
Borrelia species (Relapsing Fever)
Authors: Peter J. Krause, M.D.
Authors, Second Edition: Teshale Seboxa, MD, M.SC (CTM); Daniel Fekade, M.D.
MICROBIOLOGY
Relapsing fever is a group of infections caused by spirochetes in the genus Borrelia that are characterized by recurrent fever and found throughout the world (1, 15, 16, 19, 24, 27, 31, 32, 33, 38, 42, 47, 52,56, 59, 61, 69, 70, 71, 76, 78, 82, 86). These Borrelia are transmitted either by lice (louse-borne relapsing fever or LBRF), soft-bodied ticks (soft tick-borne relapsing fever or STBRF), or hard bodied ticks (hard tick-borne relapsing fever or HTBRF). Distinct febrile episodes are accompanied by non-specific symptoms separated by periods of very mild symptoms or wellness (1, 15, 16, 19, 24, 27, 31, 32, 33, 38, 42, 47,52, 56, 59, 61, 69, 70, 71, 76, 78, 82, 86). Relapse of fever and associated symptoms are caused by cycles of rising spirochetemia and an associated immune response characterized by diminution in the number of spirochetes, immune evasion by a subset of spirochetes, and a resurgence in spirochetemia.
Relapsing fever borrelia are spirochetal bacteria whose spiral shape enhances their motility (Figure 1). They contain a linear chromosome and several linear and circular plasmids. Inner and outer cell membranes are separated by a periplasmic space that contains a bundle of flagella, which are not surface exposed (8, 36, 49, 91). Flagella emerge from each end of the organism and overlap in the middle. They are responsible for shape and motility. The most abundant surface lipoproteins of the outer membrane are variable major proteins (Vmps) that determine serotype identity (4, 5, 68). A change in the expression of variable major proteins enables relapsing fever borrelia to survive in vertebrate hosts and during transmission between a vertebrate host and arthropod vector (5, 68, 77). Alteration in variable major proteins allow escape from adaptive immune attack and sustained spirochetemia in mammalian reservoir hosts that helps perpetuate vector-host transmission (28-36). Relapsing fever borreliarequire nutrients found in the extracellular environment in reservoir hosts and tick vectors to survive. These environments can be recreated using in vitro culture for propagation of Borrelia for research studies.
EPIDEMIOLOGY
Louse-Borne Relapsing Fever
Lice transmit a single species of relapsing fever borrelia (Borrelia recurrentis) from person to person without an intermediate host. Episodic outbreaks of LBRF have been widely reported in Africa, Asia, Europe, and South America (15, 19, 27, 52, 59, 70, 71, 82, 86). Louse-borne relapsing fever has caused massive epidemics in times of war and social disruption. The most recent consisted of an estimated 13 million cases and 5 million deaths in Eastern Europe and Russia between 1919 and 1923 and more than a million cases and 50,000 thousand deaths in Europe and North Africa during World War II (52, 82). Louse-borne relapsing fever is currently endemic only in Eritrea, Ethiopia, Somalia, and Sudan (15, 27, 59, 70, 71, 86).
Soft Tick-Borne Relapsing Fever
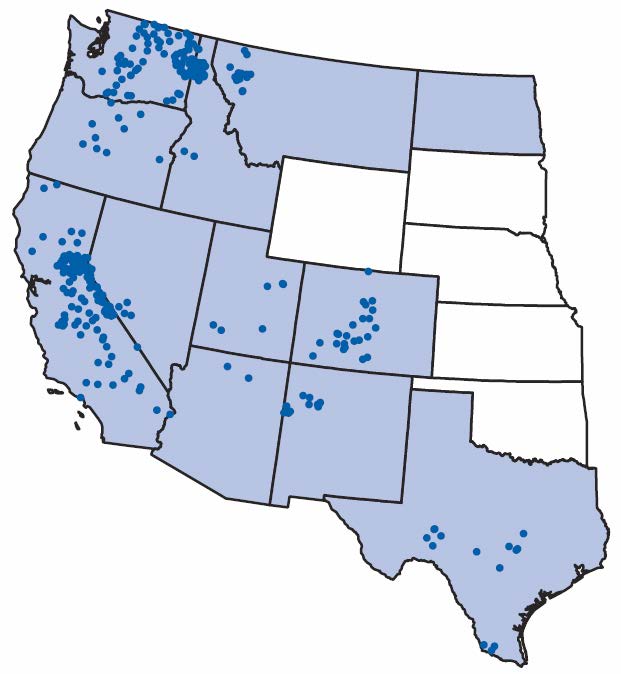
Soft bodied ticks (Argasidae) transmit several species of Borrelia including Borrelia hermsii and Borrelia turicatae in the US, Borrelia duttonii and Borrelia crocidurae in sub Saharan Africa, and Borrelia persica, Borrelia latyshevi, and Borrelia hispanica in Asia, Africa, and the Middle East (1, 16, 24, 31, 32, 33, 38, 47, 59, 61, 76, 78). These Borrelia are maintained in rodents and other mammals, including domestic farm animals. Birds also might serve as reservoir hosts. Transovarial transmission from female adults to their eggs allows survival of the Borrelia when reservoir hosts are scarce. Soft ticks feed for less than an hour, usually at night when people are asleep, and are almost never detected. Soft tick-borne relapsing fever is widespread and is found in North, Central and South America and in Africa, Asia, and Europe. STBRF cases have a focal distribution in the United States and occur throughout western North America and northern Mexico (Figure 2) (16, 31, 32, 38, 47, 78).Borrelia hermsii cases are predominantly associated with staying overnight in rustic cabins or other habitats where rodents have gotten into the walls or ceilings, rather than from camping in tents in the outdoors. B. turicatae is found primarily in the southwestern and south-central United States in desert or plains environments. Most cases are acquired from entering caves or sleeping in caves.
{kind=link}
Hard Tick-Borne Relapsing Fever
Hard-bodied ticks transmit the relapsing fever spirochete Borrelia miyamotoi (1, 3, 23, 25, 30, 34, 40, 42, 43, 44, 48, 50, 56, 57, 63, 69, 73, 74, 75, 80, 83, 85). These same tick species also transmit Borrelia burgdorferi (the Lyme disease agent) and several other pathogens including Babesia microti and human granulocytic anaplasmosis. B. miyamotoi has been found in Ixodes scapularis in the northeastern and midwestern United States, Ixodes pacificus in the western United States, Ixodes ricinus in Europe, and Ixodes ovatus, Ixodes pavlovskyi, and Ixodes persulcatus in Asia. Human cases were first described in Russia in 2011 but have since been described in the United States, Europe, and Japan , (23, 42, 48, 56, 57, 69, 75). Ixodes ticks feed over the course of several days, usually in the daytime, and are more easily detected than soft bodied ticks.
![]()
CLINICAL MANIFESTATIONS
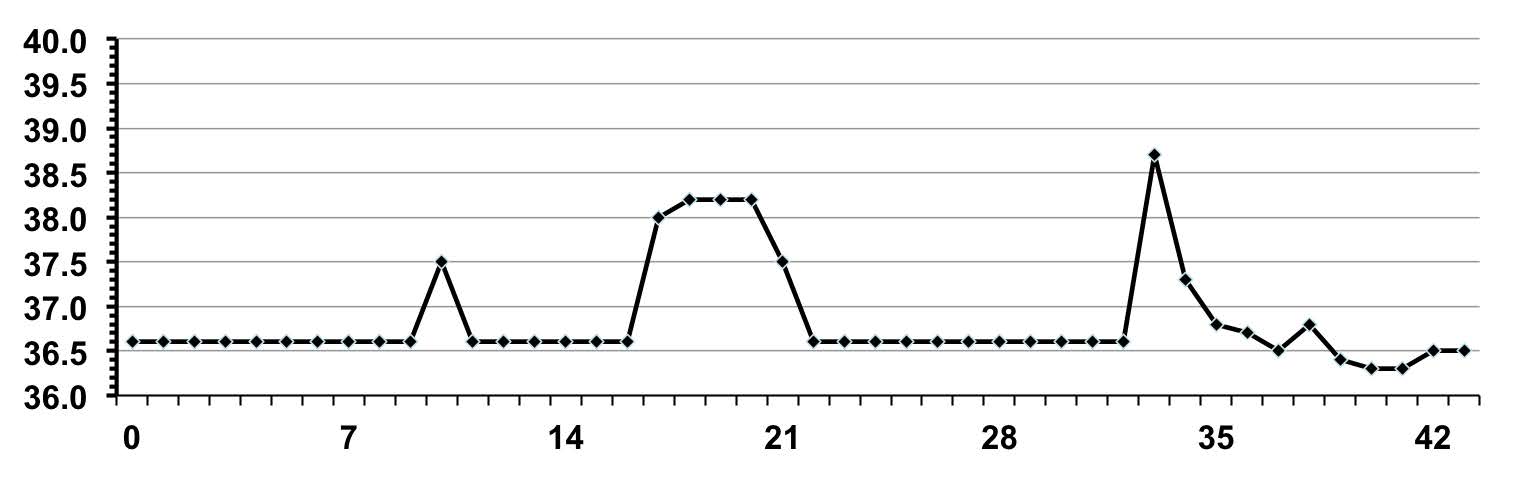
The term “relapsing fever” denotes the clinical manifestation that distinguish louse-born relapsing fever (LBRF), soft tick-borne relapsing fever (STBRF), and hard-tick borne relapsing fever (HTBRF) from most other infectious diseases, namely episodes of high fever separated by periods of wellness (Figure 3). Up to 10 relapses may occur over several weeks or months if the diagnosis is missed and no antibiotic therapy is given (27, 32, 59, 69, 78). Alternatively, there may be only one relapse or no relapse in some patients, especially with LBRF and HTBRF. In the initial report of human B. miyamotoi infection where the diagnosis was confirmed in 46 patients with febrile illness, only five experienced relapsing fever (69). It is possible that a greater number of these patients would have developed fever relapse had they not been treated early in the course of illness with antibiotics. In other respects, the clinical presentation of relapsing fever is highly variable. Although most patients experience a viral-like illness, some may have gastrointestinal symptoms and a few may develop central nervous system symptoms such as meningoencephalitis (22, 32, 42, 48, 52, 59). The characteristic recurring episodes of fever are accompanied by non-specific symptoms, including headache, shaking chills, myalgia, arthralgia, and abdominal distress that last from 3 to 5 days with relapses that occur after 5 to 14 days of apparent recovery (Table 1) (1,16, 19, 24, 27, 31, 32, 33, 38, 42, 47, 52, 56, 59, 61, 69, 71, 78, 82). In the original case series of hard-tick borne relapsing fever, 10% of patients presented with an erythema migrans rash (69). It is unclear whether the erythema migrans rash was due to coinfecting Lyme borreliosis or to B. miyamotoi, although no other relapsing fever Borrelia have been shown to cause erythema migrans. B. miyamotoi and B. burgdorferi coinfection have been documented in reports from the United States and Japan (56, 75). B. burgdorferi and Babesia microti coinfection or B. burgdorferi and Anaplasma phagocytophilumcoinfection cause more severe acute disease than B. burgdorferi infection alone (11, 55, 58). Further studies are needed to determine whether B. miyamotoi and B. burgdorferi coinfection increases relapsing fever disease severity.
{kind=link}
Louse-born relapsing fever, soft tick-borne relapsing fever, and hard-tick borne relapsing fever borrelia infections are associated with a variety of possible complications because these pathogens can invade many different tissues and cause inflammation. Neurologic impairment is one of the most common complications of relapsing fever (22, 36, 42, 48, 52). Both the central and peripheral nervous systems may be involved. Meningitis or meningoencephalitis are a result of direct invasion of the cerebrospinal fluid and brain tissue. Patients may have an acute episode of meningitis or a progressive deterioration in consciousness. Cranial neuritis may occur, especially the seventh or eighth cranial nerves that result in Bells’ palsy and decreased hearing. Infection and inflammation of the anterior portion of the eye (iridocyclitis) or more generalized eye involvement (panoptholmitis) have been reported (22). Involvement of the nerves of the spinal cord (radiculopathy or myelitis) may occur. Cardiac manifestations of relapsing fever include myocarditis and cardiomegaly. Pulmonary complications consist of pneumonia and pulmonary edema. Hepatic impairment may result in hepatitis and hepatomegaly and can proceed to liver failure. Bleeding may occur with epistaxis, petechiae, and ecchymosis due to thrombocytopenia, decreased clotting factors, or capillary obstruction by aggregation of Borrelia. Louse-born relapsing fever and soft tick-borne relapsing fever can be especially severe during pregnancy, resulting in abortion, stillbirth, and/or neonatal infection (17, 39, 57, 60, 87).
Relapsing fever may cause death and is most commonly associated with LBRF. Fatality rates may exceed 40% in large epidemics among nutritionally and immunosuppressed populations during war or famine (19, 37, 59, 82). In contrast, the fatality rate of STBRF is 5% or less (31).
![]()
LABORATORY DIAGNOSIS
The diagnosis of relapsing fever should be considered in any patient who develops a febrile illness, especially if recurrent; lives or travels in an endemic area; and/or has had recent exposure to body lice or soft-bodied or hard-bodied (Ixodes) ticks. Confirmation of the diagnosis can be made by identification of Borrelia on thin blood or CSF smear, amplification of relapsing fever Borrelia DNA using polymerase chain reaction (PCR), inoculation of blood into immunodeficient mice with subsequent identification of the organism as outlined above, or a four-fold rise in specific antibody in acute and convalescent sera (37, 42, 56, 57, 69, 75, 91). Giemsa or Wright stained thick or thin blood smears are most likely to be positive during a febrile episode. Amplification and identification of relapsing fever Borrelia DNA using PCR in blood or CSF samples is at least equal to or often more sensitive and specific than smear, however, PCR is less available, less rapid, and more labor intensive to perform than smear. The most reliable antibody test currently available is that based on B. miyamotoi GLPQ antigen (56, 79). Like PCR, animal inoculation and antibody testing are not yet widely available.
PATHOGENESIS
Relapsing fever borrelia are transmitted by lice or ticks but also can be transmitted across the placenta or transmitted through accidental contact with infected blood. At least one case each of blood transfusion transmission with B. recurrentis and B. duttoni have been reported (46, 89). A recent study in mice suggests that B. miyamotoi also may be transmitted through blood transfusion (54).
Following initial transmission and proliferation of relapsing fever borrelia in the blood, antibody and other immune factors greatly decrease spirochetemia. A few remaining Borrelia are able to alter certain surface variable membrane lipoproteins, evade immune attack, and begin to proliferate. The new variant (serotype) elicits an altered immune response and the recrudescence of symptoms (4, 5, 6, 7, 65, 72). A single strain of B. hermsii can produce up to 40 anitigenically distinct variable small (Vsp) and large (Vlp) membrane proteins. Certain strain variants are more efficient in their ability to invade neural tissue.
SUSCEPTIBIILTY IN VITRO AND IN VIVO
Relapsing fever Borrelia are microaerophilic and can be cultivated in cell free media but have complex nutritional requirements for growth (8, 91). In general, relapsing fever Borrelia are very susceptible to tetracyclines and penicillins and most cephalosporins and less susceptible to macrolids. Minimum inhibitory concentrations of penicillin and tetracycline for Borrelia spp. generally are less than 0.1 µg/ml (2,9). B. recurrentis was cultivated in the laboratory for the first time in 1997 and was found to be highly susceptible to tetracycline (MIC and MBC 0.006µg/ml); penicillin (MIC 0.2µg/ml and MBC 0.75µg/ml); and erythromycin (MIC 0.04µg/ml and MBC < 0.02µg/ml). The recently discovered B. miyamotoi has been cultured in vitro from isolates in Japan and the United States but information about in vitroantimicrobial susceptibility is not yet available.
![]()
ANTIMICROBIAL THERAPY
Doxycycline/tetracycline, penicillin, most cephalosporins, and erythromycin are effective for the treatment of relapsing fevers (10, 13, 14, 21, 28, 29, 41, 53, 62, 66, 67, 81). Borrelia species are susceptible tochloramphenicol and vancomycin but side effects of chloramphenicol and the poor CNS penetration of vancomycin limit their use. Azithromycin is likely to be effective but therapeutic trials have not been carried out. Borrelia species are not susceptible to rifampin, metronidazole and sulfa drugs, and are relatively resistant to most quinolones and aminoglycosides.
For louse-borne relapsing fever, single dose doxycycline (100 mg) or tetracycline (500 mg), or erythromycin stearate or ethyl succinate (500 mg), by mouth provide effective therapy and clear spirochetes from the circulation in 2-4 hrs (Table 2) (21, 62, 67). Doxycyclines/tetracyclines are preferred but should not be used in pregnant and nursing women and in children less than 9 years old. For all children, erythromycin (12.5 mg/kg up to 500 mg) by mouth is effective. For children older than 8 years old, doxycycline (2 mg/kg up to 100 mg) or tetracycline (12.5 mg/kg up to 500 mg) can be used. If oral therapy cannot be given, parenteral treatment with intramuscular penicillin G procaine (600,000-800,000 units for adults and 400,000 units for children) can be given. The overall recurrence rate is less than 5% following antimicrobial therapy.
For soft tick-borne relapsing fever or hard tick-borne relapsing fever, doxycycline or tetracycline given for 7 to 10 days are preferred treatments for patients who are non-pregnant, non-lactating, and older than 9 years. Although single dose therapy can be used (100 mg doxycycline or 500 mg tetracycline), there is some evidence that the recurrence rate may be unacceptably high for soft tick-borne relapsing fever (32, 47, 82). Doxycycline (100 mg or 4 mg/kg) twice daily or tetracycline (500 mg or 12.5 mg/kg) every 6 hours are given by mouth. Erythromycin (500 mg or 12.5 mg/kg) given orally every 6 hours is an alternative choice. For children less than 8 years of age, erythromycin is the drug of choice. For patients experiencing central nervous system involvement, parenteral beta-lactam antibiotics are administered. Patients with meningoencephalitis due to B. miyamotoi were successfully treated either with intravenous penicillin G 24 million units daily for 30 days of ceftriaxone 2 grams per day for 2 weeks (42, 48).
Physicians need to be aware of the potential for a Jarisch-Herxheimer reaction when treating patients for relapsing fever because it occurs in 80-90% of patients with louse-borne relapsing fever and 30-40% of patients with soft tick-borne relapsing fever, and can be life-threatening or fatal in some cases. Patients with this reaction experience an acute exacerbation of symptoms within 1 to 2 hours following the first dose of antibiotic (12, 18, 20, 26, 35, 64, 84, 88, 90). These include fever and chills followed by drenching sweats, hypotension, and exhaustion. It is thought that large numbers of bacteria are abruptly fragmented and killed with antibiotic therapy, exposing lipoprotein antigen that bind to macrophages and other cytokine producing cells, which in turn elicit an intense cytokine response. Circulating levels of tumor necrosis factor, interleukin-6 and interleukin-8 were increased by six and four fold, respectively from admission levels in patients with the Jarisch-Herxheimer reaction and there was a correlation between peak cytokine concentrations and the severity of the reaction (64). Most reactions are self-limited and can be managed using supportive therapy that consists of bed rest, antipyretics, and volume expansion for hypotension. Measures to kill Borrelia gradually will decrease the severity of the reaction, although they may prolong symptoms. The use of penicillin in low dose is less likely to rapidly kill Borrelia than tetracyclines and results in less severe but more prolonged symptoms (20, 90). Treatment to block the reaction is more problematic. Meptazinol is an opiod with agonist properties that has been shown to lessen the severity of the reaction in louse-borne relapsing fever but the drug is not available in the United States (84). Pretreatment with sheep anti–tumor necrosis factor (TNF), Fab antibody fragments suppresses Jarisch-Herxheimer reactions in louse-borne relapsing fever patients (35). Corticosteroids do not work very well, although prednisone and prednisolone have shown some beneficial effects in patients experiencing the reactions associated with treatment for syphilis (12). Regardless of the management approach, patients who experience evidence of this reaction should be monitored closely for the first 12 hours after the initial dose of antibiotic in the emergency room or hospital with IV access in place.
![]()
ENDPOINTS FOR MONITORING THERAPY
Mortality rates for LBRF range from 10-70% and for STBRF range from 4-10% without treatment. These rates decrease with treatment to 2-5% and less than 2%, respectively (32, 59). Spirochetes usually are cleared from the circulation by 24 hours following administration of antibiotics. Relapsing fever patients who are immunocompromised and those with CNS, cardiac, pulmonary or liver complications have a poorer prognosis and need to be followed more closely and for a longer duration.
VACCINES
There are no vaccines available for relapsing fever.
PREVENTION
Preventive measures for louse-borne relapsing fever include avoiding contact with human body lice, good personal hygiene, delousing procedures, cutting hair short, laundering clothing and bedding material at 60°C with soap followed by ironing, and applying residual insecticides to clothing and bedding.
Preventive measures for soft tick-borne relapsing fever include rodent-proof construction for dwellings in endemic areas. For unsatisfactory dwellings, removal of rodent nesting materials and liberal spraying of insecticides are useful. People traveling in endemic areas should be advised to avoid cabins or caves and natural areas inhabited by ticks and rodents and should use tick repellents. Sleeping on the floor or in a bed adjacent to walls should be avoided. People who are bitten by a soft-bodied tick in an area that is endemic for soft tick-borne relapsing fever may be protected if they take prophylactic antibiotic within 2 days of the exposure. For non-pregnant individuals over 9 years of age, doxycycline (200 mg orally the first day and then 100 mg a day for four days) or tetracycline (500 mg orally four times daily for 3 days) will decrease the risk of infection (45).
![]()
REFERENCES
1. Barbour A. Phylogeny of a relapsing fever Borrelia species transmitted by the hard tick Ixodes scapularis. Infect Genet Evol. 2014;27:551–558. [PubMed]
2. Barbour AG. Laboratory aspects of Lyme borreliosis. Clin Microbiol Rev 1988;1:399-414. [PubMed]
3. Barbour AG, Bunikis J, Travinsky B, Hoen AG, Diuk-Wasser MA, Fish D, Tsao JI. Niche partitioning of Borrelia burgdorferi and Borrelia miyamotoi in the same tick vector and mammalian reservoir species. Amer J Trop Med Hyg 2009;81:1120-1131. [PubMed]
4. Barbour AG, Barrera O, Judd RC. Structural analysis of the variable major proteins of Borrelia hermsii. J Exp Med 1983; 158:2127-2140. [PubMed]
5. Barbour AG, Carter CJ, Burman N, Freitag CS, Garon CF, Bergström S. Tandem insertion sequence–like elements define the expression site for variable antigen genes of Borrelia hermsii. Infect Immun 1991;59:390-397. [PubMed]
6. Barbour AG, Carter CJ, Sohaskey CD. Surface protein variation by expression site switching in the relapsing fever agent Borrelia hermsii. Infect Immun 2000; 68:7114-7121. [PubMed]
7. Barbour AG, Dai Q, Restrepo BI, Stoenner HG, Frank SA. Pathogen escape from host immunity by a genome program for antigenic variation. Proc Natl Acad Sci. 2006;103:18290-18295. [PubMed]
8. Barbour AG, Hayes SF. Biology of Borrelia species. Microbiol Rev 1986;50:381-400. [PubMed]
9. Barbour AG, Todd WJ and Stoenner HG. Action of penicillin on Borrelia hermsii. Antimicrob Agents Chemother 1982;21:823-829. [PubMed]
10. Barclay AJ, Coulter JB. Tick-borne relapsing fever in central Tanzania. Trans R Soc Trop Med Hyg 1990; 84:852-856. [PubMed]
11. Belongia EA, Reed KD, Mitchell PD, Chyou PH, Mueller-Rizner N, Finkel MF, Schriefer ME. Clinical and epidemiological features of early Lyme disease and human granulocytic ehrlichiosis in Wisconsin. Clin Infect Dis 1999;29:1472–1477. [PubMed]
12. Belum GR, Belum VR,Arudra SKC, Reddy BSN. The Jarisch-Herxheimer reaction: Revisited. Travel Medicine and Infectious Disease 2013;11:231-237. [PubMed]
13. Borgnolo G, Hailu B, Ciancarelli A, Almaviva M, Woldemariam T. Louse-borne relapsing fever. Trop Geogr Med 1993;45:66-69. [PubMed]
14. Borgnolo G, Denku B, Chiabrera F, Hailu B. Louse-borne relapsing fever in Ethiopian children: a clinical study. Ann Trop Paediatr 1993;13:165-171. [PubMed]
15. Boutellis A, Mediannikov O, Bilcha KD, Ali J, Campelo D, Barker SC, Raoult D. Borrelia recurrentis in head lice, Ethiopia. Emerg Infect Dis. 2013;19:796-8. [PubMed]
16. Boyer KM, Munford RS, Maupin GO, Pattison CP, Fox MD, Barnes AM, Jones WL, Maynard JE. Tick-borne relapsing fever: an interstate outbreak originating at Grand Canyon National Park. Am J Epidemiol.1977;105:469-479. [PubMed]
17. Brasseur D. Tick-borne relapsing fever in a premature infant. Ann Trop Paediatr 1985;5:161-162. [PubMed]
18. Bryceson AD, Parry EH, Perine PL, Warrell DA, Vukotich D, Leithead CS. Louse-borne relapsing fever: a clinical and laboratory study of 62 cases in Ethiopia and a reconsideration of the literature. Q J Med 1970;39:129-70. [PubMed]
19. Bryceson ADM. Clinical pathology of the Jarisch-Herxheimer reaction. J Infect Dis 1976;133:696-704. [PubMed]
20. Butler T. Relapsing fever: New lessons about antibiotic action. Ann Intern Med 1985; 102:397-399. [PubMed]
21. Butler T, Jones PK, Wallace CK. Borrelia recurrentis infection: single dose antibiotic regimens and management of the Jarisch-Herxheimer reaction. J Infect Dis 1978;137:573-577. [PubMed]
22. Cadavid D, Barbour AG. Neuroborreliosis during relapsing fever: review of the clinical manifestations, pathology, and treatment of infections in humans and experimental animals. Clin Infect Dis. 1998;26:151-164. [PubMed]
23. Chowdri HR, MD; Gugliotta JL, Berardi VP, Goethert HK, ScD, Molloy PJ, Sterling SL, Telford SL III. Borrelia miyamotoi infection presenting as human granulocytic anaplasmosis: a case report. Ann Intern Med 2013;159:217. [PubMed]
24. Christensen J, Fischer RJ, McCoy BN, Raffel SJ, Schwan TG. Tickborne relapsing Fever, bitterroot valley, Montana, USA. Emerg Infect Dis. 2015;21:217-23. [PubMed]
25. Cosson JF, Michelet L, Chotte J, Le Naour E, Cote M, Devillers E, Poulle ML, Huet D, Galan M, Geller J, Moutailler S, Vayssier-Taussat M. Genetic characterization of the human relapsing fever spirocheteBorrelia miyamotoi in vectors and animal reservoirs of Lyme disease spirochetes in France. Parasit Vectors 2014;7:233. [PubMed]
26. Coxon RE, Fekade D, Knox K, Melka A, Daniel A. Griffin GE, Warrell DA. The effect of polyclonal antibody fragments to tumour necrosis factor on the cytokine response during the Jarish-Herxheimer reaction of louse borne relapsing fever. Q J Med 1997;90:213-221. [PubMed]
27. Cutler SJ, Abdissa A, Trape JF. New concepts for the old challenge of African relapsing fever borreliosis. Clin Microbiol Infect. 2009;15:400-406. [PubMed]
28. Daniel E, Beyene H, Tessema T. Relapsing fever in children- demographic, social and clinical features. Ethiop Med J 1992;30:207-214. [PubMed]
29. de Pierpont E, Goubau P, Verhaegen J, Vandepitte J. Single dose minocycline and doxycycline treatment of tick borne relapsing fever: a double blind clinical trial in Rwanda. Ann Soc Belge Med Trop 1983;63:357-361. [PubMed]
30. Dibernardo A, Cote T, Ogden NH, Lindsay LR. The prevalence of Borrelia miyamotoi infection, and co-infections with other Borreliaspp. in Ixodes scapularis ticks collected in Canada. Parasit Vectors. 2014;15:183. [PubMed]
31. Dworkin MS, Anderson DE, Schwan TG, Shoemaker PC, Banerjee SN, Kassen BO, Burgdorfer W. Tick-borne relapsing fever in the northwestern United States and southwestern Canada. Clin Infect Dis 1998,26:122-131. [PubMed]
32. Dworkin MS, Schwan TG, Anderson DE, Borchardt SM. Tick-borne relapsing fever. Infect Dis N Amer 2008;22:449-468. [PubMed]
33. Edall TA, Emerson JK, Maupin GO, et al. Tick-borne relapsing fever in Colorado: Historical review and report of cases. JAMA 1979;241:2279-2282. [PubMed]
34. Eshoo MW, Crowder CD, Carolan HE, Rounds MA, Ecker DJ, Haag H, Mothes B, Nolte O. Broad-range survey of tick-borne pathogens in Southern Germany reveals a high prevalence of Babesia microti and a diversity of other tick-borne pathogens. Vector Borne Zoonotic Dis 2014;14:584-591. [PubMed]
35. Fekade D, Knox K, Hussein K, Melka A, Daniel A, Griffin GG, Warrell DA. Prevention of Jarisch-Herxheimer reactions by treatment with antibodies against tumor necrosis factor TNF. N Engl J Med 1996;335:311-315. [PubMed]
36. Felsenfeld O. Borrelia, human relapsing fever, and parasite-vector-host relationships. Bacteriol Rev 1965;29:46-74. [PubMed]
37. Felsenfeld O. Borrelia: Strains, Vectors, Human and Animal Borreliosis. St. Louis, Warren H. Green, 1971.
38. Forrester JD, Kjemtrup AM, Fritz CL, Marsden-Haug N, Nichols JB, Tengelsen LA, Sowadsky R, DeBess E, Cieslak PR, Weiss J, Evert N, Ettestad P, Smelser C, Iralu J, Nett RJ, Mosher E, Baker JS, Houten CV, Thorp E, Geissler AL, Kugeler K, Mead P. Tickborne relapsing Fever - United States, 1990-2011. MMWR Morb Mortal Wkly Rep. 2015;64:58-60. [PubMed]
39. Fuchs PC, Oyama AA. Neonatal relapsing fever due to transplacental transmission of Borrelia. JAMA 1969;208:690-692. [PubMed]
40. Fukunaga M, Takahashi Y, Tsuruta Y, Matsushita O, Ralph D, McClelland M, Nakao M. Genetic and phenotypic analysis of Borrelia miyamotoi sp. nov., isolated from the ixodid tick Ixodes persulcatus, the vector for Lyme disease in Japan. Internat J System Bacteriol 1995;45:804-810. [PubMed]
41. Gebrehiwot T, Fiseha A. Tertracycline versus penicillin in the treatment of louse-borne relapsing fever. Ethiop Med J 1992;30:175-178. [PubMed]
42. Gugliotta JL, Goethert HK, Berardi VP, Telford SR, 3rd. Meningoencephalitis from Borrelia miyamotoi in an immunocompromised patient. New Engl J Med. 2013;368:240-245. [PubMed]
43. Hamer SA, Hickling GJ, Keith R, Sidge JL, Edward D Walker ED, Tsao J. Associations of passerine birds, rabbits, and ticks with Borrelia miyamotoi and Borrelia andersonii in Michigan, U.S.A. Parasites & Vectors 2012;5:231. [PubMed]
44. Hansford KM, Fonville M, Jahfari S, Sprong H, Medlock JM. Borrelia miyamotoi in host-seeking Ixodes ricinus ticks in England. Epidemiol Infect 2014;14:1-9. [PubMed]
45. Hasin T, Davidovitch N, Cohen R, Dagan T, Romem A, Orr N, Klement E, Lubezky N, Kayouf R, Sela T, Keller N, Derazne E, Halperin T, Yavzori M, Grotto I, Cohen D. Postexposure treatment with doxycycline for the prevention of tick-borne relapsing fever. N Engl J Med 2006;355:148-155. [PubMed]
![]()
46. Hira PR, Husein SF. Some transfusion-induced parasitic infections in Zambia. J Hyg Epidemiol Microbiol Immunol 1979;23:436-444. [PubMed]
47. Horton JM, Blaser MJ. The spectrum of relapsing fever in the Rocky Mountains. Arch Intern Med 1985;145:871-875. [PubMed]
48. Hovius JW, de Wever B, Sohne M, Brouwer MC, Coumou J, Wagemakers A, Oei A, Knol H, Narasimhan S, Hodiamont CJ, Jahfari S, Pals ST, Horlings HM, Fikrig E, Sprong H, Oers MHJ. A case of meningoencephalitis by the relapsing fever spirochaete Borrelia miyamotoi in Europe. Lancet 2013;382:658. [PubMed]
49. Hyde FW, Johnson RC. Genetic relationship of Lyme disease spirochetes to Borrelia, Treponema, and Leptospira spp. J Clin Microbiol 1984;20:151-154. [PubMed]
50. Jahfari S, Herremans T, Platonov AE, Kuiper H, Karan LS, Vasilieva O, Koopmans MPG, Hovius JWR, Sprong H. High seroprevalence of Borrelia miyamotoi antibodies in forestry workers and individuals suspected of human granulocytic anaplasmosis in the Netherlands. New Microbes New Infect 2014;2:144-149. [PubMed]
51. Jongen VH, van Roosmalen J, Tiems J, Van Holten J, Wetsteyn JC. Tick-borne relapsing fever and pregnancy outcome in rural Tanzania. Acta Obstet Gynecol Scand 1997;76:834-838. [PubMed]
52. Judge DM, Samuel I, Perine PL, Vukotic D, Ababa A. Louse-borne relapsing fever in man. Arch Pathol 1974;97:136-140. [PubMed]
53. Kazragis RJ, Dever LL, Jorgensen JH, Barbour AG. In vivo activities of ceftriaxone and vancomycin against Borrelia spp. in the mouse brain and other sites. Antimicrob Agents Chemother. 1996;40:2632-2636. [PubMed]
54. Krause PJ, Hendrickson J, Steeves T, Fish D. Blood transfusion transmission ofthe tick-borne relapsing fever spirochete Borrelia miyamotoi in mice, Transfusion 2014. [Epub ahead of pub] [PubMed]
55. Krause PJ, McKay K, Thompson CA, Sikand VK, Lentz R, Lepore T, Closter L, Christianson D, Telford SR, Persing D, Radolf, JD Spielman A and the deer-associated infection study group. Disease-specific diagnosis of coinfecting tick-borne zoonoses: Babesiosis, human granulocytic ehrlichiosis and Lyme disease. Clin Infect Dis 2002;34:1184-1191. [PubMed]
56. Krause PJ, Narasimhan S, Wormser GP, Barbour AG, Platonov AE, Brancato J, Lepore T, Dardick K, Mamula M, Rollend L, Steeves TK, Diuk-Wasser M, Usmani-Brown S, Williamson P, Sarksyan DS, Fikrig E, Fish D. Borrelia miyamotoi sensu lato seroreactivity and seroprevalence in the northeastern United States. Emerg Infect Dis 2014; 20:1183-1190. [PubMed]
57. Krause PJ, Narasimhan S, Wormser GP, Rollend L, Fikrig E, Lepore T, Barbour A, Fish D. Human Borrelia miyamotoi Infection in the United States. New Engl J Med 2013;368:291-293. [PubMed]
58. Krause PJ, Telford S, Spielman A, Sikand VJ, Ryan R, Christianson D, Burke G, Brassard P, Pollack R, Peck J, Persing DH. Concurrent Lyme disease and babesiosis: Evidence for increased severity and duration of illness. JAMA1996;275:1657-1660. [PubMed]
59. Larsson C, Andersson M, Bergström S. Current issues in relapsing fever. Curr Opin Infect Dis. 2009;22:443-449. [PubMed]
60. Larsson C, Andersson M, Guo BP, Nordstrand A, Hagerstrand I, Carlsson S, Bergstrom S. Complications of pregnancy and transplacental transmission of relapsing-fever borreliosis. J Infect Dis.2006;194:1367-74. [PubMed]
61. Le CT. Tick-borne relapsing fever in children. Pediatrics 1980;66:963-966. [PubMed]
62. Mekasha A. Louse borne relapsing fever in children. J Trop Med Hyg 1992;95:206-209. [PubMed]
63. Mun J, Eisen RJ, Eisen L, Lane RS. Detection of a Borrelia miyamotoi sensu lato relapsing-fever group spirochete from Ixodes pacificus in California. J Med Entomol 2006;43:120-123. [PubMed]
64. Negussie Y, Remick DG, DeForge LE, Kunkel SL, Eynon A, Griffin GE. Detection of plasma tumor necrosis factor, interleukins 6 and 8 during the Jarisch-Herxheimer reaction of relapsing fever. J Exp Med 1992;175:1207-1212. [PubMed]
65. Norris SJ. Antigenic variation with a twist—the Borrelia story. Mol Microbiol 2006;60:1319-1322. [PubMed]
66. Perine PL, Krause DW, Awoke S, McDade JE. Single dose doxycycline treatment of louse borne relapsing fever and epidemic typhus. Lancet 1974;2:742-744. [PubMed]
67. Perine PL, Teklu B. Antibiotic treatment of louse-borne relapsing fever in Ethiopia: A report of 377 cases. Am J Trop Med Hyg 1983;32:1096-1100. [PubMed]
68. Plasterk RHA, Simon MI, Barbour AG. Transposition of structural genes to an expression sequence on a linear plasmid causes antigenic variation in the bacterium Borrelia hermsii. Nature 1985;318:257-263. [PubMed]
69. Platonov AE, Karan LS, Kolyasnikova NM, Makhneva NA, Toporkova MG, Maleev VV, Fish D, Krause PJ. Humans infected with relapsing fever spirochete Borrelia miyamotoi, Russia. Emerg Infect Dis 2011;17:1816-1823. [PubMed]
70. Ramos JM, Malmierca E, Reyes F, Tesfamariam A. Results of a 10-year survey of louse-borne relapsing fever in southern Ethiopia: a decline in endemnicity. Ann Trop Med Parsitol 2008;102:467-469. [PubMed]
71. Ramos JM, Malmierca E, Reyes F, Wolde W, Galata A, Tesfamariam A, Gorgolas M. Characteristics of louse-borne relapsing fever in Ethiopian children and adults. Ann Trop Med Parisitol 2004;98:191-196. [PubMed]
72. Restrepo BI, Barbour AG. Antigenic diversity in the bacterium B. hermsii through “somatic mutations” in rearranged vmp genes. Cell 1994;78:867-876. [PubMed]
73. Richter D, Schlee DB, Matuschka FR. Relapsing fever-like spirochetes infecting European vector tick of Lyme disease agent. Emerg Infect Dis 2003;9:697-701. [PubMed]
74. Salkeld D, Cinkovich S, Nieto NC. Tick-borne pathogens in northwestern California, USA. Emerg Infect Dis 2014;20:493-494. [PubMed]
75. Sato K, Takano A, Konnai S, Nakao M, Ito T, Koyama K, Kaneko M, Ohnishi M, Kawabata H. Human infections with Borrelia miyamotoi, Japan. Emerg Infect Dis 2014;20:1391-1393. [PubMed]
76. Schwan TG, Anderson JM, Lopez JE, Fischer RJ, Raffel SJ, McCoy BN, Safronetz D, Sogoba N, Maïga O, Traoré SF. Endemic foci of the tick-borne relapsing fever spirochete Borrelia crocidurae in Mali, West Africa, and the potential for human infection. PLoS Negl Trop Dis. 2012;6:e1924. [PubMed]
77. Schwan TG, Hinnebusch BJ. Bloodstream- versus tick-associated variants of a relapsing fever bacterium. Science. 1998;280:1938-1940. [PubMed]
78. Schwan TG, Raffel SJ, Schrumpf ME, Schrumpf ME, Webster LS, Marques AR, Spano R, Rood M, Burns J, Hu R. Tick-borne relapsing fever and Borrelia hermsii, Los Angeles County, California, USA. Emerg Infect Dis. 2009;15:1026-1031. [PubMed]
79. Schwan TG, Schrumpf ME, Hinnebusch BJ, Anderson DE Jr, Konkel ME. GlpQ: an antigen for serological discrimination between relapsing fever and Lyme borreliosis. J Clin Microbiol. 1996;34:2483-2492. [PubMed]
80. Scoles GA, Papero M, Beati L, Fish D. A relapsing fever group spirochete transmitted by Ixodes scapularis ticks. Vector Borne Zoonotic Dis 2001;1:21-34. [PubMed]
81. Seboxa T, Rahlenbeck SI. Treatment of louse-borne relapsing fever with low dose penicillin or tetracycline: a clinical trial. Scand J Infect Dis 1995;27:29-31. [PubMed]
82. Southern PM, Sanford JP. Relapsing fever: A clinical and microbiological review. Medicine 1969;48:129-149.
83. Takano A, Toyomane K, Konnai S, Ohashi K, Nakao M, Ito T, Andoh M, Maeda K, Watarai M, Sato K, Kawabata H. Tick surveillance for relapsing fever spirochete Borrelia miyamotoi in Hokkaido, Japan. PLoS One 2014 11;9:e104532. [PubMed]
84. Teklu B, Habte-Michael A, Warrell DA, White NJ, Wright DJ. Meptazinol diminishes the Jarisch-Herxheimer reaction of relapsing fever. Lancet 1983;1:835-839. [PubMed]
85. Tokarz R, Jain K, Bennett A, Briese T, Lipkin WI. Assessment of polymicrobial infections in New York State. Vector Borne Zoonotic Dis2010;10:217-221. [PubMed]
86. Trape JF, Diatta G, Arnathau C, Bitam I, Sarih M, Belghyti D, Bouattour A, Elguero E, Vial L, Mané Y, Baldé C, Prugnolle F, Chauvancy G, Mahé G, Granjon L, Duplantier JM, Durand P, Renaud F. The epidemiology and geographic distribution of relapsing fever borreliosis in West and North Africa, with a review of the Ornithodoros erraticus complex (Acari: Ixodida).PLoS One. 2013;8:e78473. [PubMed]
87. van Holten J, Tiems J and Jongen VH. Neonatal Borrelia duttoni infection: a report of three cases. Trop Doct 1997;27:115-116. [PubMed]
88. Vidal V, Scragg IG, Cutler SJ, Rockett KA, Fekade D, Warrell DA, Wright DJ, Kwiatkowski D. Variable major lipoprotein is a principal TNF-inducing factor of louse-borne relapsing fever. Nat Med 1998;4:1416-1420. [PubMed]
89. Wang CW, Lee CU. Malaria and relapsing fever following blood transfusion including the report of a case of congenital transmission of relapsing fever. Chin Med J 1936;50:241-248.
90. Warrell DA, Perine P, Krause D, Bing D, MacDougal S. Pathophysiology and immunology of the Jarisch-Herxheimer like reaction louse-borne relapsing fever: comparison of tetracycline and slow-release penicillin. J Infect Dis 1983;147:898-909. [PubMed]
91. Wilske B, Schreifer ME. Borrelia. In Murray, P. R., Baron, E. J., Jorgensen, J., et al. (eds.): Manual of Clinical Microbiology. Washington, D.C., American Society for Microbiology, 2003, pp. 937-954.
![]()
Tables
Table 1. Manifestations of tick-borne relapsing fever acquired in the northwestern United States and southwestern British Columbia. (Adapted from Dworkin MS, Schwan TG, Anderson DE, Borchardt SM. Tick-borne relapsing fever. Inf Dis N Am 2008;22:449-468.13).
| Sign or symptom | % | Sign or symptom | % |
|---|---|---|---|
| Headache | 94 | Photophobia | 25 |
| Myalgia | 92 | Neck pain | 24 |
| Chills | 88 | Rash | 18 |
| Nausea | 76 | Dysuria | 13 |
| Arthralgia | 73 | Jaundice | 10 |
| Vomiting | 71 | Hepatomegaly | 10 |
| Abdominal pain | 44 | Splenomegaly | 6 |
| Confusion | 38 | Conjunctival injection | 5 |
| Dry cough | 27 | Eschar | 2 |
| Eye pain | 26 | Meningitis | 2 |
| Diarrhea | 25 | Nuchal rigidity | 2 |
| Dizziness | 25 |
Table 2. Antibiotic treatment of tick-borne and louse-borne relapsing fever in adults. (Adapted from Dennis DT, Hayes EB. Relapsing fever. In: Braunwald E, Hauser SL, Fauci AS, Longo DL, Kasper DL, Jameson JL, editors. Harrison’s principles of internal medicine. 16th edition. New York: McGraw-Hill; 2005).
| Medication | Tick-borne relapsing fever (7-day adult dosage schedule) | Louse-borne relapsing fever (single dose) |
|---|---|---|
| Oral | ||
| Doxycycline | 100 mg every 12 hours | 100 mg |
| Erythromycin | 500 mg every 6 hours | 500 mg |
| Tetracycline | 500 mg every 6 hours | 500 mg |
| Parenteral* | ||
| Doxycycline | 100 mg every 12 hours | 100 mg |
| Erythromycin | 500 mg every 6 hours | 500 mg |
| Penicillin G (procaine) | 600,000 IU daily | 600,000 IU |
| Tetracycline | 250 mg every 6 hours | 250 mg |
* Parenteral medication should be continued until oral medication is tolerated. If oral medication is tolerated at the time of diagnosis, parenteral medication may not be necessary.
What's New
Hingwe, A. Jarisch-Herxheimer reaction. 2009
Steere AC, McHugh G, et al. Prospective Study of Serologic Tests for Lyme Disease. Clin Infect Dis. 2008 Jul 15;47:188-95.
Cutler SJ. Possibilities for Relapsing Fever Reemergence. Emerg Infect Dis, March 2006.