |
1%-4% |
Low |
Cancer |
C. lusitaniae |
1%-2% |
Low |
Cancer |
Show are frequency estimates for the species causing invasive disease from (4, 223, 497, 609, 614, 817).
Virulence and special clinical associations are discussed and cited in the text.
Table 3: Susceptibility of Candida spp. to antifungal agents
| MIC50 | AmB | FLU | ITRA | VOR | 5FC | ANID | CAS | MIC |
|---|---|---|---|---|---|---|---|---|
C. albicans |
0.5 |
0.5 |
0.12 |
0.03 |
< 0.25 |
0.03 |
0.03 |
0.015 |
C. tropicalis |
0.25 |
1 |
0.06 |
0.06 |
< 0.25 |
0.03 |
0.03 |
0.03 |
C. glabrata |
0.5 |
16 |
0.25 |
0.25 |
< 0.25 |
0.06 |
0.03 |
0.015 |
C. parapsilosis |
0.25 |
1 |
0.12 |
0.03 |
< 0.25 |
2 |
0.5 |
1 |
C. krusei |
0.25 |
64 |
0.5 |
0.5 |
16 |
0.03 |
0.06 |
0.06 |
C. lusitaniae |
> 1 |
2 |
0.25 |
0.03 |
< 0.25 |
0.06 |
0.12 |
0.12 |
Shown are typical species-specific MIC50s (μg/mL) adapted from reports describing collections of clinical isolates (432, 520, 556, 559, 571, 562, 575, 616, 619). MICs were obtained by the NCCLS M27 methodology (488) for all drugs but amphotericin B. As this method fails to detect amphotericin B-resistant Candida (616), the reported amphotericin B MICs were obtained by a more sensitive method based on use of Antibiotic Medium 3 in a agar-based testing format (798).
Table 4: Interpretive breakpoints for antifungal susceptibility testing
| Antifungal Agent | Fluconazole | Itraconazole | Voriconazole | Flucytosine | Echinocandins |
|---|---|---|---|---|---|
Susceptible (S) |
≤ 8 |
≤ 0.125 |
≤ 1 |
≤ 4 |
≤ 2 |
Susceptible-dose dependent (S-DD) |
16-32 |
0.25-0.5 |
2 |
|
|
Intermediate |
|
|
|
8-16 |
|
Resistant (R) |
≥64 |
≥1 |
≥4 |
≥32 |
|
C. albicans |
S |
S |
S |
S |
S |
C. tropicalis |
S |
S |
S |
S |
S |
C. parapsilosis |
S |
S |
S |
S |
S |
C. glabrata |
S-DD to R |
S-DD to R |
S-DD to R |
S |
S |
C. krusei |
R |
R |
S |
R |
S |
C. lusitaniae |
S |
S |
S |
S |
S |
Shown are the breakpoints in μg/mL for Candida isolates against the indicated antifungal agents (130). A disk diffusion-based testing methodology is also available and provides comparable interpretive categories (490). See text for a discussion of the S-DD and I categories. Below this is shown the most common interpretive categories for isolates of the most common species of Candida. Agreed interpretive breakpoints are not available for any of the echinocandins. However, the available data obtained using the above described microdilution methods read at 24h at a partial inhibition endpoint (509) would suggest that wild-type susceptibles isolates of all species have an MIC < 2 micrograms/ml. Essentially all (>99%) current isolates appear susceptible using this interpretive principle. By contrast, isolates from cases of clinical failure have often had MICs > 8 micrograms/ml.
Table 5. Summary of key points for selection of therapy
| Species most likely to have (or develop) reduced susceptibility to… | Frank resistance is usual | Resistance readily develops |
|---|---|---|
…fluconazole |
C. krusei, C. rugosa |
C. glabrata |
…voriconazole |
|
C. krusei, C. rugosa, C. glabrata |
…flucytosine |
C. krusei |
C. albicans |
…amphotericin B |
|
C. lusitaniae, C. glabrata, and C. rugosa |
…an echinocandin |
|
C. parapsilosis and C. guilliermondii |
Combinations in the column labeled “Frank resistance is usual” should be avoided. For the other combinations, successful therapy has been seen but frank resistance has also been shown to develop. Success against isolates with elevated MICs may require use of maximal safe doses. This concept is best document for fluconazole and C. glabrata (see (525, 814) for a good illustrations). It is speculative for other organism-drug combinations but plausible based on best evidence. See text for additional literature support.
Table 6: Therapy for Vaginal Candidiasis: Topical Agents
| Drug | Formulation | Dosage regimen |
|---|---|---|
*Butoconazole |
2% cream |
5 g/d x 3 d |
|
2% cream, slow-release |
5g/d x 1d |
*Clotrimazole |
1% cream |
5 g/d x 7-14 d |
|
100 mg vaginal tablet |
1 tablet/d x 7 d |
|
100 mg vaginal tablet |
2 tablet/d x 3 d |
|
500 mg vg. tab |
1 tablet/d x 1 d |
*Miconazole |
2% cream |
5 g/d x 7 d |
|
100 mg vaginal suppository |
1 suppository x 7 d |
|
200 mg vaginal suppository |
1 suppository/d x 3 d |
|
1200 mg vaginal suppository |
1 suppository/d x 1 d |
Econazole |
150 mg vaginal tablet |
1 tablet/d x 3 d |
Fenticonazole |
2% cream |
5 g/d x 7 d |
*Tioconazole |
2% cream |
5 g/d x 3 d |
|
6.5% cream |
5 g/d x 1 d |
Terconazole |
0.4% cream |
5 g/d x 7 d |
|
0.8% cream |
5 g/d x 3 d |
|
80 mg vaginal suppository |
80 mg/d x 3 d |
Nystatin |
100,000 U vaginal tablet |
1 tablet/d x 14 d |
Table 7: Therapies of choice for Invasive Candidiasisa
C. albicans: Fluconazole
C. tropicalis: Fluconazole
C. parapsilosis: Fluconazole
C. glabrata: An echinocandinb
C. krusei: An echinocandinb (IV); voriconazole (PO)
C. lusitaniae: Fluconazole
Species unknown: An echinocandinb
Neutropenia: An amphotericin B preparation or caspofunginc until neutrophil recovery, then as above.
Febrile neutropenia without proven candidiasis: Caspofunginc
Meningitis: Echinocandins should probably be avoided—see text
Dosages
Amphotericins
1. Amphotericin B deoxycholate (Fungizone): 0.6–0.8 mg/kg/d IV
2. Liposomal amphotericin B (Ambisome): 3 mg/kg/d IV
3. Amphotericin B lipid complex (ABLC, Abelcet): 5 mg/kg/d IV
4. Amphotericin B colloidal dispersion (ABCD, Amphotec): 3-4 mg/kg/d IV (but not recommended due to inferior toxicity profile)
Azoles
5. Fluconazole: Initiate therapy with 800 mg loading dose then 400 mg/day IV. Followup at 400 mg/day PO.
6. Voriconazole: Initiate IV therapy with 6 mg/kg q12h x two doses then 3 mg/kg q12h. Followup therapy is 200 mg q12h PO.
Echinocandins
7. Anidulafungin: 200 mg IV load then 100 mg/day IV
8. Caspofungin: 70 mg IV load then 50 mg/d day IV
9. Micafungin: 100 mg/day IV
aThese guidelines apply principally to candidemia but can in general be extrapolated to renal, urinary, ocular, cardiac, pericardial, suppurative vascular (phlebitis), peritoneal, gallbladder, pancreatic, skeletal (osteomyelitis), joint (arthritis), meningeal, and pulmonary candidiasis. Unfortunately, the amount of data in these other settings is limited and there is usually no obvious best choice of therapy. The only other general guidelines are (a) durable cure of infected devices is very difficult to achieve without device removal (although infection can often be suppressed—see for example the section entitled “Candida Endocarditis, Pericarditis, and Suppurative Phlebitis”) and (b) an agent that penetrates well is needed for protected spaces (the eye and brain—see those sections for details). Helpful anecdotes are found in the chapter sections that discuss individual disease forms.
bThe echinocandins are caspofungin, anidulafungin, and micafungin. These agents appear similar in their efficacy for invasive candidiasis.
cCaspofungin has the most data in neutropenic patients. In particular, it is the only echinocandin as yet studied in febrile neutropenia.
When following these general guidelines, remember also that (a) Candida is not the only yeast to cause invasive fungal infections (be especially alert for cryptococcosis and histoplasmosis), (b) there can be mechanical and pharmacological factors that drive failure or breakthrough (see the section entitled “Persistent and Breakthrough Disease”), and (c) catheters and other potentially infected prosthetic devices usually need to be removed (see sections entitled “Management of Catheters” and “Candida Endocarditis, Pericarditis, and Suppurative Phlebitis”).
What's New?
Colombo AL, et al. Caspofungin Use in Patients with Invasive Candidiasis caused by Common Non-albicans Candida Species: Review of the Caspofungin Database. Antimicrob Agents Chemother 2010;Mar 15 [Epub ahead of print]
Betts RF, Nucci M, et al. A Multicenter, Double-Blind Trial of a High-Dose Caspofungin Treatment Regimen versus a standard Caspofungin Treatment Regimen for Adult Patients with Invasive Candidiasis. Clin Inf Dis. 2009;48:1676-84.
Zaoutis T. et al. A Prospective, Multicenter Study of Caspofungin for the Treatment of Documented Candida or Aspergillus Infections in Pediatric Patients.PEDIATRICS. 2009 Mar;123(3):877-84.
Hamza et al. Single-Dose Fluconazole versus Standard Therapy for Oropharyngeal Candidiasis in HIV-Infected Patients: A Randomized, Double-Blind, Double-Dummy Trial. Clin Infect Dis. 2008 Nov 15;47(10):1270-6.
Legrand F, et al. Adjuvant corticosteroid therapy for chronic disseminated candidiasis. Clin Infect Dis. 2008;46:696-702.
Van Hal et al. Candida dubliniensis Meningitis as Delayed Sequela of Treated C. dubliniensis Fungemia. Emerg Infect Dis. 2008 February; 14(2): 327–329.
Pappas PG, et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis 2007;45:883-893.
Reboli A, Rotstein C, Pappas P, Schranz J, Krause D, Walsh T, Anidulafungin Study Group. Anidulafungin versus fluconazole for invasive candidiasis. N Engl J Med 2007;357(13):1347.
Ruan SY, Lee LN, et al. Candida glabrata fungaemia in intensive care units. Clin Microbiol Infect 2007 Nov 28 [Epub ahead of print]Sun RL, et al. Clinical characteristics and outcome of Candida keratitis. Am J Ophthalmol 2007;143:1043-1045.
Harrington A. Differentiation of Candida albicans from non-albicans yeast directly from blood cultures by Gram stain morphology. Eur J Clin Microbiol Infect Dis 2007;26:325-329.
GUIDED MEDLINE SEARCH FOR:
Review Articles
Espinosa-Aguilar L, Forrest GN. Candidiasis in Solid Organ Transplantation
Singh N, Treatment of opportunistic mycoses: how long is long enough? Lancet Infect Dis 2003;3:703-08
Schaudin C, Stoodley P, Kainovic' A, O'Keeffe T, Costerton B, Robinson D, Baum M, Ehrlich G, Webster P. Bacterial Biofilms, Other Structures Seen as Mainstream Concepts. Microbe 2007;2:231-237.
Adhikari P, Mietzner T. Cell Mediated Immunity. 2008.
Efflux Pumps as a Mechanism of Antimicrobial Resistance. 2008
Raad, I., Hanna, H. and Maki, D. Intravascular Catheter-related Infections: Advances in Diagnosis, Prevention and Management. The LANCET Infectious Diseases 2007; Vol.7, Issue 10, 645-657.
Pappas PG, et al. Clinical Practice Guidelines for the Management of Candidiasis: 2009 Update by the Infectious Diseases Society of America. Clin Infect Dis 2009;48:503-535.
GUIDED MEDLINE SEARCH FOR RECENT REVIEWS
History
Logan McCool: The Discovery and Naming of Candida
Simi Vincent: Origin of the Names of Species of Candida
GUIDED MEDLINE SEARCH FOR HISTORICAL ASPECTS
Table of Contents
- Microbiology
- Epidemiology
- Clinical Manifestation
- Laboratory Diagnosis
- Pathogenesis
- Susceptibility in Vitro and in Vivo
- Antimicrobial Therapy
- General
- Amphotericin B and its Various Lipid-Associated Preparations
- The Azoles
- The Echinocandins
- Flucytosine
- Approaches to Therapy When Susceptibility Testing Data are Unavailable
- Antifungal Dosing in Renal Failure
- Antifungal Dosing for Candida Infections in Pregnancy
- Antifungal Dosing for Candida Infections in Pediatrics
- Specific Situations
- Non-Genital Mucocutaneous Candidiasis
- Genital Candidiasis
- Candidemia and Acute Disseminated Candidiasis
- Presumptive Therapy of Disseminated Candidiasis
- Chronic Disseminated Candidiasis
- Neonatal Candidiasis
- Urinary Candidiasis
- Candida Endophthalmitis
- Candida Endocarditis, Pericarditis, and Suppurative Phlebitis
- Candida Infections of the Peritoneum, Gallbladder, Pancreas
- Candida Osteomyelitis, Arthritis, and Mediastinitis
- Candidal Meningitis
- Candida Pneumonia
- Alternative Therapies
- Endpoints for Monitoring Therapy
- Prophylaxis