
Salmonella typhi (Typhoid Fever) and S. paratyphi (Paratyphoid Fever)
Authors: David B. Huang, MD, PhD, MPH, Nicholas J. White, M.D.,Herbert L. DuPont, MD
MICROBIOLOGY
Typhoid and paratyphoid fevers are commonly grouped together under the collective term 'enteric fever'. Typhoid is caused by Salmonella typhi (strictly termed S. enterica sub-species enterica serotype typhi) (236) and paratyphoid is caused by either Salmonella paratyphi A, B, or C. Serologically S. typhi is LPS antigen 09, 12, protein flagellar antigen Hd, and capsular polysaccharide antigen Vi positive. Salmonella paratyphi B is also known as S. schottmuelleri, and Salmonella paratyphi C as S. hirschfeldii. These Salmonelloses are highly adapted infections of man, having no animal or environmental reservoir. Occasionally other Salmonellae may cause an enteric fever-like syndrome. The complete genome of S. typhi CT 18 has been sequenced (175). All isolates of S. typhi are closely related, although the genome is remarkably plastic (with homologous recombination around 7 ribosomal RNA genes) (159). Typhoid fever was once a major cause of morbidity and mortality throughout the world with a case fatality rate of approximately 15% (65,120). Over the past century the infection has been largely eradicated from more affluent temperate countries (261), although it remains a major infection in tropical areas of the world (119). Precise estimates of the mortality and morbidity of infectious diseases in poor countries are notoriously unreliable, but estimates suggest that there are approximately 16,000,000 cases of typhoid each year, with 600,000 deaths (129).
EPIDEMIOLOGY
Typhoid and paratyphoid are transmitted mainly by the fecal-oral route. In most cases an asymptomatic carrier of S. typhi, or an individual who has recently recovered from the infection, continues to excrete large numbers of organisms in the stool and contaminates food or water, either through direct food handling, through transfer of bacteria by flies and other insects, or by contamination of potable water (150,151,152). Approximately 10% of patients recovering from typhoid fever excreteS. typhi in the stool for three months, and in the past 2-3% became permanent carriers. These infections have great potential for epidemic spread therefore (227,233). In the tropics, enteric fever tends to be more common during the hot dry seasons when the concentration of bacteria in rivers and streams increases, or in the rainy season if flooding distributes sewage to drinking water sources. In some areas the incidence of typhoid may be as high as 1,000 cases per 100,000 population per year (Figure 1). In such areas typhoid is predominantly a disease of children, and stool excretion of S. typhi during and after infection is the main source of the infection. In such areasSalmonella typhi infections are commonly mild and self limiting. Severe disease represents the "tip of the iceberg". During fever surveillance in Dhaka urban slum, bacteremic typhoid fever incidence was determined to be 3.9 episodes/1,000 person-years (36). In temperate countries persistent carriers are a more important reservoir of infection (119). For travelers the highest attack rates are associated with visits to Peru [17 per 105 visits], India [11/105 visits], and Pakistan [10/105 visits]. Although Indonesia has a reported annual incidence up to 1%, the attack rate for travelers is low. In general, the mortality of enteric fever is low (< 1%) where antibiotics are available, but in poorer areas, or in the context of natural disasters, war, migrations, large concentrated refugee populations, and other privations, the mortality may rise to 10-30%, despite antibiotic therapy. Typhoid tends to cluster in families (152), presumably reflecting a common source of the infection and is associated with poverty and poor housing. Apart from exposure to the contaminated food (often ice creams or iced drinks), poultry droppings (6) or water source, descriptions of sexual transmission of typhoid fever have been reported among men who denied travel abroad and had sexual exposure to a asymptomatic male S. typhoid carrier (190). A number of host factors increase the risk of Salmonella infections. Disease related (achlorhydria) or iatrogenic (antacids, H2 blockers, proton pump inhibitors) reduction in stomach acidity or gut pathology (surgery, inflammatory bowel disease, malignancy) and recent antibiotics increase the susceptibility to infection. Disease related or iatrogenic immunosuppression and several other infections, notably schistosomiasis, malaria (151,152), histoplasmosis and bartonellosis, are associated with an increased risk of Salmonella infections. Typhoid is more common, and more severe at the extremes of age. Neonatal typhoid usually acquired from the mother may follow a fulminant course often with meningitis (25,46). Patients with hemoglobinopathies, particularly sickle cell disease, are also at increased risk.
CLINICAL MANIFESTATIONS
The clinical features of enteric fever vary considerably between different geographic regions. In many areas typhoid becomes the leading differential diagnosis of a patient with a fever which has lasted for more than one week. The clinical features of typhoid and paratyphoid fever are generally similar, although paratyphoid tends to be a more mild infection (65). Most patients with enteric fever present with a non-specific gradual onset of an influenza-like illness although Salmonella typhi infection can present with fever and a bewildering array of signs and symptoms (127) ranging from non-metastatic central nervous system syndromes including psychosis and cerebellar ataxia (241), to focal involvement of bone (77), liver (88,130,210), spleen (10), rhabdomyolysis (171), psoas abscess (73), testes (264), meninges (145,219), vascular prostheses, and atheromatous plaques. In general the enteric fevers are sub-acute infections with an incubation period of approximately 7 - 14 days (range 3-60 days) following exposure. The illness begins insidiously with non-specific signs and symptoms of fever (192), headache, muscle and joint aches, malaise, lassitude, anorexia, often a dry cough (sometimes associated with a sore throat) (215). The spleen enlarges, but lymphadenopathy is not usually prominent. There may be a few rose spots (sparse, pink, macular papular lesions which blanch with pressure and fade after two or three days) on the thorax or abdomen (usually less than 10), but these are often unnoticed, particularly in dark skinned patients. In paratyphoid fever rose spots may be more prominent. The classic "stepladder fever" of typhoid is unusual although the fever does become higher as the disease progresses, until it levels between 39°C and 40°C. Mild chills and sweating are common but true rigors are rare. Relative bradycardia is considered common in typhoid although in many series this has not been a feature of the disease. Some abdominal complaints are common although eitherdiarrhea or constipation may occur. There is usually some abdominal discomfort, and even in the first week of the disease the patient may notice passage per-rectum of a small amount of blood or melena. Normal bowel habit is unusual in typhoid. Diarrhea is more common in infants (30,199), and in patients with AIDS. Constipation occurs in approximately 40% of patients. A fulminant onset with a septic shock presentation may occur but is unusual.
The clinical evolution of untreated typhoid is divided classically into weeks (65). During the first week the fever rises gradually, and in the second week the fever reaches a high plateau. By the second week the patient has become progressively weaker, lost weight, and has often developed the characteristic affect from which typhoid derives its name (typhoid means "like typhus", which in turn derives from the Greek typhos meaning smoke, and refers to the clouding of the sensorium in these infections). The patient remains apathetic or depressed, anergic, often confused and withdrawn while lying in bed, yet sleep does not come easily. By the third week of infection, if untreated, a dangerous stage is entered upon in which either intestinal perforation or hemorrhage become more likely as the necrotic Peyer's patches either erode through the wall of the terminal ileum (33,46,47) or penetrate a large blood vessel. In a large series reported before the pre-chloramphenicol era, intestinal hemorrhage occurred in 7-21% of cases and intestinal perforation in between 0.7 and 4.7% of cases (65). In the antibiotic era the incidence of perforation has fallen slightly to approximately 3% of cases, and clinically significant intestinal bleeding now occurs in less than 2% although figures still vary considerably from series to series. The risk of both hemorrhage and perforation increase from the middle of the second week. In the third week of the illness the patients is often withdrawn, obtunded, or intermittently delirious. The abdomen becomes distended and there may be, vomiting, and abdominal pain. Right upper quadrant pain may indicate cholecystitis or cholangitis (3% of cases) whereas lower quadrant pain with signs of peritoneal irritation may indicate perforation. Table 1 lists reported extra-intestinal complications (127) that may occur in the third and fourth week such as pneumonia (177), ARDS (41), the development of acute psychosis, coma (32,188), myocarditis (183), pericarditis, orchitis (264), venous thrombosis,(100) splenic rupture, (9) meningitis, (107,145) osteitis (142), hepatic dysfunction (130), and occasional renal failure (221). If the patient survives this phase of the illness there follows a gradual recovery.
As the duration of infection is an important determinant of the risk of severe complications, a delay in receiving appropriate antibiotic treatment may have serious consequences. In some endemic areas, multi-drug resistance (and thus delayed treatment with effective antimicrobials) has led to an increase in mortality, particularly in infants (25).

LABORATORY DIAGNOSIS
The clinical diagnosis of typhoid or paratyphoid is confirmed by culture of the organism from blood or bone marrow or another non-gastrointestinal site. Isolation of the organism from the duodenal secretions or the stool in a febrile patient is also suggestive of enteric fever (although of course fever from a different infection may occur in someone who has recently recovered from typhoid or in a chronic carrier). Stool cultures are positive in approximately 60% of children and 25% of adults (102). Excretion of S. typhi in the stool is more likely with higher blood bacterial counts, and children tend to have higher bacteremia than adults. Blood cultures are positive in 60% - 80% of patients with yields maximized by taking a large volume of blood. Lysis centrifugation and lysis plating methods accelerate identification of S. typhi from blood (201). The median bacterial count is one cfu per mL of blood (253). Approximately two thirds of these organisms are within phagocytic cells, and thus located in the buffy coat (200,255). Blood bacterial counts decline as the disease progresses. Bone marrow counts are approximately ten times higher (253). Bone marrow culture increases the diagnostic yield from blood cultures by approximately 30% (74,102,120,122). Biopsies of the rose-spots are also usually culture positive. S. typhi is usually present in the duodenum and can be recovered using the string test (122). This is also useful for identifying chronic gallbladder carriers (101). S. typhi is sometimes excreted in the urine and occasionally causes urinary tract infections, particularly if there are structural abnormalities of the urinary tract (158). In areas where S. haematobium is endemic, such as Egypt, urinary tract carriers outnumber enteric carriers of S. typhi. Urine antigen tests have been described recently (57) but these have not been evaluated sufficiently. Several PCR methods have been described, but these are not widely used (136,219,222,252). However, molecular typing is important in distinguishing recrudescent from newly acquired infections in endemic areas (254). Serological diagnosis is widely relied upon (125). The Widal test which measures the antibody titers to the somatic O and flagella H antigens is relied upon widely, although there are very divergent views on its utility (4). There have been several well documented epidemics in which the Widal was usually negative, but other epidemiological settings where it has proved useful. Overall sensitivity is approximately 70-80% with specificity ranging from 80-95% (178). New IgM and IgG based rapid serological tests have proved useful in some areas (24,64,148) but are not validated sufficiently for widespread adoption. A recent animal study suggests that antibodies to iron-regulated outer membrane protein of mice play an important role protection against S. typhi at the systemic and mucosal level (225).
SUSCEPTIBILITY IN VITRO AND IN VIVO
Salmonella typhi and Salmonella paratyphi A, B and C are susceptible in vitro to a variety of antibiotics. However, in vivo responses are not always predicted accurately from in vitro susceptibility, largely because of their predominantly intracellular location within phagocytic cells (59). For example, the aminoglycosides are highly effective in vitro but are ineffective in vivo because of their poor penetration into cells and susceptibility to the acid pH inside the phagolysosomes containing ingested bacteria. The in vitro susceptibility profile to antimicrobial drugs is shown in Table 2. In general in vitro susceptibility testing to the agents commonly used for the treatment of typhoid does predict the clinical response. In endemic areas, patients with mild typhoid may improve following administration of an antibiotic to which the organism is shown subsequently to be resistant in vitro. This represents self-cure in a semi-immune subject and natural resolution of the infection, and explains why therapeutic responses in semi-immunes are always superior to those in non-immune subjects. As Salmonella typhi and S. paratyphi are obligate infections of man, there are no appropriate animal models in which to test treatment regimens. In general S. typhimurium in a murine model has been used to assess pathophysiology and host defense mechanisms, but not treatment responses.
Chloramphenicol
Chloramphenicol has been used as a treatment for typhoid and paratyphoid fevers since 1948, when Woodward and his colleagues first demonstrated its effectiveness in Malaya while evaluating chloramphenicol in the treatment of scrub-typhus (263). A patient in their trials proved to have typhoid, and instead of the normally protracted debilitating fever, he responded well to the new antibiotic. Chloramphenicol has reduced the mortality of typhoid from 20% to less than 1%, and the duration of fever from 2-4 weeks to 4-5 days. It has provided the gold-standard against which other antibiotics have been compared. When chloramphenicol and ciprofloxacin have been compared for the treatment of enteric fever, no significant differences in clinical cure and time to defervescence have been found (97). Chloramphenicol has excellent cellular penetration and it is extensively distributed in the body. Chloramphenicol sensitive stains of S. typhi typically have MICs between 0.75 and 5μg/mL (Table 2). Thiamphenicol (in which the P-nitro group of the benzene ring of chloramphenicol is substituted by a methyl-sulphonyl group) has been used less frequently, but has given similar clinical results.
Ampicillin, Amoxicillin and Trimethoprim-Sulfamethoxazole
There have been many open evaluations and several comparisons of these drugs in typhoid fever (135,193). In general ampicillin, amoxicillin or trimethoprim-sulfamethoxazole have given similar, or slightly inferior results to those with chloramphenicol. They have emerged as effective and acceptable alternatives with trimethoprim-sulfamethoxazole holding a slight advantage over ampicillin, although many authorities still prefer chloramphenicol, particularly for severe infections (49). Ampicillin and amoxicillin have been the treatment of choice in pregnancy and in neonates. MIC values for ampicillin are typically 0.25 - 5μg/mL, either similar or one dilution lower for amoxicillin, and 0.125 - 0.5μg/mL for trimethoprim (Table 1). Although synergy can be demonstrated with sulfonamides in vitro, and the majority of clinical experience is with trimethoprim-sulfamethoxazole, the importance of synergy in determining the response to treatment in enteric fever is unclear. Some authorities consider trimethoprim alone to be equally effective, and less toxic. Unfortunately strains which are simultaneously resistant to all of these first-line drugs have become widespread in recent years (169,189). As a consequence the third generation cephalosporins and the fluoroquinolones have been increasingly used as multi-drug resistance has spread (7,27,55,62).
Resistance to Chloramphenicol, Ampicillin and Trimethoprim
Resistance to chloramphenicol, ampicillin, and trimethoprim-sulfamethoxazole is usually plasmid mediated. Resistance to chloramphenicol was reported within two years of its original introduction, but did not prove to be a major problem until the early 1970s (38,49,118). The extensively documented epidemic in Mexico involved chloramphenicol resistant S. typhi (108,174,249) which, in a few cases, were also resistant to the other first line antimicrobials. Over the following twenty years reports of similar chloramphenicol resistant organisms appeared in many other countries mostly in Central and South America and Asia (3,14,38,50,53,98,106,185). With increasing usage of ampicillin (or amoxicillin) and trimethoprim-sulfamethoxazole as alternatives (211), resistance to these antibiotics also developed (13,75,87,197,209). Resistance was shown to be transmissible by a single "R" factor (plasmid) (50,106,174). These also often encoded resistance to tetracyclines, sulfonamides and the aminoglycosides. In some countries, particularly those such as Thailand and Vietnam where trimethoprim-sulfamethoxazole was deployed widely, but chloramphenicol was not, the prevalence of chloramphenicol resistance fell before the arrival of multi-drug resistance in the early 1990s (49). Loss of chloramphenicol resistance has been a recent phenomenon in some other areas (226). In recent years, multi-drug resistance has been reported from the Americas, North and South Africa and the Middle East, although the biggest problems are in the Indian sub-continent, South-east Asia and China (8,12,69,115,163,164,189,197,241,262) while other areas have reported a decrease in multi-drug resistance (58). In many countries where typhoid fever is endemic the proportion of multi-drug resistant isolates has increased steadily and these now comprise the majority of strains isolated. Spread has resulted either from dissemination of a single MDR clone or transfer of the plasmid among multiple S. typhi strains (68). In a few areas (e.g. parts of India), where chloramphenicol use has declined, the proportion of MDR strains appears to have decreased again (229). Resistance is usually associated with a single large plasmid varying in Mr between approximately 90 X 106 and 120 X 106 which is of the incompatibility group H complex (usually H1) (197,221,231). S. typhi CT18 (which was sequenced fully) harbors a very large (218 kb) conjugative plasmid pHCM1 carrying multiple antibiotic resistance genes which contains 168 kb of sequence with >99% identity to R27, of an inc H1 plasmid isolated first in the 1960s (175). DNA probes identifying these plasmid encoded resistance genes have been used for molecular typing in epidemiological investigations (117).
The mechanism of resistance to chloramphenicol is usually the production of chloramphenicol acetyl transferase. For ampicillin, it is the production of beta-lactamases (usually TEM1, and therefore inhibited by clavulanic acid). Other mechanisms may contribute, as MDR strains are more resistant to amoxicillin-clavulanic acid than sensitive isolates (see Table 1). Trimethoprim and sulfamethoxazole resistance is mediated by alteration in the enzyme targets dihydrofolate reductase and dihydropteroate synthase, respectively. These are usually related to point mutations in the respective genes. MIC values for resistant isolates are typically greater than 125 to 256μg/ml for all three first line antibiotics. S. typhi carrying multi-drug resistant plasmids appears to be at least as virulent, and possibly more virulent, than fully drug sensitive strains (255).
Third Generation Cephalosporins
Multi-drug resistant (MDR) strains of S. typhi remains sensitive to the third generation cephalosporins, the fluoroquinolone antibiotics, aztreonam, and the carbapenems (7,40,55,91,156,163,169,195,224,232,245,259). Ceftriaxone has been the most widely used of the third generation cephalosporins, although there have been several studies with oral cefixime which is also very active in vitro. MIC values for both drugs are typically 0.06μg/ml. Fortunately, resistance to these compounds is still very rare (202).
Fluoroquinolones
S. typhi, and S. paratyphi A, B, and C are usually extremely sensitive to the fluoroquinolone antibiotics. In time-kill studies, the fluoroquinolones are significantly more rapidly bactericidal than the third generation cephalosporins. In general MICs for the individual fluoroquinolones against S. typhi and S. paratyphi parallel those against other Enterobacteriaeceae. In vivo these are the most active drugs, and they give the most rapid response rates, the highest cure rates, and the lowest rates of residual stool excretion. Although the earlier compounds enoxacin, cinoxacin and norfloxacin have proved effective in the treatment of typhoid, they have usually given inferior results, presumably because of poor oral bioavailability (168,206). Norfloxacin occupies an intermediate position. It is more active in vivo than enoxacin and cinoxacin but less effective than the newer fluoroquinolones. These earlier quinolones should not be used to treat typhoid. All the newer fluoroquinolones are highly active against S. typhi, although none are significantly better than ofloxacin or ciprofloxacin. Levofloxacin (the L-isomer of ofloxacin) is approximately twice as active as the racemic mixture.
Unfortunately, quinolone resistance has developed in S. paratyphi A (39) and, more importantly, in S. typhi, from Central Asia, southern India, Vietnam and Canada (51,72,170,173,176,191,194,222,234,235). In 1997, an outbreak of quinolone resistant typhoid occurred in Tajikistan involving 8000 people and claiming 150 lives (162). Quinolone resistance in S. typhi has increased alarmingly in these areas as a consequence of widespread availability of inexpensive fluoroquinolones. As in S. typhimurium and other bacteria, fluoroquinolone resistance is usually associated with single point mutations in the "quinolone resistance determining region" of the gyrA gene (37,112). To date this is the only locus that has been identified. This locus is chromosomal; not plasmid mediated, and does not appear to be transferable. The most commonly identified mutation has been a serine to phenylalanine substitution at position 83 (37,256). Less common have been aspartate to tyrosine or glycine at position 87. Reduced susceptibility to quinolones without these mutations has also been reported suggesting an alternative mechanism of resistance. S. typhi containing these gyr A mutations show reduced susceptibility to fluoroquinolones, although the MICs are often still below the current break points for fluoroquinolone resistance, and on disc susceptibility testing zone sizes may still indicate full susceptibility (these break points need revising for Salmonellae causing systemic infections). Compared with fluoroquinolone sensitive strains, MIC values are commonly two or three dilutions higher (ofloxacin MIC90 0.5μg/mL compared with 0.06 to 0.125μg/mL for quinolone-sensitive strains). Greater discrimination is found testing with nalidixic acid. With a nalidixic acid disc these fluoroquinolone resistant strains are found to be resistant, and give MICs > 32μg/mL compared with 4 to 8 μg/mL in sensitive isolates. In a recent series from Vietnam the mean (SD) zone diameter around an ofloxacin 5 μg disc was 30mm (3) with nalidixic acid sensitive organisms (N=381), and 22.5mm (2) around the 14 nalidixic acid resistant organisms (p<0.001) (256). These nalidixic acid resistant isolates are effectively fluoroquinolone resistant in vivo. Thus, nalidixic acid disc testing with a 30μg disc should be routine when evaluating S. typhi or S. paratyphi susceptibility. To date only single point mutations have been encountered, but additional mutations in gyrA, or other topoisomerase genes, conferring high level fluoroquinolone resistance (as in other Enterobacteriaeceae) can be expected to arise. Resistance to the third generation cephalosporins is still extremely rare. One study suggested that ceftriaxone be used in cases showing non-responsiveness to ciprofloxacin (154).
Mecillinam (Amdinocillin)
Mecillinam is available either as the parenteral formulation or as a pro-drug, pivmecillinam for oral use. 6 - beta- amidinopenicillin is very active against ampicillin sensitive strains of S. typhi with MIC values typically of 0.2μg/mL. Although it is more stable than ampicillin against the beta-lactamases produced by MDR strains, MIC values are higher (typically 0.8 to 2 μg/mL). When used alone for the treatment of typhoid, efficacy has been disappointing with relatively low cure rates and high rates of stool carriage (133). Mecillinam binds to PBP2, and in vitro synergy can be shown with other beta-lactam antibiotics. Combinations of mecillinam with ampicillin or pivmecillinam with pivampicillin given for 10 to 14 days have given good clinical results, although in the former study stool carriage rates were very high. These double beta-lactam combinations have rarely been used in recent years.
Furazolidone
This inexpensive nitrofuran derivative has been available for many years in tropical countries and has been used extensively for enteric infections (214). Although inferior to chloramphenicol in sensitive infections it retains sensitivity against multi-drug resistant strains of S. typhi. Furazolidone has been recently shown to be effective in an uncontrolled study of 56 children with MDR typhoid although fever clearance was slow; mean (SD): 5.9 (1.6) days range 3-10 days (141,214). However, oral bioavailability is very poor, and in the absence of further information, furazolidone cannot be recommended for enteric fever unless other more effective drugs are not available.
Aztreonam
The monobactam aztreonam is highly active against S. typhi in vitro with MIC90 values of 0.25µg/mL. Despite good results in earlier uncontrolled trials, aztreonam (6 g/day for 10 days) proved inferior to chloramphenicol (50 mg/kg/day for 14 days) in 44 adults in Peru with uncomplicated chloramphenicol sensitive enteric fever. Mean (SD) fever clearance was slower 6.6 (3.6) days compared with 4.5 (2.3) days, and seven patients failed compared to none in the chloramphenicol group (179).
Azithromycin
Although the macrolides and lincosamides have generally little or no activity against Salmonellae, the new macrolide, azithromycin, does have in vivo activity against S. typhi despite MIC values which are typically between 4 and 8μg/mL. S. typhi exhibits tolerance to this antimicrobial with an MBC - MIC ratio that commonly exceeds 8 although sub MIC concentrations cause temporary inhibition of growth (43). The MIC is highly dependent on pH; alkalinization reduces MICs to 0.25 to 0.5 mg/L (43), and the inoculum used. The good in vivo activity may result from having over 100-fold concentration in leucocytes. Clinical results with azithromycin were initially mixed (242,257) but recent studies confirm that azithromycin is an effective treatment for typhoid fever, including MDR and quinolone resistant infections. No resistance has yet been reported, although cost limits the widespread use of azithromycin.
Antimicrobial Pharmacokinetics in Enteric Fever
Chloramphenicol
Oral chloramphenicol, either as crystalline base or as the palmitate ester, is well absorbed in patients with uncomplicated enteric fever (16). Intravenous or intramuscular chloramphenicol succinate is a biologically inactive pro-drug for the active base. Systemic bioavailability of chloramphenicol base following intravenous administration of the succinate is between 50 and 80%. Plasma concentration profiles vary considerably between individuals. In Pakistan, children receiving either 75 or 100 mg/kg/day of intravenous chloramphenicol succinate 48 hours after starting treatment had mean (SD) peak levels of 15.4 (6.1) and 19.9 (12.2)μg/mL respectively, and trough levels of 8.8 (7.7) and 5.4 (2.6)μg/mL respectively (28,29). In an unrandomized study Ti et al in Singapore compared plasma concentrations following equivalent doses of oral and intravenous chloramphenicol in 11 and 15 patients respectively: plasma concentrations were approximately 50% lower in the parenteral group (237). Using a regimen of 60mg/kg daily orally or intravenously until defervescence followed by 40mg/kg/day to complete 14 days treatment in 31 Bangladeshi adults and children, Islam et al (128) found trough serum chloramphenicol concentrations on day 3 between 5 and 57μg/mL (median 18 μg/mL), and between 5 and 40 ug/mL on day 7 (median 20 ug/mL). Concentrations above 20μg/mL are known to suppress erythropoiesis (160). Thus, even with intravenous administration there is considerable inter-individual variability. The greatest controversy has surrounded intramuscular administration of chloramphenicol. Following the study of adults with either Rocky Mountain spotted fever or induced typhoid, it has been generally recommended that chloramphenicol should not be given by intramuscular injection because of poor bioavailability. In this relatively small study (only four in the oral group and 13 in the intramuscular group) plasma chloramphenicol levels after oral administration were approximately twice those following intramuscular administration of chloramphenicol sodium succinate (83). Later authors pointed out that this difference could be explained by the incomplete systemic bioavailability of chloramphenicol base following administration of the succinate pro-drug. Subsequently Shann et al studied 57 children in Papua New Guinea with a variety of infections and showed that both peak serum concentrations and AUC values were similar following intramuscular and intravenous chloramphenicol sodium succinate (218). In a randomized comparison in 29 Nepalese adults with suspected uncomplicated typhoid or paratyphoid fever given 30mg/kg of succinate ester, mean (SD) peak plasma chloramphenicol concentrations following intramuscular administration were 7.8 (3.6) μg/mL compared with 16.2 (9.1) μg/mL following intravenous administration, but AUC values were not significantly different with the two routes of administration indicating similar bioavailability (2). In the 16 culture positive patients, chloramphenicol plasma clearance correlated weakly with measures of liver blood flow (indocyanine green clearance) and metabolic function (antipyrine clearance), but was unrelated to glomerular filtration rate (iothalamate clearance).
Ceftriaxone
Trough plasma ceftriaxone concentrations following an intravenous dose of 3 grams/day are usually greater than 11 μg/mL (which corresponds approximately to an unbound concentration of 0.5 μg/mL), concentrations at least eight times the usual MIC for S. typhi (1).
Ofloxacin
The pharmacokinetic properties of intravenous and oral ofloxacin have been studied recently in children with multi-drug resistant typhoid fever (21). The median (95% CI) peak serum concentrations following an intravenous infusion of 7.5mg/kg were 8.7 (7.6 to 9.7) μg/mL and 5.5 (4.7 to 6.3) μg/mL for oral ofloxacin. These were 10 to 100 times higher than the maximum MIC values for S. typhi. The mean (95%) estimated oral bioavailability was 91% (74 to 109%). Although systemic clearance values were slightly higher than reported previously in adults with other infections, these data suggest that dose regimens should be the same in adults and children.
ANTIMICROBIAL THERAPY
Use of chloramphenicol, ampicillin, and TMP-SMZ can still be appropriately used in many areas of the world for treatment of susceptible strains of S. typhi and S. paratyphi. These antimicrobials are widely available and inexpensive drugs for treatment of uncomplicated cases of typhoid fever (79). The majority of patients with typhoid or paratyphoid fevers have uncomplicated infections and present with a febrile illness. Most patients can take oral treatment and 90% of cases are treated as outpatients. The proportion of patients who present with complicated infections varies considerably; for example in Nepal and Vietnam the majority of patients with typhoid have uncomplicated infections and many are still able to walk despite having positive blood cultures. In contrast in Jakarta, Indonesia, severe infections are relatively common, particularly in children, and often present with encephalopathy or shock (120). These patients obviously require parenteral treatment.
With the extensive spread of multi-drug resistant Salmonella typhi chloramphenicol can no longer be regarded the drug of choice for suspected enteric fever (113,196). In uncomplicated infections the median time to fever clearance in fully sensitive infections is usually 4 - 5 days. It is not uncommon for blood cultures to remain positive up to the third day of treatment with chloramphenicol in a fully sensitive infection. The fluoroquinolones should now be regarded as the treatment of first choice for typhoid fever. They sterilize the blood more rapidly than other drugs, and in general fever clearance times have ranged between 3 and 5 days with this group of drugs (Table 3). Fever lasting one week following fluoroquinolone treatment is unusual and usually indicates nalidixic-acid (i.e.quinolone) resistance. With the third generation cephalosporins fever clearance times have been longer, generally ranging between 5 and 8 days ( Table3) (104,223,240,258). Studies with short course fluoroquinolone treatment suggest that the duration of fever does not reliably reflect the duration of infection. Two day treatments with fluoroquinolones, which have over 85% treatment efficacy (251), are associated with a fever clearance time of 4 - 5 days, i.e. the patient is febrile for a longer period than the treatment is given. Patients with background immunity will have a better response to treatment than non-immune persons, and may self cure with ineffective drug treatment. Oligosymptomatic patients with mild fever will usually respond rapidly and have a low incidence of relapse. In a recent study from Nepal, high plasma concentrations of proinflammatory cytokines, reflecting a more severe infection, were associated with a delayed response to antimicrobial treatment, and an increased risk of relapse (45). Quinolone resistance poses a major therapeutic problem. Decreased in vitro susceptibility and diminished clinical response to quinolone therapy have resulted in reevaluation of susceptible break points for S. typhi (213). A study using an in vitro infection model to determine the pharmacokinetic and dynamic measure of fluoroquinolone activity against wild-type and resistant S. typhi suggested that the susceptible breakpoints for ciprofloxacin and gatifloxacin were 0.12 µg/ml and levofloxacin was 0.25 μg/ml (34). MDR quinolone resistant S. typhiusually responds to azithromycin, long courses of high dose fluoroquinolones, or third generation cephalosporins, but the optimum treatment has not been determined.
Drug of Choice
The fluoroquinolones are now the treatment of choice for typhoid fever (Table 6). In the past chloramphenicol or trimethoprim-sulfamethoxazole have given equivalent results in randomized trials and have been considered equivalent first line treatments (70,211). Ampicillin has given either equal or slightly inferior therapeutic results and is considered acceptable empiric therapy (181), and of particular value in the eradication of chronic gall-bladder carriage. Amoxicillin is certainly as good as ampicillin, and with better oral bioavailability and less iatrogenic diarrhea, may be considered preferable where cost is not a limiting factor.
There are insufficient studies with trimethoprim alone to conclude that this can be substituted for trimethoprim-sulfamethoxazole, however, small studies suggest equivalence (96,161). The risk of serious drug toxicity (hepatitis, erythema multiforme) is 30-50% lower with trimethoprim alone. However in many endemic areas formulations of trimethoprim alone are unavailable.
The newer fluoroquinolones have proved the most effective drugs for the treatment of enteric fever (91,177,223,240). They have given the highest cure rates, and the lowest carrier rates, without significant adverse effects in treatment courses as short as 2 days (250,251). This compares favorably with the general recommendation of 2 - 3 week courses of either chloramphenicol, trimethoprim-sulfamethoxazole, or ampicillin (amoxicillin). The fluoroquinolones are significantly better than all other classes of antimicrobials against quinolone sensitive S. typhi. Short course fluoroquinolone therapy is particularly effective in epidemic containment (223). The clinical trials are reviewed in Table 3. There have been a total of 16 randomized controlled trials involving the newer fluoroquinolones, (i.e. excluding cinoxacin, enoxacin, andnorfloxacin) which together have enrolled and treated 984 patients with culture confirmed enteric fever (>95% S. typhi, and mostly multi-drug resistant). The mean fever clearance time was 3.7 days ranging between 2.5 and 5.2 days. The overall mean (95% CI) pooled clinical cure rate was 97.8 (96.6 to 98.6)% and the microbiological cure rate was 99.4 (98.6 to 99.8)%. Several of the more recent studies have been conducted in areas where quinolone resistance has developed and have given lower response rates. The mean (95% CI) relapse rate was 1.3% (0.7 to 2.3). In over half the studies there were no relapses (i.e. median relapse rate: 0%). Of the 591 patients for whom follow-up stool cultures were reported, only one (0.2%) was identified as a carrier in these series. This compares with a rate of approximately 3% with other drugs and strongly suggests that fluoroquinolones prevent the carrier state. Ofloxacin has been the most extensively evaluated of the fluoroquinolones, althoughciprofloxacin, fleroxacin, and pefloxacin have all given similar results. There is no reason a priori to suspect that other drugs in the same class with good oral bioavailability would give inferior responses. All have excellent activity in vitro. Norfloxacin, cinoxacin and enoxacin have insufficient systemic bioavailability and should not be used to treat enteric fever if the newer agents are available.
There have been 16 randomized trials involving the third generation cephalosporins. These have enrolled and treated 528 patients (Table 4). Mean fever clearance times were 6.9 days ranging from 5.2 to 8.3 days. In general longer courses (>7 days) have given higher cure rates, and lower relapse rates (23). The overall mean (95%) pooled clinical and microbiological cure rates were 90% (95% CI 85 to 95%) and 97% (96 to 98%) respectively. The median relapse rate in these series following cephalosporin treatment was 4%. Thus the fluoroquinolones are clearly superior to the oral or parenteral third generation cephalosporins in multi-drug resistant typhoid and they are less expensive. There are insufficient comparative studies with chloramphenicol, trimethoprim-sulfamethoxazole, or ampicillin (amoxicillin) in fully sensitiveS. typhi and S. paratyphi infections for firm conclusions, but the available data suggests that the fluoroquinolones are superior. Even in those areas where antimicrobial resistance is unusual the fluoroquinolones offer the advantages of a very well tolerated short course treatment with very low relapse and carrier rates, and efficacy should the infection prove subsequently to be resistant to the other antibiotics. Azithromycin is becoming established as effective alternative second-line drug with four recent randomized trials attesting to its safety and efficacy (Table 5). Aztreonam and imipenem should be considered as third line compounds.
Dose and Duration of Treatment
Since the introduction of the fluoroquinolones, the duration of treatment in clinical trials has become progressively shorter. Treatment courses of two days in Vietnam have given cure rates which are similar to those following longer courses, and regimens of ofloxacin at 10 mg/kg/day have given equivalent results to those with 15 mg/kg/day. Although further studies are required in other areas, in non-immune patients, these data suggest a considerable margin of therapeutic efficacy for longer courses of fluoroquinolone treatment. A five day fluoroquinolone treatment regimen (e.g. ofloxacin 10mg/kg/day) allows observation of the therapeutic response, and the option to continue treatment if the patient does not appear to be responding (usually indicative of quinolone resistance). In epidemic containment three days treatment is highly effective. For fluoroquinolone resistant infections 7-10 days of maximum doses should be given. The alternatives are azithromycin (8mg/kg/day) or a third generation cephalosporin (e.g. cefixime 20mg/kg/day) given for 7 days.
There is ample evidence in Vietnam to support a treatment course of ofloxacin for three days (15 mg/kg/day usually given as two doses per day) in previously healthy individuals. Although two-day regimens have not proved significantly inferior, cure rates have been slightly lower than with the three to five day regimens. These short course regimens have not been evaluated outside the endemic areas and it remains possible that background immunity or other unidentified host factors contribute significantly to these excellent clinical responses. Until further trials are conducted in other countries it would be prudent to give ofloxacin for five or seven days in a dose of 10 mg/kg/day. This also allows assessment of the patient’s response and the option to continue or switch treatment if the organism is found to be quinolone resistant. Recent pharmacokinetic studies support a twice daily dose regimen. Further studies are needed to define the importance of concentration-dependent killing and post-antibiotic effect with this class of compounds and to determine whether a once daily regimen would be equally or more effective. However, in the absence of such information, a twice daily regimen is recommended currently.
Chloramphenicol treatment of typhoid fever with a total adult dose of less than 15g, or a duration of treatment less than 10 days has been associated with an increased incidence of complications (86,198). The importance of dose and duration of treatment in preventing relapse is less clear. In early studies relapse was generally more common following chloramphenicol compared with no antibiotic treatment at all, but this reflected the eventual acquisition of immunity following self cure, and did not take into account the morbidity associated with a protracted illness, nor the hazards of intestinal hemorrhage or perforation (86). In general chloramphenicol,trimethoprim-sulfamethoxazole, and ampicillin have all been prescribed between 14 and 21 days. It is often recommended that the dose of oral or parenteral chloramphenicol should be reduced by 30% at the time of, or shortly after defervescence (from 50 mg/kg/day to 35 mg/kg/day; usual adult dose from 3 g to 2 g per day).
Multi-Drug Resistant Typhoid or Paratyphoid Fever
For multi-drug resistant typhoid or paratyphoid fever, fluoroquinolones are the treatment of choice. The oral third generation cephalosporins are also effective although in randomized comparative trials both parenteral ceftriaxone and oral cefixime have proved clinically inferior to ofloxacin. Azithromycin is also effective although therapeutic responses are slower than to the fluoroquinolones. Nevertheless these remain alternative treatments, and they are of particular value for the treatment of nalidixic acid (quinolone) resistant S. typhi (71). Fortunately, these infections have been confined largely to Central Asia, India and Vietnam, but with increasing use of fluoroquinolones, multi-drug resistant typhoid or paratyphoid fever can be expected to spread. The treatment rate with short course/cure fluoroquinolone treatments in nalidixic acid sensitive organisms consistently exceeds 95%. (It is worth re-emphasizing that all S. typhi isolates must be screened for nalidixic acid susceptibility). However, if the organisms are nalidixic acid resistant then, whether or not they are reported as sensitive to the fluoroquinolones, the failure rates for short course (<5 days) treatment are approximately 50%. Use of maximum permitted doses and extending the fluoroquinolone treatment course to seven or ten days will result in cure in >90% of cases -- although the overall clinical response is slower and fever clearance times are much longer (average 7 days). If nalidixic acid resistance is confirmed then the course of fluoroquinolones should be extended to 10-14 days and maximum doses used. The only available alternatives are azithromycin or the third generation cephalosporins. The third generation cephalosporins are associated with a slow resolution of fever and symptoms and a relapse rate of approximately 20%. Azithromycin is better, giving a 95% cure rate. Most of the nalidixic acid resistant isolates of S. typhi have also been fully resistant to chloramphenicol, trimethoprim-sulfamethoxazole, andampicillin. Although in theory amoxicillin-clavulanic acid might be considered an alternative to the fluoroquinolones, as ampicillin resistance is usually mediated by a TEM1 plasmid encoded β lactamase, preliminary clinical trials with this drug in multi-drug resistant typhoid have proved disappointing. There have been insufficient randomized comparative trials on which to make categorical recommendations for the treatment of quinolone-resistant typhoid but this is likely to pose increasing problems in the near future (6,90,187,216).
Combination Drugs
The only combination of drugs used widely for the treatment of typhoid and paratyphoid fevers is trimethoprim-sulfamethoxazole. The combination of ampicillin with chloramphenicol proved no more effective than chloramphenicol alone (193). Recent studies have evaluated a combination of fluoroquinolones and azithromycin, but the role of this combination is yet to be determined.
Children
The advantages of the fluoroquinolones in terms of efficacy and the simplicity of short course treatment outweigh theoretical concerns over toxicity. In those areas where resistance is unusual, chloramphenicol, trimethoprim-sulfamethoxazole or ampicillin ( amoxicillin) may all be used. Multi-drug resistant typhoid fever in children has been treated successfully with the third generation cephalosporins, although parenteral ceftriaxone is impractical, and oral cefixime has given slow responses with mean times to fever clearance over five days (105). In a comparative study in 138 Vietnamese children with uncomplicated typhoid fever, oral ofloxacin proved significantly better than oral cefixime with median (95%CI) fever clearance times of 102 (78 to 108) hours and 177 (150 to 204) hours, respectively, and failure rates of 3% and 21%, respectively. In many countries typhoid and paratyphoid fevers are predominantly infections of children (114). The fluoroquinolones are generally considered to be contraindicated in children because of their potential for cartilage toxicity. In immature experimental animals, principally beagle dogs, the fluoroquinolones cause damage to the cartilaginous endplates of long bones. There is no evidence that a similar process of joint damage occurs in humans, but caution has dictated that alternative drugs should be used in children. However, in areas with multi-drug resistant typhoid the orally administered alternatives for children would be oral third generation cephalosporins or azithromycin (20,26,84,166,184). These are more expensive and less effective unless quinolone resistant strains are prevalent. Fluoroquinolones have been evaluated in children with infections caused by other non-typhi multi-drug resistant Salmonellae without complications (60,110,140). Large studies in Vietnam have evaluated fluoroquinolones given for one week or less in the treatment of uncomplicated typhoid fever in adults and children (223,251). In total, over 500 Vietnamese children less than 14 years have been enrolled in prospective randomized comparisons with both short term and long term follow up examining joint or skeletal toxicity with the use of fluoroquinolones. These comparisons have not revealed evidence of adverse effects (22,228). In a controlled comparison 326 children received either short course ofloxacin (total dose 45 mg/kg over 3 days), or a longer duration of ciprofloxacin (total dose 140 mg/kg over 7-10 days). These children were compared to control children from the same location and of the same age who had not received any fluoroquinolones. Over a two year period of follow up, there were no short or long term adverse effects and no evidence of impaired growth, indeed children who received the higher dose (ciprofloxacin) showed a significant increase in growth (height velocity) during the first year of the study compared with untreated healthy controls (22). Similar negative results were obtained in a recent detailed evaluation of growth rates and joint symptoms in 75 children with suspected typhoid fever treated with ciprofloxacin (78). Taken together, these data suggest that short courses of fluoroquinolones are safe and effective in children with multi-drug resistant typhoid and should now be the treatment of choice. Given their other advantages in this potentially life-threatening disease and their safety profile not only in typhoid, but also in children treated for other infections (notably protracted high dosages in cystic fibrosis) (42,60,110,208), there is no reason to withhold fluoroquinolones from children with drug sensitive enteric fever either.
Pregnancy
Ampicillin or amoxicillin are considered the treatment of choice for enteric fever in pregnancy. Ciprofloxacin or ofloxacin should be given for multi-drug resistant infections, or to women coming from areas where these strains are prevalent, before sensitivities become available. Treatment can then be changed to ampicillin if the infecting organism is sensitive (146). Vertical intrauterine transmission has been reported resulting in severe neonatal infection, so the newborn needs to be observed carefully and treated for typhoid if there are signs of infection.
Severe Typhoid
There have been no recent randomized controlled trials of the specific antibiotic treatment of severe typhoid. The agents used for the oral treatment of uncomplicated typhoid may all be given parenterally, and all are effective (84). Our current preference is for intravenous fluoroquinolones; ofloxacin can be used at a dose of 5mg/kg 12-hourly by intravenous infusion. The optimum duration of treatment has not been determined. Our recommendation is to give seven to fourteen days antibiotic treatment in severe typhoid. In a double blind randomized placebo controlled trial of severe typhoid conducted in Jakarta, high dose corticosteroids (dexamethasone 3 mg/kg followed by 1 mg/kg six hourly for hours) reduced mortality from 56% (10/18) to 10% (2/20).
The Immunocompromised Patient
Immunocompromised patients with typhoid or paratyphoid fever have a high rate of relapse and should not receive short-course treatment, although the optimum duration of treatment has not been established. Empirically the duration of treatment should be proportional to the degree of immunosuppression. A three to six week course of fluoroquinolones should be sufficient in mildly compromised patients. In patients with AIDS between six weeks and eight months of fluoroquinolone treatment has been given. The fluoroquinolones and zidovudine show synergistic antibiotic activity against S. typhi in vitro. In patients infected with sensitive organisms, trimethoprim-sulfamethoxazole prophylaxis in AIDS will also contribute to prevention of relapse and allow a shorter course of fluoroquinolones (3 weeks) to be given. There are insufficient data in this important area to provide confident treatment recommendations.
Extraintestinal Infections
Therapy for CNS involvement, cardiac infections especially endocarditis, pulmonary infections (pneumonia and empyema, bone and joint infection (osteomyelitis, septic arthritis), liver abscess, splenic abscess, genitourinary infections, subcutaneous infection and hematological complications (hematophagocystosis) are reviewed in detail in the article below. The drug of choice is usually a quinolone, but with the emergence of quinolone resistance, third generation cephalosporins, especially ceftriaxone, have been increasingly used; we recommend that ceftriaxone be given every 12 hours rather than 24 hours for pharmacodynamic reasons.
Review Article: Huang DB, DuPont HL. Problem pathogens: extra-intestinal complications of Salmonella enterica serotype Typhi infection. Lancet Infect Dis 2005;5:341-8.
The Carrier State
The objective of treatment in uncomplicated typhoid is to prevent progression to severe disease and complications, and to reduce the incidence of relapse and prevent the carrier state. As asymptomatic carriers are a major source of the infection, elimination of carriers has major epidemiological importance. The carrier state occurs in up to 10% of patients (usually 3%) receiving conventional treatments and in less than 1% of patients receiving fluoroquinolones. Approximately 25% of carriers report no acute infection. Carriers are people who excrete in the stool, or urine, for more than three months following an acute infection. Following chloramphenicoltreatment the proportion of carriers at the end of three months is approximately 4% and 3% at one year (65). The carrier state is more likely to occur in adults, and more likely in females than males. Carriers are usually asymptomatic although they have an increased risk of gall-bladder cancer. High serum levels of antibody to the Vi antigen are useful diagnostically. A carrier may continue to excrete S. typhi throughout his or her life. Stool excretion is intermittent and variable in intensity with stool bacterial counts of up to 1010 S. typhi per gram of feces. Several spaced stool samples are needed therefore to exclude the carrier state. The fecal carrier state results from chronic infection of the gallbladder and is strongly linked to cholelithiasis. Management may therefore require a combination of medical and surgical treatment.
Compared with the large amount of information on the treatment of enteric fever, there is relatively little information on the treatment of S. typhi carriers. Chloramphenicol does not seem to be effective. High dose ampicillin or amoxicillin (14 days of intravenous treatment or three months of oral treatment in combination with probenecid) have given the best results. Phillips reviewed three studies (180) and concluded that eradication of the carrier state was obtained in 34 (71%) of 48 patients who had received 4 g of ampicillin/day for 28 days. Others have reported lower cure rates. Carriage in patients with gallstones with often not be eradicated with this regimen, and cholecystectomy may be needed (85). Recent experience with the fluoroquinolones suggests that these drugs may become the treatment of choice for chronic carriers. Ferreccio reported cure in 10 of 12 Chilean adult patients (93) given ciprofloxacin 750 mg twice daily for 28 days. Equally good results have been obtained elsewhere (204). There are no data on the management of carriers excreting multi-drug resistant and quinolone resistant organisms.
Whether fluoroquinolones should become the treatment of choice for all typhoid and paratyphoid fever and also for eradication of the carrier state remains unresolved. In countries where the quinolones are still considered contraindicated in children, then either trimethoprim-sulfamethoxazole or chloramphenicol remains satisfactory treatments for drug sensitive infections. Given for two weeks chloramphenicol has been associated with relapse rates of between 10% and 25%, compared with failure rates of less than 5% with the fluoroquinolones. However, there are insufficient randomized comparative trials between the fluoroquinolones and the conventional first line drugs in the treatment of drug sensitive infections to define the extent of the advantage. Depending on the source of antibiotics a three day course of fluoroquinolones is only slightly more expensive than a two week course of chloramphenicol or trimethoprim-sulfamethoxazole.
ADJUNCTIVE THERAPY
Surgical therapy and aspiration for extraintestinal complications of brain abscess, endocarditis, empyema, osteomyelitis, paravertebral abscess, septic arthritis, hepatic abscess, splenic abscess, renal abscess, pelvic infections and subcutaneous abscess are reviewed in detail in the article below.
ENDPOINTS FOR MONITORING THERAPY
Monitoring for Response to Treatment
Clinical Follow Up
Patients should be observed in hospital until their fever has returned to normal for at least one day, and they are able to sit and eat. Although the patient often begins to feel better within one or two days, the fever in typhoid is slow to resolve even with appropriate antibiotic treatment (220). Recent recommendations that treatment should be deemed to have failed if the fever persists for > 5 days are too strict (70), as many patients will be cured despite fever clearance longer than this. As can be seen from Table 4, the majority of patients treated effectively with the third generation cephalosporins will have fever clearance greater than 5 days. Fever clearance is usually defined as the time until the oral temperature has fallen below 37.5 °C and remained below this level for at least 24 hours. The most important parameter to observe is the patient’s general well being. If they are brighter, able to sit and take some food, or even walk, then the physician can afford to wait. But if their general condition is deteriorating, they are becoming more withdrawn, the pulse and fever are rising, and the abdomen is becoming more distended or painful, then intravenous treatment should be substituted, and continued beyond five days. In practice the therapeutic options are limited, particularly with multi-drug resistant typhoid. Parenteral treatment should always be given if there is any doubt about the oral route of administration.
Patients with severe typhoid should be admitted to an intensive care unit and monitored closely (46). The development of a perforation or hemorrhage does not indicate a treatment failure within one week of starting treatment. Perforation requires surgical intervention (11,47,247) with segmental resection and broadening of antimicrobial coverage to treat the associated peritonitis.
Microbiological Follow Up
It is not unusual following treatment with chloramphenicol, trimethoprim-sulfamethoxazole or ampicillin (amoxicillin) for blood cultures to remain positive for several days despite clinical improvement. Occasionally blood cultures have been positive in the second and third weeks of disease despite full in vitrosensitivity to the antibiotic being given. With fluoroquinolone treatment, it is unusual for blood cultures to be positive after the first 24 hours of treatment, and a positive day 3 culture indicates a significant risk of subsequent treatment failure.
In routine clinical practice it is not necessary to repeat blood cultures in patients who are clearly responding to treatment. If the patient does not respond or deteriorates then cultures should be repeated at any time, and if fever persists for 7 days, even if there is a clinical response, the cultures should be repeated. Cultures from sites other than blood or stool should be recultured on the 3rd and 7th day following the start of treatment. In order to identify S. typhi carriers, convalescent stool samples should be obtained in all patients. Three separate samples should be taken at 3-7 day intervals beginning one month after completion of treatment. Patients with repeated positive cultures should be educated about the public health risk they pose, started again on antibiotic treatment, and reviewed at monthly intervals.
Severe Typhoid
Severe typhoid carries a high mortality. There are two different syndromes. The first represents severe infection with a heavy bacterial load. The patient may present with septic shock or complications including acute renal failure, hepatic dysfunction (88,210), myocardial failure (183), disseminated intravascular coagulation (48,138), or encephalopathy (188). The encephalopathic presentation is particularly common in Java, where it was associated with a mortality of 56% (121). The second presentation is the culmination of a steady downhill progression and results from a focal necrotic process in the terminal ileum. The debilitated patient presents indicating either with signs of acute blood loss or peritonitis, intestinal hemorrhage, or perforation respectively (5,33,247) usually in the third or fourth week of disease. The clinical diagnosis of perforation can be difficult as localized abdominal discomfort with guarding and rebound may occur without evident perforation in typhoid. In severe typhoid the objective of treatment is to save life and to manage complications as early as possible. Although there was a period during which conservative management was considered acceptable in intestinal perforation, the weight of opinion now strongly favors immediate surgery (11,33,47,207). Patients with severe typhoid need intensive care. Cardiovascular monitoring should be started and blood should be grouped. Plasma electrolytes and renal function should be monitored, and the patient examined frequently for signs of intestinal blood loss or peritonitis. The mortality of intestinal perforation has been reduced significantly by prompt resuscitation with vigorous fluid administration to restore the intravascular volume and by the use of parenteral broad spectrum antibiotics to treat the fecal peritonitis (31,247). These should cover aerobic and anerobic bacteria. The choice of antibiotic will depend on which drug is being used for typhoid treatment. For example, if fluoroquinolones or third generation cephalosporins are being used then metronidazole should be added.
Intestinal Perforation
If perforation is suspected nasogastric suction should be started, and the patient resuscitated. Plain abdominal films should be obtained to look for subdiaphragmatic air. Once the hemodynamic status is stabilized, a laparotomy should be performed as soon as possible. Both small and large bowel should be examined. The choice of surgical procedure will depend on the extent of ulceration and the state of the bowel wall. Either resection or wedge excision of the ulcer with single or double layer closure of the perforation can be performed (11). Where the bowel wall looks friable or an ulcer is about to penetrate, these areas too may need pre-emptive surgery.
Intestinal Hemorrhage
Passage of a small quantity of blood per rectum is not unusual (approximately 10% of cases). In most cases intestinal bleeds can be managed with fluid replacement and transfusion, preferably of fresh blood. Uncontrolled hemorrhage may necessitate surgery. Intra-arterial vasopressin has also been used to control bleeding.
VACCINES
Indications
For over 100 years heat killed phenol treated whole organisms (either S. typhi alone, or combined with S. paratyphi A and B) have been used as vaccines (89). These vaccines are usually administered by subcutaneous injection. Monovalent whole cell typhoid vaccine contains not less than 109 heat killed, phenol preserved S. typhi bacteria/mL. These whole cell vaccines have given 51 to 77% protection, but unpleasant local and systemic side effects have been common with fever in up to 30%, and local pain and swelling in up to 60% of those vaccinated. Approximately 25% of vaccine recipients are sufficiently unwell to miss school or work. An acetone inactivated vaccine which may be given either by subcutaneous or intramuscular injection has been shown to be both more effective and more toxic. In a recent study 5 of 25,000 military personnel who received the acetone inactivated vaccine by I.M. injection required hospitalization. Most of the protective efficacy of the phenol, and acetone inactivated vaccines derives from the Vi antigen content, and this has led to the development of a parenteral purified Vi antigen vaccine. Two vaccines have now largely superseded the older crude vaccines; these are the purified parenteral Vi capsular polysaccharide antigen (182), and an oral live attenuated bacterium (Ty21a) (147). Both have a protective efficacy of between 65% and 70% with immunity lasting between 3 and 7 years (139) and they are generally well tolerated (89). These vaccines are generally not deployed in endemic areas. Several vaccines are under development including live attenuated S. typhi, containing autotrophic mutations, which may be more immunogenic than Ty21a, and could therefore be given in a single immunizing dose (123). Recently a new vaccine in which the S. typhi capsular polysaccharide (Vi) has been conjugated to non-toxic recombinant Pseudomonas aeruginosa exotoxin A has been developed (Vi-rEPA) and evaluated in a double blind placebo controlled trial in 11,091 children aged 2 to 5 years living in the Mekong delta region of Vietnam (149). The vaccine prevented severe disease, and had an overall protective efficacy of 91.5% (95% CI 77.1 to 99.6%) (149). The Vi-rEPA vaccine was also well tolerated; only 0.33% of vaccinated children had an area of swelling on the vaccinated arm >5 cm in diameter.
In general typhoid vaccines have not been deployed widely in endemic areas; most usage is in travelers. The currently available parenteral Vi antigen and oral live attenuated Ty21a vaccines give similar levels of protective efficacy, and there is little to choose between the two. A recent study suggests that a subset of nonclassical human HLA-E-restricted S. Typhi-specific CD8+ T cells derived from PBMC may contribute to host defense against intracellular organisms (203). Neither give 100% protection and neither vaccine is considered to provide adequate protective efficacy in children <18 months of age. The Ty21a is not generally recommended under the age of six. Thus, the Vi vaccine should be used for younger children although not below two years of age. Local and systemic reactions to parenteral typhoid vaccine begin within hours and last for up to three days. Subjects receiving typhoid vaccines should be warned about potential side effects (see Table 7).
Typhoid immunization is advised for laboratory workers handling the organisms and travelers to countries in Africa, some parts of Eastern Europe, Asia, Oceania, Central and South America and the Caribbean where sanitation and hygiene is poor. Typhoid immunization may not be necessary for individuals making short trips and staying in good accommodation. Typhoid immunization is not recommended for contacts of known carriers and has not been recommended in the past for epidemic containment. This prescription is under review; mass immunization could be of benefit, particularly in containing multi-drug resistant epidemics where there are no effective treatments (230,232).
Contraindications
Typhoid vaccines should not be given during an acute febrile illness, if there has been a previous reaction to the same vaccine and to pregnant women (unless there is clear indication). The oral Ty21a vaccine should not be given to patients who have a disease or drug treatment causing immunosuppression (including those who are HIV positive). The oral Ty21a vaccine also should not be given to patients receiving antibiotics, and efficacy is reduced if co-administered with mefloquine prophylaxis. A gap of three days between the mefloquine and the vaccine is recommended (35,124). There is a theoretical risk of interference in local immune responses if oral polio vaccine is co-administered with Ty21a; a gap of three weeks between the two is recommended.
PREVENTION
A high prevalence of typhoid reflects poor sanitation and hygiene. The most efficient methods for prevention involve provision of clean potable water and effective sewage disposal. Typhoid carriers should be identified and treated, and prevented from preparing foods until their carrier state has been eradicated. Because of familial clustering, ill members of the household of an identified case should be screened and treated. For the individual, prevention entails avoidance of potentially contaminated food or water. Dairy products, meat, and shellfish are all potential sources of infection. Non-bottled drinks, ice, uncooked food (apart from fruit and vegetables that can be shelled or peeled), and some desserts, particularly ice cream from an unreliable source, are also potential sources of infection.
COMMENTS AND CONTROVERSIES
Although the clinical trials data are very encouraging and indicate therapeutic superiority of the fluoroquinolones in the treatment of enteric fever, and the prevention of the carrier state, it is not certain how effective they are at preventing complications of typhoid. More information is also needed on the optimum treatment duration for immunocompromised patients.
REFERENCES
1. Acharya G, Crevoisier C, Butler T, Ho M, Tiwari M, Stoeckel K, Bradley CA. Pharmacokinetics of ceftriaxone in patients with typhoid fever. Antimicrob Agents Chemother 1994;38:2415-8. [PubMed]
2. Acharya GP, Davis TM, Ho M, Harris S, Chataut C, Acharya S, Tuhladar N, Kafle KE, Pokhrel B, Nosten F, Dance DA, Smith A, Weber A, White NJ. Factors affecting the pharmacokinetics of parenteral chloramphenicol in enteric fever. J Antimicrob Chemother 1997;40:91-8. [PubMed]
3. Agarwal SC. Chloramphenicol resistance of Salmonella species in India, 1959-61. Bull World Health Organ 1962;27:331-5. [PubMed]
4. Ahmed A, Basit A, Rehman AZ. Salmonella osteomyelitis. J Coll Physicians Surg Pak 2004;14:433-5. [PubMed]
5. Akgun Y, Bac B, Boylu S, Aban N, Tacyildiz I. Typhoid enteric perforation. Br J Surg 1995;82:1512-5. [PubMed]
6. Akinyemi KO, Smith SI, Oyefolu AO, Coker AO. Multidrug resistance in Salmonella enterica serovar typhi isolated from patients with typhoid fever complications in Lagos, Nigeria. Public Health 2005;119:321-7.[PubMed]
7. Alam MN, Haq SA, Das KK, Baral PK, Mazid MN, Siddique RU, Rahman KM, Hasan Z, Khan MA, Dutta P. Efficacy of ciprofloxacin in enteric fever: comparison of treatment duration in sensitive and multidrug-resistant Salmonella. Am J Trop Med Hyg 1995;53:306-11. [PubMed]
8. Albert MJ, Haider K, Nahar S, Kibriya AK, Hossain MA. Multiresistant Salmonella typhi in Bangladesh. J Antimicrob Chemother 1991;27:554-5. [PubMed]
9. Ali G, Kamili MA, Rashid S, Mansoor A, Lone BA, Allaqaband GQ. Spontaneous splenic rupture in typhoid fever. Postgrad Med J 1994;70:513-4.[PubMed]
10. Allal R, Kastler B, Gangi A, Bensaid AH, Bouali O, Cherrak C, Brun F, Dietemann JL. Splenic abscesses in typhoid fever: US and CT studies. J Comput Assist Tomogr 1993;17:90-3. [PubMed]
11. Ameh EA, Dogo PM, Attah MM, Nmadu PT. Comparison of three operations for typhoid perforation. Br J Surg 1997;84:558-9. [PubMed]
12. Anand AC, Kataria VK, Singh W, Chatterjee SK. Epidemic multiresistant enteric fever in eastern India. Lancet 1990;335:352. [PubMed]
13. Anderson ES. The problem and implications of chloramphenicol resistance in the typhoid bacillus. J Hyg (Lond) 1975;74:289-99. [PubMed]
14. Anderson ES, Smith HR. Chloramphenicol resistance in the typhoid bacillus. Br Med J 1972;3:329-31. [PubMed]
15. Arif N, Khan AA, Iqbal Z. Hepatic involvement with typhoid fever: a report of nine patients. J Pak Med Assoc 1990;40:4-9. [PubMed]
16. Arnold K, Hong CS, Nelwan R, Zavala-Trujillo I, Kadio A, Barros MA, de Garis S. Randomized comparative study of fleroxacin and chloramphenicol in typhoid fever. Am J Med 1993;94:195S-200S. [PubMed]
17. Arora A, Singh S, Aggarwal A, Aggarwal PK. Salmonella osteomyelitis in an otherwise healthy adult male-successful management with conservative treatment: a case report. J Orthop Surg (Hong Kong) 2003;11:217-20. [PubMed]
18. Aslam F, Bhaila I, Nadeem N, Fadoo Z. Salmonella typhi-infected lung hydatid cyst. Pediatr Infect Dis J 2005;24:270-2. [PubMed]
19. Baccaro FG. Primary psoas abscess due to Salmonella typhi. MedGenMed 1999:E16. [PubMed]
20. Bavdekar A, Chaudhari M, Bhave S, Pandit A. Ciprofloxacin in typhoid fever. Indian J Pediatr 1991;58:335-9. [PubMed]
21. Bethell DB, Day NP, Dung NM, McMullin C, Loan HT, Tam DT, Minh LT, Linh NT, Dung NQ, Vinh H, MacGowan AP, White LO, White NJ. Pharmacokinetics of oral and intravenous ofloxacin in children with multidrug-resistant typhoid fever. Antimicrob Agents Chemother 1996;40:2167-72. [PubMed]
22. Bethell DB, Hien TT, Phi LT, Day NP, Vinh H, Duong NM, Len NV, Chuong LV, White NJ. Effects on growth of single short courses of fluoroquinolones. Arch Dis Child 1996;74:44-6. [PubMed]
23. Bhutta ZA, Khan IA, Shadmani M. Failure of short-course ceftriaxone chemotherapy for multidrug-resistant typhoid fever in children: a randomized controlled trial in Pakistan. Antimicrob Agents Chemother 2000;44:450-2. [PubMed]
24. Bhutta ZA, Mansurali N. Rapid serologic diagnosis of pediatric typhoid fever in an endemic area: a prospective comparative evaluation of two dot-enzyme immunoassays and the Widal test. Am J Trop Med Hyg 1999;61:654-7. [PubMed].
25. Bhutta ZA. Impact of age and drug resistance on mortality in typhoid fever. Arch Dis Child 1996;75:214-7. [PubMed]
26. Bhutta ZA. Therapeutic aspects of typhoidal salmonellosis in childhood: the Karachi experience. Ann Trop Paediatr 1996;16:299-306. [PubMed]
27. Bhutta ZA, Khan IA, Molla AM. Therapy of multidrug-resistant typhoid fever with oral cefixime vs. intravenous ceftriaxone. Pediatr Infect Dis J 1994;13:990-4.[PubMed]
28. Bhutta ZA, Naqvi SH, Durrani S, Suria A. Chloramphenicol therapy of typhoid fever and its relationship to hepatic dysfunction. J Trop Pediatr 1991;37:320-2.[PubMed]
29. Bhutta ZA, Naqvi SH, Durrani S, Suria A. Chloramphenicol therapy of typhoid fever. J Pak Med Assoc 1991;41:26-30. [PubMed]
30. Bhutta ZA, Naqvi SH, Razzaq RA, Farooqui BJ. Multidrug-resistant typhoid in children: presentation and clinical features. Rev Infect Dis 1991;13:832-6. [PubMed]
31. Bissett IP. Typhoid enteric perforation. Br J Surg 1996;83:1478-9. [PubMed]
32. Biswal N. Neurological manifestations of typhoid fever in children. J Trop Pediatr 1994;40:190. [PubMed]
33. Bitar R, Tarpley J. Intestinal perforation in typhoid fever: a historical and state-of-the-art review. Rev Infect Dis 1985;7:257-71. [PubMed]
34. Booker BM, Smith PF, Forrest A, Bullock J, Kelchlin P, Bhavnani SM, Jones RN, Ambrose PG. Application of an in vitro infection model and simulation for reevaluation of fluoroquinolone breakpoints for Salmonella enterica serotype typhi. Antimicrob Agents Chemother 2005;49:1775-81. [PubMed]
35. Brachman PS, Metchock B, Kozarsky PE. Effects of antimalarial chemoprophylactic agents on the viability of the Ty21a typhoid vaccine strain. Clin Infect Dis 1992;15:1057-8. [PubMed]
36. Brooks WA, Hossain A, Goswami D, Nahar K, Alam K, Ahmed N, Naheed A, Nair GB, Luby S, Breiman RF. Bacteremic typhoid fever in children in an urban slum, Bangladesh. Emerg Infect Dis 2005;11:326-9. [PubMed]
37. Brown JC, Shanahan PM, Jesudason MV, Thomson CJ, Amyes SG. Mutations responsible for reduced susceptibility to 4-quinolones in clinical isolates of multi-resistant Salmonella typhi in India. J Antimicrob Chemother 1996;37:891-900. [PubMed]
38. Brown JD, Duong Hong M, Rhoades ER. Chloramphenicol-resistant Salmonella typhi in Saigon. JAMA 1975;231:162-6. [PubMed]
39. Brown NM, Millar MR, Frost JA, Rowe B. Ciprofloxacin resistance in Salmonella paratyphi A. J Antimicrob Chemother 1994;33:1258-9. [PubMed]
40. Bryan JP, Rocha H, Scheld WM. Problems in salmonellosis: rationale for clinical trials with newer beta-lactam agents and quinolones. Rev Infect Dis 1986;8:189-207. [PubMed]
41. Buczko GB, McLean J. Typhoid fever associated with adult respiratory distress syndrome. Chest 1994;105:1873-4. [PubMed]
42. Burkhardt JE, Walterspiel JN, Schaad UB. Quinolone arthropathy in animals versus children. Clin Infect Dis 1997;25:1196-204. [PubMed]
43. Butler T, Frenck RW, Johnson RB, Khakhria R. In vitro effects of azithromycin on Salmonella typhi: early inhibition by concentrations less than the MIC and reduction of MIC by alkaline pH and small inocula. J Antimicrob Chemother 2001;47:455-8. [PubMed]
44. Butler T, Sridhar CB, Daga MK, Pathak K, Pandit RB, Khakhria R, Potkar CN, Zelasky MT, Johnson RB. Treatment of typhoid fever with azithromycin versus chloramphenicol in a randomized multicentre trial in India. J Antimicrob Chemother 1999;44:243-50. [PubMed]
45. Butler T, Ho M, Acharya G, Tiwari M, Gallati H. Interleukin-6, gamma interferon, and tumor necrosis factor receptors in typhoid fever related to outcome of antimicrobial therapy. Antimicrob Agents Chemother 1993;37:2418-21. [PubMed]
46. Butler T, Islam A, Kabir I, Jones PK. Patterns of morbidity and mortality in typhoid fever dependent on age and gender: review of 552 hospitalized patients with diarrhea. Rev Infect Dis 1991;13:85-90. [PubMed]
47. Butler T, Knight J, Nath SK, Speelman P, Roy SK, Azad MA. Typhoid fever complicated by intestinal perforation: a persisting fatal disease requiring surgical management. Rev Infect Dis 1985;7:244-56.[PubMed]
48. Butler T, Bell WR, Levin J, Linh NN, Arnold K. Typhoid fever. Studies of blood coagulation, bacteremia, and endotoxemia. Arch Intern Med 1978;138:407-10.[PubMed]
49. Butler T, Linh NN, Arnold K, Adickman MD, Chau DM, Muoi MM. Therapy of antimicrobial-resistant typhoid fever. Antimicrob Agents Chemother 1977;11:645-50.[PubMed]
50. Butler T, Linh NN, Arnold K, Pollack M. Chloramphenicol-resistant typhoid fever in Vietnam associated with R factor. Lancet 1973;2:983-5. [PubMed]
51. Butt T, Ahmad RN, Mahmood A, Zaidi S. Ciprofloxacin treatment failure in typhoid fever case, Pakistan. Emerg Infect Dis 2003;9:1621-2. [PubMed]
52. Caksen H, Oner AF, Arslan S, Koseoglu B, Harman M, Atas B, Abuhandan M. Splenic abscess, pleural effusion and severe anemia caused by Salmonella typhi. Kobe J Med Sci 2000;46:201-4. [PubMed]
53. Calder JF. Chloramphenicol resistance in typhoid. Br Med J 1972;3:645. [PubMed]
54. Cao XT, Kneen R, Nguyen TA, Truong DL, White NJ, Parry CM. A comparative study of ofloxacin and cefixime for treatment of typhoid fever in children. The Dong Nai Pediatric Center Typhoid Study Group. Pediatr Infect Dis J 1999;18:245-8. [PubMed]
55. Carbon C, Weber P, Levy M, Boussougant Y, Cerf M. Short-term ciprofloxacin therapy for typhoid fever. J Infect Dis 1987;155:833. [PubMed]
56. Carvell JE, Maclarnon JC. Chronic osteomyelitis of the thoracic spine due to Salmonella typhi: a case report. Spine 1981;6:527-30. [PubMed]
57. Chaicumpa W, Ruangkunaporn Y, Burr D, Chongsa-Nguan M, Echeverria P. Diagnosis of typhoid fever by detection of Salmonella typhi antigen in urine. J Clin Microbiol 1992;30:2513-5. [PubMed]
58. Chande C, Shrikhande S, Kapale S, Agrawal S, Fule RP. Change in antimicrobial resistance pattern of Salmonella Typhi in central India. Indian J Med Res 2002;115:248-50. [PubMed]
59. Chang HR, Vladoianu IR, Pechere JC. Effects of ampicillin, ceftriaxone, chloramphenicol, pefloxacin and trimethoprim-sulphamethoxazole on Salmonella typhi within human monocyte-derived macrophages. J Antimicrob Chemother 1990;26:689-94. [PubMed]
60. Cheesbrough JS, Mwema FI, Green SD, Tillotson GS. Quinolones in children with invasive salmonellosis. Lancet 1991;338:127. [PubMed]
61. Chien YH, Lee PI, Huang LM, Lee CY, Lin DT, Lin KH. Typhoid fever presenting as infection-associated hemophagocytic syndrome: report of one case. Acta Paediatr Taiwan 1999;40:339-40. [PubMed]
62. Chinh NT, Parry CM, Ly NT, Ha HD, Thong MX, Diep TS, Wain J, White NJ, Farrar JJ. A randomized controlled comparison of azithromycin and ofloxacin for treatment of multidrug-resistant or nalidixic acid-resistant enteric fever. Antimicrob Agents Chemother 2000;44:1855-9. [PubMed]
63. Chiu S, Chiu CH, Lin TY, Luo CC, Jaing TH. Septic arthritis of the hip caused by Salmonella typhi. Ann Trop Paediatr 2001;21:88-90. [PubMed]
64. Choo KE, Davis TM, Ismail A, Tuan Ibrahim TA, Ghazali WN. Rapid and reliable serological diagnosis of enteric fever: comparative sensitivity and specificity of Typhidot and Typhidot-M tests in febrile Malaysian children. Acta Trop 1999;72:175-83. [PubMed]
65. Christie AB. Anonymous Infectious Diseases: Epidemiology and Clinical Practice. 3rd ed. Edinburgh: Churchill Livingstone, 1984, Typhoid and paratyphoid fevers. p. 47-102.
66. Cobos JA, Calhoun JH, Mader JT. Salmonella typhi osteomyelitis in a nonsickle cell patient. A case report. Clin Orthop 1993;288:277-81. [PubMed]
67. Collazos J, Mayo J, Martinez E, Blanco MS. Muscle infections caused by Salmonella species: case report and review. Clin Infect Dis 1999;29:673-7. [PubMed]
68. Connerton P, Wain J, Hien TT, et al. Epidemic typhoid in vietnam: molecular typing of multiple-antibiotic-resistant Salmonella enterica serotype typhi from four outbreaks. J Clin Microbiol 2000;38:895-7. [PubMed]
69. Connerton P, Wain J, Hien TT, Ali T, Parry C, Chinh NT, Vinh H, Ho VA, Diep TS, Day NP, White NJ, Dougan G, Farrar JJ. An outbreak of multiresistant Salmonella typhi in South Africa. Q J Med 1992;82:91-100. [PubMed]
70. Corrado ML, DuPont HL, Cooperstock M, Fekety R, Murray DM. Evaluation of new anti-infective drugs for the treatment of typhoid fever. Infectious Diseases Society of America and the Food and Drug Administration. Clin Infect Dis 1992;15 Suppl 1:S236-40. [PubMed]
71. Crump JA, Barrett TJ, Nelson JT, Angulo FJ. Reevaluating fluoroquinolone breakpoints for Salmonella enterica serotype Typhi and for non-Typhi salmonellae. Clin Infect Dis 2003;37:75-81. [PubMed]
72. Daga MK, Sarin K, Sarkar R. A study of culture positive multidrug resistant enteric fever--changing pattern and emerging resistance to ciprofloxacin. J Assoc Physicians India 1994;42:599-600. [PubMed]
73. Dakdouki GK, Bizri AR. Rhabdomyolysis and Salmonella typhi infection: case report and review of the literature. J Med Liban 2003;51:143-7. [PubMed]
74. Dance D, Richens JE, Ho M, Acharya G, Pokhrel B, Tuladhar NR. Blood and bone marrow cultures in enteric fever. J Clin Pathol 1991;44:1038. [PubMed]
75. Datta N, Richards H, Datta C. Salmonella typhi in vivo acquires resistance to both chloramphenicol and co-trimoxazole. Lancet 1981;1:1181-3. [PubMed]
76. De Matteis A, Armani G. Salmonella typhi pneumonia without intestinal lesions. J Pathol Bacteriol 1967;94:464-7. [PubMed]
77. Declercq J, Verhaegen J, Verbist L, Lammens J, Stuyck J, Fabry G. Salmonella typhi osteomyelitis. Arch Orthop Trauma Surg 1994;113:232-4. [PubMed]
78. Doherty CP, Saha SK, Cutting WA. Typhoid fever, ciprofloxacin and growth in young children. Ann Trop Paediatr 2000;20:297-303. [PubMed]
79. Dromigny JA, Perrier-Gros-Claude JD. Antimicrobial resistance of Salmonella enterica serotype Typhi in Dakar, Senegal. Clin Infect Dis 2003;37:465-6. [PubMed]
80. du Plessis JP, Govendrageloo K, Levin SE. Right-sided endocarditis due to Salmonella typhi. Pediatr Cardiol 1997;18:443-4. [PubMed]
81. Duncan ME, Perine PL, Krause DW. Pelvic infection caused by Salmonella typhi. Two unusual cases. East Afr Med J 1981;58:703-7. [PubMed]
82. Duong NM, Chau NVV, Anh DCV, Hoa NT, Tam DTH, Ho VA, Hai DT, Hien TT, Arnold K. Short course fleroxacin in the treatment of typhoid fever. JAMA South East Asia 1995;11:21-5.
83. DuPont HL, Hornick RB, Weiss CF, Snyder MJ, Woodward TE. Evaluation of chloramphenicol acid succinate therapy of induced typhoid fever and rocky mountain spotted fever. N Engl J Med 1970;282:53-7. [PubMed]
84. Dutta P, Rasaily R, Saha MR, et al. Ciprofloxacin for treatment of severe typhoid fever in children. Antimicrob Agents Chemother 1993;37:1197-9. [PubMed]
85. Edelman R, Levine MM. Summary of an international workshop on typhoid fever. Rev Infect Dis 1986;8:329-49. [PubMed]
86. El Ramli AH. Choramphenicol in treatment of enteric fever. Lancet 1950;1:618-20.[PubMed]
87. El Sherbini A. An outbreak of typhoid fever resistant to chloramphenicol and other drugs in Gharbeya Governorate in Egypt .J Trop Pediatr 1991;38:331-4. [PubMed]
88. El-Newihi HM, Alamy ME, Reynolds TB. Salmonella hepatitis: analysis of 27 cases and comparison with acute viral hepatitis. Hepatology 1996;24:516-9. [PubMed]
89. Engels EA, Falagas ME, Lau J, Bennish ML. Typhoid fever vaccines: a meta-analysis of studies on efficacy and toxicity. BMJ 1998;316:110-6. [PubMed]
90. Erdem B, Ercis S, Hascelik G, Gur D, Aysev AD. Antimicrobial resistance of Salmonella enterica group C strains isolated from humans in Turkey, 2000-2002. Int J Antimicrob Agents 2005;26:33-7. [PubMed]
91. Eykyn SJ, Williams H. Treatment of multiresistant Salmonella typhi with oral ciprofloxacin. Lancet 1987;2:1407-8. [PubMed]
92. Fame TM, Engelhard D, Riley HD, Jr. Hemophagocytosis accompanying typhoid fever. Pediatr Infect Dis 1986;5:367-9. [PubMed]
93. Ferreccio C, Morris JG Jr, Valdivieso C, Prenzel I, Sotomayor V, Drusano GL, Levine MM. Efficacy of ciprofloxacin in the treatment of chronic typhoid carriers. J Infect Dis 1988;157:1235-9.[PubMed]
94. Frenck RW Jr, Mansour A, Nakhla I, Sultan Y, Putnam S, Wierzba T, Morsy M, Knirsch C. Short-course azithromycin for the treatment of uncomplicated typhoid fever in children and adolescents. Clin Infect Dis 2004;38:951-7. [PubMed]
95. Frenck RW Jr, Nakhla I, Sultan Y, Bassily SB, Girgis YF, David J, Butler TC, Girgis NI, Morsy M. Azithromycin versus ceftriaxone for the treatment of uncomplicated typhoid fever in children. Clin Infect Dis 2000;31:1134-8. [PubMed]
96. Gargalianos P, Jackson PT, Herzog C, Geddes AM. Trimethoprim in enteric fever. J Antimicrob Chemother 1986;18:277-9. [PubMed]
97. Gasem MH, Keuter M, Dolmans WM, Van Der Ven-Jongekrijg J, Djokomoeljanto R, Van Der Meer JW. Persistence of Salmonellae in blood and bone marrow: randomized controlled trial comparing ciprofloxacin and chloramphenicol treatments against enteric fever. Antimicrob Agents Chemother 2003;47:1727-31. [PubMed]
98. Geddes AM, Goodall JA. Chloramphenicol resistance in the typhoid bacillus. Br Med J 1972;3:525. [PubMed]
99. Ghadage DP, Bal AM. Infective endocarditis due to an unusual serotype of Salmonella. Indian Heart J 2001;53:350-1. [PubMed]
100. Ghosh JB, Samanta S. Venous thrombosis in enteric fever. Indian Pediatr 1994;31:230-1. [PubMed]
101. Gilman RH, Islam S, Rabbani H, Ghosh H. Identification of gallbladder typhoid carriers by a string device. Lancet 1979;1:795-6. [PubMed]
102. Gilman RH, Terminel M, Levine MM, Hernandez-Mendoza P, Hornick RB. Relative efficacy of blood, urine, rectal swab, bone-marrow, and rose-spot cultures for recovery of Salmonella typhi in typhoid fever. Lancet 1975;1:1211-3. [PubMed]
103. Girgis NI, Butler T, Frenck RW, Sultan Y, Brown FM, Tribble D, Khakhria R. Azithromycin versus ciprofloxacin for treatment of uncomplicated typhoid fever in a randomized trial in Egypt that included patients with multidrug resistance. Antimicrob Agents Chemother 1999;43:1441-4.[PubMed]
104. Girgis NI, Sultan Y, Hammad O, Farid Z. Comparison of the efficacy, safety and cost of cefixime, ceftriaxone and aztreonam in the treatment of multidrug-resistant Salmonella typhi septicemia in children. Pediatr Infect Dis J 1995;14:603-5. [PubMed]
105. Girgis NI, Tribble DR, Sultan Y, Farid Z. Short course chemotherapy with cefixime in children with multidrug-resistant Salmonella typhi Septicaemia. J Trop Pediatr 1995;41:364-5. [PubMed]
106. Goldstein FW, Chumpitaz JC, Guevara JM, Papadopoulou B, Acar JF, Vieu JF. Plasmid-mediated resistance to multiple antibiotics in Salmonella typhi. J Infect Dis 1986;153:261-6. [PubMed]
107. Gonen I, Akcam FZ. Meningitis owing to an unusual aetiological agent in an adult: Salmonella typhi. Scand J Infect Dis 2005;37:319-20. [PubMed]
108. Gonzalez-Cortes A, Bessudo D, Sanchez-Leyva R, Fragoso R, Hinojosa M, Becerril P. Water-borne transmission of chloramphenicol-resistant Salmonella typhi in Mexico. Lancet 1973;2:605-7. [PubMed]
109. Gosbell I, Jones PD, Matthews A, Yeo B. Surgical presentation of hepatobiliary disease due to Salmonella typhi. Aust N Z J Surg 1995;65:898-9.[PubMed]
110. Green SD, Ilunga FM, Numbi A, Cheesbrough JS, Tillotson GS. An open study of ciprofloxacin for the treatment of proven or suspected extra intestinal salmonellosis in African children: a preliminary report. Adv Antimicrob Antineoplast Chemother 1992; 11:181-7.
111. Green SD, Cheesbrough JS. Salmonella bacteraemia among young children at a rural hospital in western Zaire. Ann Trop Paediatr 1993;13:45-53. [PubMed]
112. Griggs DJ, Hall MC, Jin YF, Piddock LJ. Quinolone resistance in veterinary isolates of Salmonella. J Antimicrob Chemother 1994;33:1173-89. [PubMed]
113. Gulati S, Marwaha RK, Prakash D, Ayyagari A, Singhi S, Kumar L, Singhi P, Walia BN. Multi-drug-resistant Salmonella typhi--a need for therapeutic reappraisal. Ann Trop Paediatr 1992;12:137-41.[PubMed]
114. Gupta A. Multidrug-resistant typhoid fever in children: epidemiology and therapeutic approach. Pediatr Infect Dis J 1994;13:134-40. [PubMed]
115. Harnett N, McLeod S, AuYong Y, Brown S, Krishnan C. Emergence in Ontario, Canada, of multiresistant Salmonella typhi from South Asia. Lancet 1992;340:177.[PubMed]
116. Herbert DA, Ruskin J. Salmonella typhi epidural abscess occurring 47 years after typhoid fever. Case report. J Neurosurg 1982;57:719-21. [PubMed]
117. Hermans PW, Saha SK, van Leeuwen WJ, Verbrugh HA, van Belkum A, Goessens WH. Molecular typing of Salmonella typhi strains from Dhaka (Bangladesh) and development of DNA probes identifying plasmid-encoded multidrug-resistant isolates. J Clin Microbiol 1996;34:1373-9. [PubMed]
118. Herzog C, Wood MJ. Chloramphenicol resistance in Salmonella typhi. Lancet 1982;2:658-9. [PubMed]
119. Hoffman SL, GT Strickland, editors. Hunter's Tropical Medicine. 6th ed. Philadelphia: WB Saunders, 1984, Typhoid fever. p. 282-96.
120. Hoffman SL, Edman DC, Punjabi NH, Lesmana M, Cholid A, Sundah S, Harahap J. Bone marrow aspirate culture superior to streptokinase clot culture and 8 ml 1:10 blood-to-broth ratio blood culture for diagnosis of typhoid fever. Am J Trop Med Hyg 1986;35:836-9. [PubMed]
121. Hoffman SL, Punjabi NH, Kumala S, Moechtar MA, Pulungsih SP, Rivai AR, Rockhill RC, Woodward TE, Loedin AA. Reduction of mortality in chloramphenicol-treated severe typhoid fever by high-dose dexamethasone. N Engl J Med 1984;310:82-8. [PubMed]
122. Hoffman SL, Punjabi NH, Rockhill RC, Sutomo A, Rivai AR, Pulungsih SP. Duodenal string-capsule culture compared with bone-marrow, blood, and rectal-swab cultures for diagnosing typhoid and paratyphoid fever. J Infect Dis 1984;149:157-61. [PubMed]
123. Hohmann EL, Oletta CA, Killeen KP, Miller SI. phoP/phoQ-deleted Salmonella typhi (Ty800) is a safe and immunogenic single-dose typhoid fever vaccine in volunteers. J Infect Dis 1996;173:1408-14. [PubMed]
124. Horowitz H, Carbonaro CA. Inhibition of the Salmonella typhi oral vaccine strain, Ty21a, by mefloquine and chloroquine. J Infect Dis 1992;166:1462-4. [PubMed]
125. House D, Wain J, Ho VA, Diep TS, Chinh NT, Bay PV, Vinh H, Duc M, Parry CM, Dougan G, White NJ, Hien TT, Farrar JJ.Serology of typhoid fever in an area of endemicity and its relevance to diagnosis. J Clin Microbiol 2001;39:1002-7. [PubMed]
126. Hsu CC, Chen WJ, Chen SY, Chiang WC, Hsueh PR. Fatal septicemia and pyomyositis caused by Salmonella typhi. Clin Infect Dis 2004;39:1547-9. [PubMed]
127. Huang DB, DuPont HL. Problem pathogens: extra-intestinal complications of Salmonella enterica serotype Typhi infection. Lancet Infect Dis 2005;5:341-8.
128. Islam A, Butler T, Kabir I, Alam NH. Treatment of typhoid fever with ceftriaxone for 5 days or chloramphenicol for 14 days: a randomized clinical trial. Antimicrob Agents Chemother 1993;37:1572-5.[PubMed]
129. Ivanoff B. Typhoid fever: Global situation and WHO recommendations. SE Asian J Trop Med Publ Hlth 1995;26:1-6.
130. Jagadish K, Patwari AK, Sarin SK, Prakash C, Srivastava DK, Anand VK. Hepatic manifestations in typhoid fever. Indian Pediatr 1994;31:807-11. [PubMed]
131. Jain KC, Mahapatra AK. Subdural empyema due to salmonella infection. Pediatr Neurosurg 1998;28:89-90. [PubMed]
132. Jaussaud R, Brasme L, Vernet-Garnier V, Deville JF. Splenic abscess complicating Salmonella typhi infection. Eur J Clin Microbiol Infect Dis 2000;19:399-400.[PubMed]
133. Jones DA, Kudlac H, Edwards IR. Pivmecillinam and relapse of typhoid fever. J Infect Dis 1982;145:773. [PubMed]
134. Kager PA, Rietra PJ. Splenic abscess due to Salmonella typhi. Trop Geogr Med 1982;34:375-7. [PubMed]
135. Kamat SA. Evaluation of therapeutic efficacy of trimethoprim-sulphamethoxazole and chloramphenicol in enteric fever. Br Med J 1970;3:320-2. [PubMed]
136. Karunanayake L, Atukorala SD. Enteric fever caused by Salmonella isolates with decreased susceptibility to ciprofloxacin. Ceylon Med J 2004;49:137-8. [PubMed]
137. Khan GQ, Kadri SM, Hassan G, Shahid IT, Gazanfar A, Kak M, Showkat H. Salmonella typhi endocarditis: a case report. J Clin Pathol 2003;56:801-2. [PubMed]
138. Khosla SN, Anand A, Singh U, Khosla A. Haematological profile in typhoid fever. Trop Doct 1995;25:156-8. [PubMed]
139. Klugman KP, Koornhof HJ, Robbins JB, Le Cam NN. Immunogenicity, efficacy and serological correlate of protection of Salmonella typhi Vi capsular polysaccharide vaccine three years after immunization. Vaccine 1996;14:435-8. [PubMed]
140. Kubin R. Safety and efficacy of ciprofloxacin in paediatric patients--review. Infection 1993;21:413-21. [PubMed]
141. Kumar AS, Legori M, Sathy N, Mathew R. Furazolidone in typhoid fever--correlation of clinical efficacy with serum bactericidal activity. Indian Pediatr 1995;32:533-8. [PubMed]
142. Laloum E, Zeller V, Graff W, Aerts J, Chazerain P, Mamoudy P, Ziza JM, Desplaces N. Salmonella typhi osteitis can mimic tuberculosis. A report of three cases. Joint Bone Spine 2005;72:171-4. [PubMed]
143. Lambotte O, Debord T, Castagne C, Roue R. Unusual presentation of typhoid fever: cutaneous vasculitis, pancreatitis, and splenic abscess. J Infect 2001;42:161-2. [PubMed]
144. Lasserre R, Sangalang RP, Santiago L. Three-day treatment of typhoid fever with two different doses of ceftriaxone, compared to 14-day therapy with chloramphenicol: a randomized trial. J Antimicrob Chemother 1991;28:765-72.[PubMed]
145. Lecour H, Santos L, Oliveira M, Pereira A, Simoes J. Salmonella typhi meningitis. Scand J Infect Dis 1994;26:103-4. [PubMed]
146. Leung D, Venkatesan P, Boswell T, Innes JA, Wood MJ. Treatment of typhoid in pregnancy. Lancet 1995;346:648. [PubMed]
147. Levine MM, Ferreccio C, Black RE, Germanier R. Large-scale field trial of Ty21a live oral typhoid vaccine in enteric-coated capsule formulation. Lancet 1987;1:1049-52. [PubMed]
148. Lim PL, Tam FC, Cheong YM, Jegathesan M. One-step 2-minute test to detect typhoid-specific antibodies based on particle separation in tubes. J Clin Microbiol 1998;36:2271-8. [PubMed]
149. Lin FY, Ho VA, Khiem HB, Trach DD, Bay PV, Thanh TC, Kossaczka Z, Bryla DA, Shiloach J, Robbins JB, Schneerson R, Szu SC. The efficacy of a Salmonella typhi Vi conjugate vaccine in two-to-five-year-old children. N Engl J Med 2001;344:1263-9. [PubMed]
150. Lin FY, Vo AH, Phan VB, Nguyen TT, Bryla D, Tran CT, Ha BK, Dang DT, Robbins JB. The epidemiology of typhoid fever in the Dong Thap Province, Mekong Delta region of Vietnam. Am J Trop Med Hyg 2000;62:644-8. [PubMed]
151. Luby SP, Faizan MK, Fisher-Hoch SP, Syed A, Mintz ED, Bhutta ZA, McCormick JB. Risk factors for typhoid fever in an endemic setting, Karachi, Pakistan. Epidemiol Infect 1998;120:129-38. [PubMed]
152. Luxemburger C, Chau MC, Mai NL, Wain J, Tran TH, Simpson JA, Le HK, Nguyen TT, White NJ, Farrar JJ. Risk factors for typhoid fever in the Mekong delta, southern Viet Nam: a case-control study. Trans R Soc Trop Med Hyg 2001;95:19-23. [PubMed]
153. Machiz S, Gordon J, Block N, Politano VA. Salmonella typhosa urinary tract infection and xanthogranulomatous pyelonephritis. Case report and review of literature. J Fla Med Assoc 1974;61:703-5. [PubMed]
154. Madhulika U, Harish BN, Parija SC. Current pattern in antimicrobial susceptibility of Salmonella Typhi isolates in Pondicherry. Indian J Med Res 2004;120:111-4.[PubMed]
155. Malik AS. Complications of bacteriologically confirmed typhoid fever in children. J Trop Pediatr 2002;48:102-8. [PubMed]
156. Mandal BK. Treatment of multiresistant typhoid fever. Lancet 1990;336:1383. [PubMed]
157. Mansoor IA. Typhoid osteomyelitis of the calcaneus due to direct inoculation. J Bone Joint Surg Am 1967;49:732-4. [PubMed]
158. Mathai E, John TJ, Rani M, Mathai D, Chacko N, Nath V, Cherian AM. Significance of Salmonella typhi bacteriuria. J Clin Microbiol 1995;33:1791-2. [PubMed]
159. McClelland M, Sanderson KE, Spieth J, Clifton SW, Latreille P, Courtney L, Porwollik S, Ali J, Dante M, Du F, Hou S, Layman D, Leonard S, Nguyen C, Scott K, Holmes A, Grewal N, Mulvaney E, Ryan E, Sun H, Florea L, Miller W, Stoneking T, Nhan M, Waterston R, Wilson RK. Complete genome sequence of Salmonella enterica serovar Typhimurium LT2. Nature 2001;413:852-6. [PubMed]
160. McCurdy PR. Plasma concentration of chloramphenicol and bone marrow suppression. Blood 1963;21:323-5.
161. McKendrick MW, Geddes AM, Farrell ID. Trimethoprim in enteric fever. Br Med J (Clin Res Ed) 1981;282:364. [PubMed]
162. Mermin JH, Villar R, Carpenter J, Roberts L, Samaridden A, Gasanova L, Lomakina S, Bopp C, Hutwagner L, Mead P, Ross B, Mintz ED. A massive epidemic of multidrug-resistant typhoid fever in Tajikistan associated with consumption of municipal water. J Infect Dis 1999; Jun;179:1416-22. [PubMed]
163. Mikhail IA, Haberberger RL, Farid Z, Girgis NI, Woody JN. Antibiotic-multiresistant Salmonella typhi in Egypt. Trans R Soc Trop Med Hyg 1989;83:120. [PubMed]
164. Mirza SH, Beeching NJ, Hart CA. The prevalence and clinical features of multi-drug resistant Salmonella typhi infections in Baluchistan, Pakistan. Ann Trop Med Parasitol 1995;89:515-9. [PubMed]
165. Mishra S, Pattnaik D, Mahapatra A, Swain B. Pleural empyema due to S. typhi: a case report. Indian J Pathol Microbiol 2004;47:75-6. [PubMed]
166. Mishra S, Patwari AK, Anand VK, Pillai PK, Aneja S, Chandra J, Sharma D. Multidrug resistant typhoid fever: therapeutic considerations. Indian Pediatr 1992;29:443-8. [PubMed]
167. Mokhobo KP. Typhoid cardiac involvement. S Afr Med J 1975;49:55-6. [PubMed]
168. Morelli G, Mazzoli S, Tortoli E, Simonetti MT, Perruna S, Postiglione A. Fluoroquinolones versus chloramphenicol in the therapy of typhoid fever: a clinical and microbiological study. Therapeutic Research 1992;52:532-42.
169. Mourad AS, Metwally M, el Deen AN, Threlfall EJ, Rowe B, Mapes T, Hedstrom R, Bourgeois AL, Murphy JR. Multiple-drug-resistant Salmonella typhi. Clin Infect Dis 1993;17:135-6. [PubMed]
170. Nazar HS, Rabbani A, Riaz A, Anwar J. Presentation of typhoid fever patients in Hazara Division and response to different treatment regimens. J Ayub Med Coll Abbottabad 2005;17:67-9. [PubMed]
171. Orji MU, Onuigbo HC, Mbata TI. Isolation of Salmonella from poultry droppings and other environmental sources in Awka, Nigeria. Int J Infect Dis 2005;9:86-9.[PubMed]
172. Pace F, Fanfarillo F, Giorgino F, Baratta L. Salmonella enteritidis pericarditis: case report and review of the literature. Ann Ital Med Int 2002;17:189-92. [PubMed]
173. Panhotra BR, Saxena AK, Al-Ghamdi AM. Emerging nalidixic acid and ciprofloxacin resistance in non-typhoidal Salmonella isolated from patients having acute diarrhoeal disease. Ann Saudi Med 2004;24:332-6. [PubMed]
174. Paniker CK, Vimala KN. Transferable chloramphenicol resistance in Salmonella typhi. Nature 1972;239:109-10. [PubMed]
175. Parkhill J, Dougan G, James KD, Thomson NR, Pickard D, Wain J, Churcher C, Mungall KL, Bentley SD, Holden MT, Sebaihia M, Baker S, Basham D, Brooks K, Chillingworth T, Connerton P, Cronin A, Davis P, Davies RM, Dowd L, White N, Farrar J, Feltwell T, Hamlin N, Haque A, Hien TT, Holroyd S, Jagels K, Krogh A, Larsen TS, Leather S, Moule S, O'Gaora P, Parry C, Quail M, Rutherford K, Simmonds M, Skelton J, Stevens K, Whitehead S, Barrell BG. Complete genome sequence of a multiple drug resistant Salmonella enterica serovar Typhi CT18. Nature 2001;413:848-52. [PubMed]
176. Parry C, Wain J, Chinh NT, Vinh H, Farrar JJ. Quinolone-resistant Salmonella typhi in Vietnam. Lancet 1998;351:1289. [PubMed]
177. Parry CM, Hien TT, Dougan G, White NJ, Farrar JJ. Typhoid fever. N Engl J Med 2002;347:1770-82. [PubMed]
178. Parry CM, Hoa NT, Diep TS, Wain J, Chinh NT, Vinh H, Hien TT, White NJ, Farrar JJ. Value of a single-tube widal test in diagnosis of typhoid fever in Vietnam. J Clin Microbiol 1999;37:2882-6. [PubMed]
179. Parry SD, Stansfield R, Jelley D, Gregory W, Phillips E, Barton JR, Welfare MR. Is irritable bowel syndrome more common in patients presenting with bacterial gastroenteritis? A community-based, case-control study. Am J Gastroenterol 2003;98:327-31. [PubMed]
180. Phillips WE. Treatment of chronic typhoid carriers with ampicillin. JAMA 1971;217:913-5. [PubMed]
181. Pillay N, Adams EB, North-Coombes D. Comparative trial of amoxycillin and chloramphenicol in treatment of typhoid fever in adults. Lancet 1975;2:333-4.[PubMed]
182. Plotkin SA, Bouveret-Le Cam N. A new typhoid vaccine composed of the Vi capsular polysaccharide. Arch Intern Med 1995;155:2293-9. [PubMed]
183. Prabha A, Mohanan, Pereira P, Raghuveer CV. Myocarditis in enteric fever. Indian J Med Sci 1995;49:28-31. [PubMed]
184. Pradhan KM, Arora NK, Jena A, Susheela AK, Bhan MK. Safety of ciprofloxacin therapy in children: magnetic resonance images, body fluid levels of fluoride and linear growth. Acta Paediatr 1995;84:555-60. [PubMed]
185. Prakash P, Mishra OP, Singh AK, Gulati AK, Nath G. Evaluation of nested PCR in diagnosis of typhoid fever. J Clin Microbiol 2005;43:431-2. [PubMed]
186. Rabbani MW, Iqbal I, Malik MS. A comparative study of cefixime and chloramphenicol in children with typhoid fever. J Pak Med Assoc 1998;48:163-4. [PubMed]
187. Rahman MM, Haq JA, Morshed MA, Rahman MA. Salmonella enterica serovar Typhi with decreased susceptibility to ciprofloxacin--an emerging problem in Bangladesh. Int J Antimicrob Agents 2005;25:345-6. [PubMed]
188. Rajeshwari K, Yadav S, Puri RK, Khanijo CM, Sethi Y. Cerebritis in typhoid fever. Indian Pediatr 1995;32:1305-7. [PubMed]
189. Rao PS, Rajashekar V, Varghese GK, Shivananda PG. Emergence of multidrug-resistant Salmonella typhi in rural southern India. Am J Trop Med Hyg 1993;48:108-11. [PubMed]
190. Reller ME, Olsen SJ, Kressel AB, Moon TD, Kubota KA, Adcock MP, Nowicki SF, Mintz ED. Sexual transmission of typhoid fever: a multistate outbreak among men who have sex with men. Clin Infect Dis 2003;37:141-4. [PubMed]
191. Renuka K, Kapil A, Kabra SK, Wig N, Das BK, Prasad VV, Chaudhry R, Seth P. Reduced susceptibility to ciprofloxacin and gyra gene mutation in North Indian strains of Salmonella enterica serotype Typhi and serotype Paratyphi A. Microb Drug Resist 2004;10:146-53. [PubMed]
192. Richens J, Smith T, Mylius T, Spooner V. An algorithm for the clinical differentiation of malaria and typhoid: a preliminary communication. P N G Med J 1992;35:298-302. [PubMed]
193. Robertson RP, Wahab MF, Raasch FO. Evaluation of chloramphenicol and ampicillin in salmonella enteric fever. N Engl J Med 1968;278:171-6. [PubMed]
194. Rowe B, Ward LR, Threlfall EJ. Ciprofloxacin-resistant Salmonella typhi in the UK. Lancet 1995;346:1302. [PubMed]
195. Rowe B, Ward LR, Threlfall EJ. Treatment of multiresistant typhoid fever. Lancet 1991;337:1422. [PubMed]
196. Rowe B, Threlfall EJ, Ward LR. Does chloramphenicol remain the drug of choice for typhoid?. Epidemiol Infect 1987;98:379-83. [PubMed]
197. Rowe B, Frost JA, Threlfall EJ, Ward LR. Spread of a multiresistant clone of Salmonella typhimurium phage type 66/122 in South-East Asia and the Middle East. Lancet 1980;1:1070-1. [PubMed]
198. Rowland HA. The complications of typhoid fever. J Trop Med Hyg 1961;64:143-52. [PubMed]
199. Roy SK, Speelman P, Butler T, Nath S, Rahman H, Stoll BJ. Diarrhea associated with typhoid fever. J Infect Dis 1985;151:1138-43. [PubMed]
200. Rubin FA, McWhirter PD, Burr D, Punjabi NH, Lane E, Kumala S, Sudarmono P, Pulungsih SP, Lesmana M, Tjaniadi P, et al. Rapid diagnosis of typhoid fever through identification of Salmonella typhi within 18 hours of specimen acquisition by culture of the mononuclear cell-platelet fraction of blood. J Clin Microbiol 1990;28:825-7. [PubMed]
201. Saha SK, Darmstadt GL, Baqui AH, Hanif M, Ruhulamin M, Santosham M, Nagatake T, Black RE. Rapid identification and antibiotic susceptibility testing of Salmonella enterica serovar Typhi isolated from blood: implications for therapy. J Clin Microbiol 2001;39:3583-5. [PubMed]
202. Saha SK, Talukder SY, Islam M, Saha S. A highly ceftriaxone-resistant Salmonella typhi in Bangladesh. Pediatr Infect Dis J 1999;18:387. [PubMed]
203. Salerno-Goncalves R, Fernandez-Vina M, Lewinsohn DM, Sztein MB. Identification of a human HLA-E-restricted CD8+ T cell subset in volunteers immunized with Salmonella enterica serovar Typhi strain Ty21a typhoid vaccine. J Immunol 2004;173:5852-62. [PubMed]
204. Sammalkorpi K, Lahdevirta J, Makela T, Rostila T. Treatment of chronic Salmonella carriers with ciprofloxacin. Lancet 1987;2:164-5.[PubMed]
205. Sanchez MM, Cardona-Castro NM. Development and evaluation of a PCR method for diagnosis of Salmonella enteric fever, based on DNA sequences of the hilA gene. Biomedica 2004;24:194-9. [PubMed]
206. Sarma PS, Durairaj P. Randomized treatment of patients with typhoid and paratyphoid fevers using norfloxacin or chloramphenicol. Trans R Soc Trop Med Hyg 1991;85:670-1. [PubMed]
207. Saxe JM, Cropsey R. Is operative management effective in treatment of perforated typhoid?. Am J Surg 2005;189:342-4. [PubMed]
208. Schaad UB. Use of the quinolones in paediatrics. Drugs 1993;45 Suppl 3:37-41. [PubMed]
209. Schwalbe RS, Hoge CW, Morris JG, Jr, O'Hanlon PN, Crawford RA, Gilligan PH. In vivo selection for transmissible drug resistance in Salmonella typhi during antimicrobial therapy. Antimicrob Agents Chemother 1990;34:161-3. [PubMed]
210. Schwartz E, Jenks NP, Shlim DR. 'Typhoid hepatitis' or typhoid fever and acute viral hepatitis. Trans R Soc Trop Med Hyg 1994;88:437-8. [PubMed]
211. Scragg JN, Rubidge CJ. Trimethoprim and sulphamethoxazole in typhoid fever in children. Br Med J 1971;3:738-41. [PubMed]
212. Secmeer G, Kanra G, Figen G, Akan O, Ceyhan M, Ecevit Z. Ofloxacin versus co-trimoxazole in the treatment of typhoid fever in children. Acta Paediatr Jpn 1997;39:218-21. [PubMed]
213. Sekar U, Srikanth P, Kindo AJ, Babu VP, Ramasubramanian V. Increase in minimum inhibitory concentration to quinolones and ceftriaxone in salmonellae causing enteric fever. J Commun Dis 2003;35:162-9. [PubMed]
214. Sethuraman S, Mahamood M, Kareem S. Furazolidone in multi-resistant childhood typhoid fever. Ann Trop Paediatr 1994;14:321-4. [PubMed]
215. Shadomy S, Espinel-Ingroff A, Gebhart RJ. In-vitro studies with SF 86-327, a new orally active allylamine derivative. Sabouraudia 1985;23:125-32. [PubMed]
216. Shakespeare WA, Davie D, Tonnerre C, Rubin MA, Strong M, Petti CA. Nalidixic acid-resistant Salmonella enterica serotype Typhi presenting as a primary psoas abscess: case report and review of the literature. J Clin Microbiol 2005;43:996-8. [PubMed]
217. Shanley DJ, Holmes SM. Salmonella typhi abscess in a craniopharyngioma: CT and MRI. Neuroradiology 1994;36:35-6. [PubMed]
218. Shann F, Linnemann V, Mackenzie A, Barker J, Gratten M, Crinis N. Absorption of chloramphenicol sodium succinate after intramuscular administration in children. N Engl J Med 1985;313:410-4. [PubMed]
219. Sharma AM, Sharma OP. Pulmonary manifestations of typhoid fever. Two case reports and a review of the literature. Chest 1992;101:1144-6. [PubMed]
220. Shwe TN, Nyein MM, Yi W, Mon A. Blood culture isolates from children admitted to Medical Unit III, Yangon Children's Hospital, 1998. Southeast Asian J Trop Med Public Health 2002;33:764-71. [PubMed]
221. Sitprija V, Pipantanagul V, Boonpucknavig V, Boonpucknavig S. Glomerulitis in typhoid fever. Ann Intern Med 1974;81:210-3. [PubMed]
222. Slinger R, Desjardins M, McCarthy AE, Ramotar K, Jessamine P, Guibord C, Toye B. Suboptimal clinical response to ciprofloxacin in patients with enteric fever due to Salmonella spp. with reduced fluoroquinolone susceptibility: a case series. BMC Infect Dis 2004;4:36. [PubMed]
223. Smith MD, Duong NM, Hoa NT, Wain J, Ha HD, Diep TS, Day NP, Hien TT, White NJ. Comparison of ofloxacin and ceftriaxone for short-course treatment of enteric fever. Antimicrob Agents Chemother 1994;38:1716-20. [PubMed]
224. Soe GB, Overturf GD. Treatment of typhoid fever and other systemic salmonelloses with cefotaxime, ceftriaxone, cefoperazone, and other newer cephalosporins. Rev Infect Dis 1987;9:719-36. [PubMed]
225. Sood S, Rishi P, Vohra H, Sharma S, Ganguly NK. Cellular immune response induced by Salmonella enterica serotype Typhi iron-regulated outer-membrane proteins at peripheral and mucosal levels. J Med Microbiol 2005;54:815-21. [PubMed]
226. Sood S, Kapil A, Das B, Jain Y, Kabra SK. Re-emergence of chloramphenicol-sensitive Salmonella typhi. Lancet 1999;353:1241-2. [PubMed]
227. Spika JS, Waterman SH, Hoo GW, St Louis ME, Pacer RE, James SM, Bissett ML, Mayer LW, Chiu JY, Hall B, et al. Chloramphenicol-resistant Salmonella newport traced through hamburger to dairy farms. A major persisting source of human salmonellosis in California. N Engl J Med 1987;316:565-70. [PubMed]
228. Sridhar CB, Kulkarni RD. Reassessment of frequency of occurrence of typhoid fever and cost efficacy analysis of antibiotic therapy. J Assoc Physicians India 1995;43:679-84. [PubMed]
229. Takkar VP, Kumar R, Takkar R, Khurana S. Resurgence of chloramphenicol sensitive Salmonella typhi. Indian Pediatr 1995;32:586-7. [PubMed]
230. Tarr PE, Kuppens L, Jones TC, Ivanoff B, Aparin PG, Heymann DL. Considerations regarding mass vaccination against typhoid fever as an adjunct to sanitation and public health measures: potential use in an epidemic in Tajikistan. Am J Trop Med Hyg 1999;61:163-70. [PubMed]
231. Taylor DE, Chumpitaz JC, Goldstein F. Variability of IncHI1 plasmids from Salmonella typhi with special reference to Peruvian plasmids encoding resistance to trimethoprim and other antibiotics. Antimicrob Agents Chemother 1985;28:452-5. [PubMed]
232. Taylor DN, Levine MM, Kuppens L, Ivanoff B. Why are typhoid vaccines not recommended for epidemic typhoid fever?. J Infect Dis 1999;180:2089-90.[PubMed]
233. Thong KL, Cheong YM, Puthucheary S, Koh CL, Pang T. Epidemiologic analysis of sporadic Salmonella typhi isolates and those from outbreaks by pulsed-field gel electrophoresis. J Clin Microbiol 1994;32:1135-41. [PubMed]
234. Threlfall EJ, Ward LR. Decreased susceptibility to ciprofloxacin in Salmonella enterica serotype typhi, United Kingdom. Emerg Infect Dis 2001;7:448-50. [PubMed]
235. Threlfall EJ, Ward LR, Skinner JA, Smith HR, Lacey S. Ciprofloxacin-resistant Salmonella typhi and treatment failure. Lancet 1999;353:1590-1. [PubMed]
236. Threlfall J, Ward L, Old D. Changing the nomenclature of Salmonella. Commun Dis Public Health 1999;2:156-7. [PubMed]
237. Ti TI, Monteiro EH, Lam S, Lee HS. Chloramphenicol concentrations in sera of patients with typhoid fever being treated with oral or intravenous preparation. Antimicrob Agents Chemother 1990;34:1809-11. [PubMed]
238. Tongia RK, Chowdhury MN. Endocarditis due to Salmonella typhi. Trop Geogr Med 1983;35:187-8. [PubMed]
239. Toth F, Szabo G, Abed R, Lovasz G. Multifocal simultaneous Salmonella typhi osteomyelitis in an immunocompetent adult. Scand J Infect Dis 2002;34:770-2.[PubMed]
240. Tran TH, Nguyen MD, Huynh DH, Nguyen TT, To SD, Le TP, Arnold K. A randomized comparative study of fleroxacin and ceftriaxone in enteric fever. Trans R Soc Trop Med Hyg 1994;88:464-5. [PubMed]
241. Trevett AJ, Nwokolo N, Lightfoot D, Naraqi S, Kevau IH, Temu PI, Igo JD. Ataxia in patients infected with Salmonella typhi phage type D2: clinical, biochemical and immunohistochemical studies. Trans R Soc Trop Med Hyg 1994;88:565-8. [PubMed]
242. Tribble D, Girgis N, Habib N, Butler T. Efficacy of azithromycin for typhoid fever. Clin Infect Dis 1995;21:1045-6. [PubMed]
243. Unal S, Hayran M, Tuncer S, Gur D, Uzun O, Akova M, Akalin HE. Treatment of enteric fever with pefloxacin for 7 days versus 5 days: a randomized clinical trial. Antimicrob Agents Chemother 1996;40:2898-900. [PubMed]
244. Uwaydah AK, al Soub H, Matar I. Randomized prospective study comparing two dosage regimens of ciprofloxacin for the treatment of typhoid fever. J Antimicrob Chemother 1992;30:707-11. [PubMed]
245. Uwaydah AK, Matar I, Chacko KC, Davidson JC. The emergence of antimicrobial resistant Salmonella typhi in Qatar: epidemiology and therapeutic implications. Trans R Soc Trop Med Hyg 1991;85:790-2. [PubMed]
246. Uysal H, Karademir A, Kilinc M, Erturk O. Salmonella encephalopathy with seizure and frontal intermittent rhythmic delta activity. Infection 2001;29:103-6.[PubMed]
247. van Basten JP, Stockenbrugger R. Typhoid perforation. A review of the literature since 1960. Trop Geogr Med 1994;46:336-9. [PubMed]
248. van de Wetering J, Visser LG, van Buchem MA, van der Hoeven JG. A case of typhoid fever complicated by unexpected diffuse cerebral edema. Clin Infect Dis 1995;21:1057-8. [PubMed]
249. Vazquez V, Calderon E, Rodriquez RS. Chloramphenicol-resistant strains of Salmonella typhosa. N Engl J Med 1972;286:1220. [PubMed]
250. Vinh H, Duong NM, Phuong le T, Truong NT, Bay PV, Wain J, Diep TS, Ho VA, White NJ, Day NP, Parry CM. Comparative trial of short-course ofloxacin for uncomplicated typhoid fever in Vietnamese children. Ann Trop Paediatr 2005;25:17-22. [PubMed]
251. Vinh H, Wain J, Vo TN, Cao NN, Mai TC, Bethell D, Nguyen TT, Tu SD, Nguyen MD, White NJ. Two or three days of ofloxacin treatment for uncomplicated multidrug-resistant typhoid fever in children. Antimicrob Agents Chemother 1996;40:958-61. [PubMed]
252. Wain J, House D, Zafar A, Baker S, Nair S, Kidgell C, Bhutta Z, Dougan G, Hasan R. Vi antigen expression in Salmonella enterica serovar Typhi clinical isolates from Pakistan. J Clin Microbiol 2005;43:1158-65. [PubMed]
253. Wain J, Pham VB, Ha V, Nguyen NM, To SD, Walsh AL, Parry CM, Hasserjian RP, HoHo VA, Tran TH, Farrar J, White NJ, Day NP. Quantitation of bacteria in bone marrow from patients with typhoid fever: relationship between counts and clinical features. J Clin Microbiol 2001;39:1571-6. [PubMed]
254. Wain J, Hien TT, Connerton P, Ali T, Parry CM, Chinh NT, Vinh H, Phuong CX, Ho VA, Diep TS, Farrar JJ, White NJ, Dougan G. Molecular typing of multiple-antibiotic-resistant Salmonella enterica serovar Typhi from Vietnam: application to acute and relapse cases of typhoid fever. J Clin Microbiol 1999;37:2466-72. [PubMed]
255. Wain J, Diep TS, Ho VA, Walsh AM, Nguyen TT, Parry CM, White NJ. Quantitation of bacteria in blood of typhoid fever patients and relationship between counts and clinical features, transmissibility, and antibiotic resistance. J Clin Microbiol 1998;36:1683-7. [PubMed]
256. Wain J, Hoa NT, Chinh NT, Vinh H, Everett MJ, Diep TS, Day NP, Solomon T, White NJ, Piddock LJ, Parry CM. Quinolone-resistant Salmonella typhi in Viet Nam: molecular basis of resistance and clinical response to treatment. Clin Infect Dis 1997;25:1404-10. [PubMed]
257. Wallace MR, Yousif AA, Habib NF, Tribble DR. Azithromycin and typhoid. Lancet 1994;343:1497-8. [PubMed]
258. Wallace MR, Yousif AA, Mahroos GA, Mapes T, Threlfall EJ, Rowe B, Hyams KC. Ciprofloxacin versus ceftriaxone in the treatment of multiresistant typhoid fever. Eur J Clin Microbiol Infect Dis 1993;12:907-10. [PubMed]
259. Wang F, Gu XJ, Zhang MF, Tai TY. Treatment of typhoid fever with ofloxacin. J Antimicrob Chemother 1989;23:785-8. [PubMed]
260. Wani T, Kakru DK, Shaheen R, Nazir A, Lone R, Shakeel S, Shah A. Infective endocarditis due to Salmonella typhi--a case report. Indian J Pathol Microbiol 2004;47:76-7. [PubMed]
261. Warshauer D, Monson T, Kurzynski T. The Wisconsin State Laboratory of Hygiene and emerging enteric pathogens. WMJ 2003;102:40-4. [PubMed]
262. White NJ, Dung NM, Vinh H, Bethell D, Hien TT. Fluoroquinolone antibiotics in children with multidrug resistant typhoid. Lancet 1996;348:547. [PubMed]
263. Woodward TE, Smadel JE. Management of typhoid fever and its complications. Ann Intern Med 1964;60:144-57. [PubMed]
264. Zafar J, Abbas S, Qayyum A, Ahmed N, Hussain S, Qazi RA. Typhoid orchitis. J Pak Med Assoc 1995;45:106-7. [PubMed]
Tables
Table 1. Extra-intestinal Infectious Complications of Typhoid Fever Caused by Salmonella enterica serotype Typhi
| Organ system involved | Prevalence | Risk factors | Complications |
|---|---|---|---|
| Central Nervous System | 3-35% | Residence in endemic region,217malignancy,218 endocarditis, congenital heart disease, paranasal sinus infections, pulmonary infections, meningitis, trauma, surgery, and osteomyelitis of the skull | Encephalopathy,219 cerebral edema,217 subdural empyema,220 cerebral abscess,218, 221 meningitis,222ventriculitis, transient Parkinsonism, motor neuron disorders, ataxia,20 seizures, Guillain-Barré syndrome, psychosis223 |
| Cardiovascular | 1-5% | Cardiac abnormalities such as existing valvular abnormalities, rheumatic heart disease or congenital heart defects224 | Endocarditis,225, 226,227,228myocarditis,223pericarditis,229 arteritis, congestive heart failure230 |
| Pulmonary | 1% | Residence in endemic region, past pulmonary infection, sickle cell anemia, alcohol abuse, diabetes, HIV infection30 | Pneumonia,30, 231 empyema,232 bronchopleural fistula, infected pulmonary hydatid cyst233 |
| Bone and Joint | < 1% | Sickle cell anemia, diabetes, systemic lupus erythematosus, lymphoma, liver disease, previous surgery or trauma, those at extremes of age, and steroid use234 | Osteomyelitis,62, 223, 234,235,236,237,238,239 septic arthritis240 |
| Hepatobiliary | 1-26% | Residence in endemic region, pyogenic infections, intravenous drug use, splenic trauma, HIV, hemoglobinopathy | Cholecystitis, hepatitis,223, 241 hepatic abscesses242, splenic abscess,243, 244,245 peritonitis, paralytic ileus223 |
| Genitourinary | <1% | Urinary tract, pelvic pathology and systemic abnormalities | Urinary tract infection,55, 246 renal abscess, pelvic infections,247 testicular abscess, prostatitis, epididymitis |
| Soft tissue infections | 17 cases reported in the English literature | Diabetes248 | Psoas abscess 248, 249 gluteal abscess,250 cutaneous vasculitis,251 |
| Hematologic | 5 cases reported in the English literature | Hemophagocytosis syndrome252, 253 |
Abbreviations: HIV – human immunodeficiency virus
Table 2. Minimum Inhibitory Concentrations (μg /ml) for Selected Antibiotics Against Salmonella typhi
| "Sensitive isolates" | "MDR isolates" | |||
|---|---|---|---|---|
| MIC50 | MIC90 | MIC50 | MIC90 | |
| Penicillin G | 4 | 8 | ||
| Ampicillin | 0.5 | 1.0 | >256 | >256 |
| Amoxicillin-Clavulanic acid | 0.5 | 1.0 | 8 | 8 |
| Piperacillin | 0.5 | 1 | ||
| Piperacillin-Tazobactam | 0.5 | 1 | ||
| Ticarcillin | 2 | 4 | ||
| Azlocillin | 8 | 8 | ||
| Mezlocillin | 2 | 2 | ||
| Mecillinam | 0.125 | 0.125 | 1* | 2* |
| Cefuroxime | 2 | 4 | ||
| Cefoperazone | 1 | 4 | ||
| Cefoxitin | 1 | 4 | ||
| Ceftriaxone | 0.06 | 0.125 | 0.06 | 0.125 |
| Ceftazidime | 0.25 | 0.25 | ||
| Cefepime | 0.06 | 0.125 | ||
| Cefpirome | 0.06 | 0.06 | ||
| Cefixime | 0.06 | 0.06 | ||
| Ceftizoxime | 0.06 | 0.125 | ||
| Aztreonam | 0.125 | 0.25 | ||
| Imipenem | 0.25 | 0.5 | ||
| Meropenem | 0.06 | 0.06 | ||
| Azithromycin | 8 | 8 | 8 | 8 |
| Rifampicin | 8 | 16 | ||
| Trimethoprim | 0.125 | 0.25 | 128 | >256 |
| Sulfamethoxazole | 4 | 16 | >256 | >256 |
| Chloramphenicol | 4 | 8 | >256 | >256 |
| Tetracycline | 1 | 1 | >256 | >256 |
| Gentamicin | 0.25 | 2.0 | ||
| Nalidixic acid | 4 | 8 | 4 | 8 |
| Norfloxacin | 0.06 | 0.25 | 0.06 | 0.25 |
| Ciprofloxacin | 0.015 | 0.03 | 0.015 | 0.03 |
| Ofloxacin | 0.06 | 0.125 | 0.06 | 0.125 |
| Pefloxacin | 0.125 | 0.125 | 0.125 | 0.125 |
Table 3. Fluoroquinolone Efficacy in Enteric Fever
| Drug | Reference | Dosage | Patients | Clinical cure % | Micro cure % | FCT (days) | Relapse Rate % |
|---|---|---|---|---|---|---|---|
| Ofloxacin | Morelli et al 1992120 | 300 mg tid 15 days | 30 | 100 | 100 | 2.6 | 0 |
| Pefloxacin | Morelli et al 1992120 | 400 mg tid 15 days | 36 | 100 | 100 | 3.7 | 0 |
| Ciprofloxacin | Morelli et al 1992120 | 500 mg tid 15 days | 20 | 100 | 100 | 3.3 | 0 |
| Enoxacin | Morelli et al 1992120 | 300 mg tid 15 days | 20 | 80 | 80 | 4.6 | 0 |
| Norfloxacin | Morelli et al 1992120 | 400 mg tid | 20 | 60 | 60 | 4.6 | 0 |
| Norfloxacin | Sarma & Durairaj 1991121 | 400mg bid 7 days | 20 | 100 | 100 | 3.7 | 0 |
| Ciprofloxacin | Uwayda et al 1992254 | 500mg bid, 7-10 days | 34 | 100 | 100 | 4.9 | 0 |
| Ciprofloxacin | Uwayda et al 1992254 | 750mg bid, 7-10 days | 28 | 100 | 100 | 5.2 | 4 |
| Fleroxacin | Arnold et al 1993145 | 400mg od, 7 days | 28 | 83 | 96 | 4 | 17 |
| Fleroxacin | Arnold et al 1993145 | 400mg od, 14 days | 35 | 100 | 97 | 4 | 0 |
| Ciprofloxacin | Wallace et al 1993161 | 500mg bid, 7 days | 20 | 100 | 100 | 4 | 0 |
| Fleroxacin | Hien et al 1994159 | 400mg od, 7 days | 15 | 100 | 100 | 3.4 | 0 |
| Ofloxacin | Smith et al 1994160 | 200mg bid, 5 days | 22 | 100 | 100 | 3.4 | 0 |
| Ciprofloxacin | Alam et al 199576 | 500mg bid, 10 days | 35 | 100 | 100 | 4.2 | 0 |
| Ciprofloxacin | Alam et al 199576 | 500mg bid, 14 days | 34 | 100 | 100 | 4.9 | 0 |
| Ofloxacin | Smith et al 1995160 | 15mg/kg/d 3 days | 118 | 100 | 100 | 2.5 | 0 |
| Ofloxacin | Smith et al 1995160 | 10mg/kg/d 5 days | 110 | 100 | 100 | 3.0 | 1 |
| Fleroxacin | Duong et al 1995255 | 400mg od, 5 days | 41 | 97.5 | 100 | 3.4 | 4 |
| Fleroxacin | Duong et al 1995255 | 400mg od, 3 days | 22 | 100 | 100 | 3.7 | 0 |
| Ofloxacin | Vinh et al 1996162 | 15mg/kg/d 3 days | 47 | 96 | 100 | 4.5 | 0 |
| Ofloxacin | Vinh et al 1996162 | 15mg/kg/d 2 days | 53 | 89 | 98 | 4.5 | 2 |
| Pefloxacin | Unal et al 1996256 | 400mg bid 7 days | 24 | 100 | 100 | 3.4 | 4 |
| Pefloxacin | Unal et al 1996256 | 400mg bid 5 days | 22 | 100 | 96 | 3.1 | 0 |
| Ofloxacin | Chinh et al 1997135 | 15mg/kg/d 3 days | 53 | 89 | 100 | 4.0 | 2 |
| Ofloxacin | Chinh et al 1997135 | 15mg/kg/d 2 days | 47 | 98 | 98 | 4.0 | 0 |
| Ofloxacin | Secmeer et al 1997257 | 40mg/kg/d | 24 | 100 | 100 | 3.3 | 0 |
| Ciprofloxacin | Girgis et al 1999258 | 500mg bid 7 days | 28 | 100 | 100 | 3.3 | 0 |
| Ofloxacin | Cao et al 1999259 | 10mg/kg/d 5 days | 38 | 97 | 100 | 4.4 | 0 |
| Ofloxacin* | Chinh et al 200079 | 8mg/kg/d 5 days | 44 | 86 | 95.5 | 5.6 | 5 |
| Ciprofloxacin | Gasem et al 200370 | 500mg/d 7d | 28 | 96 | 82 | 5.1 | 0 |
| Ofloxacin | Vinh et al 2005170 | 10mg/kg/d 3 days | 107 | 95.3 | 99.1 | 4.21 | 2.8 |
| Ofloxacin | Vinh et al 2005170 | 10mg/kg/d 2 days | 89 | 91.3 | 95.5 | 3.83 | 2.2 |
* 48% of the infections were quinolone resistant
Table 4. Third Generation Cephalosporin Efficacy In Enteric Fever Drug
| Reference | Dosage | No of patients | Clinical Cure (%) | Micro Cure (%) | mean (SD) FCT(days) or range | Relapse Rate(%) | |
|---|---|---|---|---|---|---|---|
| Cefotaxime | Soe et al 1987115 | 200mg/kg /day 6-14 d | 61 | 82 | 6 | ||
| Ceftriaxone | Islam et al 1988149 | 3-4g/day, 7 d | 32 | 91 | 100 | 4->14 | 6 |
| Ceftriaxone | Lasserre et al 1991260 | 3g/day,3 d | 19 | 95 | 100 | 3-13 | 11 |
| Ceftriaxone | Lasserre et al 1991260 | 4g/day, 3 d | 20 | 100 | 100 | 4-11 | 0 |
| Ceftriaxone | Wallace et al 1993161 | 3g/day, 7 d | 22 | 73 | 100 | 5.2 | 5 |
| Ceftriaxone | Islam et al 1993149 | 4g/day, 5 d | 28 | 79 | 100 | 4 | |
| Ceftriaxone | Tran et al 1994159 | 2g/day, 5 d | 15 | 87 | 93 | 6.7 | 0 |
| Ceftriaxone | Smith et al 1994160 | 3g/day, 3 d | 25 | 72 | 92 | 8.2 | 4 |
| Ceftriaxone | Bhutta et al 199477 | 65mg/kg /day, 14 d | 25 | 88 | 88 | 8.0 | 14 |
| Cefixime | Bhutta et al 199477 | 20mg/kg /day, 12+ d | 50 | 100 | 100 | 5.3 | 4 |
| Cefixime | Girgis et al 1994158 | 10mg/kg /day, 14 d | 25 | 88 | 96 | 8.3 | 4 |
| Cefixime | Girgis et al 1995178 | 7.5mg/kg bid, 14d | 50 | 100 | 100 | 5.3 | 6 |
| Ceftriaxone | Girgis et al 1995178 | 50-70mg/kg daily, 5 d | 43 | 100 | 100 | 3.9 | 5 |
| Cefixime | Rabbani et al 1998261 | 10mg/kg/d 14d | 20 | 90 | 90 | 6 | |
| Cefixime | Cao et al 1999259 | 20mg/kg/d 7d | 44 | 75 | 90 | 8.5 | 2 |
| Ceftriaxone | French et al 2000262 | 75mg/kg/d 7d | 30 | 97 | 97 | 3.9 | 13 |
| Ceftriaxone | Bhutta et al 2000171 | 6mg/kg/d 7d | 29 | 93 | 100 | 5.4 | 4 |
| Ceftriaxone | Bhutta et al 2000171 | 65mg/kg/d 14d | 28 | 96 | 100 | 5.2 | 0 |
| Ceftriaxone | Frenck et al 2004263 | 75mg/d 5d | 36 | 81 | 97 | 3.6 | 14 |
FCT = Fever clearance time
Table 5. Azithromycin Efficacy In Enteric Fever
| Reference | Dosage | Patients | Clinical cure % | Micro cure % | FCT (days) | Relapse Rate % |
|---|---|---|---|---|---|---|
| Butler et al 1999264 | 9.6 mg/kg/d 7 days | 42 | 88 | 100 | 4.1 | 0 |
| Girgis et al 1999258 | 16 mg/kg followed by 8 mg/kg total 7 days | 36 | 100 | 100 | 3.8 | 0 |
| Chinh et al 200079 | 20 mg/kg/d 5 days | 44 | 96 | 98 | 5.5 | 0 |
| Frenck et al 2000262 | 10 mg/kg/d 7 days | 34 | 91 | 97 | 4.1 | 0 |
| Frenck et al 2004263 | 20 mg/kg/d 5 days | 32 | 100 | 100 | 4.5 | 0 |
Table 6. Antibiotics of Choice [Download PDF]
| Endemic area | Non-immune | |
|---|---|---|
| Uncomplicated enteric fever | Ofloxacin or ciprofloxacin orally 7.5mg/kg b.i.d or levofloxacin orally 500mg daily for 3-5 days* | Ofloxacin or ciprofloxacin orally 7.5mg/kg b.i.d or levofloxacin orally 500mg daily for 5-7 days* |
| Severe typhoid** | Ofloxacin or ciprofloxacin 7.5mg/kg infused over 30-60 minutes every 12 hours or levofloxacin 500mg infused every 24 hours until oral treatment can be substituted. Continue same dose for 10-14 days. | Ofloxacin or ciprofloxacin 7.5mg/kg infused over 30-60 minutes every 12 hours or levofloxacin 500mg infused every 24 hours until oral treatment can be substituted. Continue same dose for 10-14 days. Immunocompromised patients should receive at least three weeks treatment. |
| Carriers | Adults: Ofloxacin or Ciprofloxacin orally 7.5 mg/kg b.i.d. or levofloxacin orally 500mg daily for 4 weeks. Children: Amoxicillin 10mg/kg/day for 6-8 weeks plus probenecid |
*Pefloxacin or fleroxacin have both proved very effective as well (Table 2). The three days course is particularly useful in epidemic containment.
**Dexamethasone 3mg/kg I.V. stat followed by 1mg/kg six hourly for 48 hours should be given to patients with encephalopathy or shock unrelated to perforation or hemorrhage. For quinolone resistant infections substitute ceftriaxone.
Alternative Treatments
| Uncomplicated enteric fever | Severe typhoid | |
|---|---|---|
| Chloramphenicol | 75mg/kg/day in 4 divided oral doses for 14 days | Chloramphenicol succinate 75mg/kg/day I.V. or I.M. in 4 divided doses until oral treatment can be substituted. Then 50mg/kg/day orally for 14-21 days |
| Ampicillin/amoxicillin | Amoxicillin 75-100mg/kg/day in 3-4 divided oral doses for 14 days | Ampicillin 15mg/kg/day I.V. in 4 divided doses for 14-21 days |
| Trimethoprim/ sulfamethoxazole | 8/40 mg/kg/day in 2 divided oral doses (corresponding in adults to 2-3 tablets b.i.d.) 14 days. | Intravenous dose regimen similar to the oral regimen |
| Cefixime/ceftriaxone | Cefixime 20mg/kg/day in 4 divided oral doses for 7-10 days | Ceftriaxone 60 mg/kg/day I.V. or I.M. for at least 5 days, then if possible switch to oral therapy to complete 14-21 days treatment |
Table 7. Typhoid Vaccines [Download PDF]
| Vaccine | Dose | Adverse effects | Comments |
|---|---|---|---|
| Vi capsular polysaccharide vaccine | Single dose 0.5mL of 50 µg/mL vaccine by I.M. or deep S.C. injection | Local pain, erythema and fever may occur 1-3 days after administration. | Children < 18 months may show sub-optimal response. Repeat every 3 years |
| Ty 21a oral live attenuated vaccine | 1 capsule to be swallowed with cold or lukewarm drink on days 1, 3, and 5 | Usually none. Nausea, vomiting, abdominal cramps, headache, fever, allergic reactions. Rarely: anaphylaxis. | Contraindicated in patients who are immunosuppressed either by disease or drugs Inactivated by antibiotics Capsules must be refrigerated. Not recommended for children <6 years. Provides protection 7-10 days after last dose, and in endemic areas this lasts for 3 years in most cases, but for travelers who are not repeatedly exposed, protection may last for only one year. Do not give mefloquine until 3 days after last dose, and administration of oral polio vaccine should be separated by at least three weeks |
Figure 1: 1,000 Cases per 100,000 Population per Year.
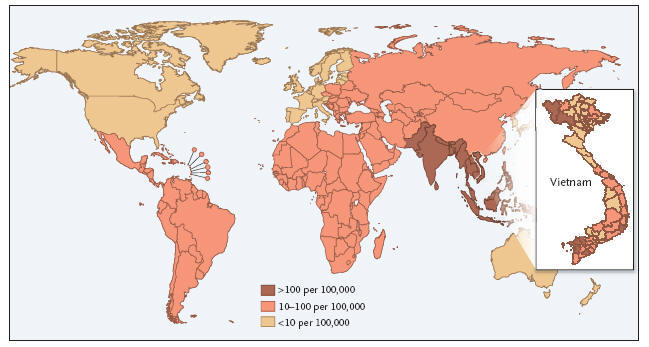
What's New
Lynch MF, et al. Typhoid fever in the United States, 1999-2006. JAMA 2009;302(8):859-65.
Sur D, et al. A Cluster-Randomization Effectiveness Trial of Vi Typhoid Vaccine in India. New Engl J Med 2009;361(4):335-344.
Guided Medline Seach For:
Reviews
Baron EJ. Flow chart for identification of enteric fecal pathogens
Effa EE, et al. Fluoroquinolones for treating typhoid and paratyphoid fever (enteric fever). Cochrane Database Syst Rev 2011;10: CD004530.
Connor BA, Schwartz E. Typhoid and paratyphoid fever in travellers. Lancet Infectious Diseases 2005;5:623-628.
Huang DB, DuPont HL. Problem pathogens: extra-intestinal complications of Salmonella enterica serotype Typhi infection. Lancet Infect Dis 2005;5:341-8.
Guided Medline Search For Recent Reviews
History
Lin-Hui Su and Cheng-Hsun Chiu: Nomenclature of Salmonella.
Logan McCool: The Story of Typhoid Mary.
Levine MM. Typhoid Vaccines Ready for Implementation: A History. New Engl J Med 2009;361(4):403-405.
Guided Medline Search For Historical Aspects
Table of Contents
- Microbiology
- Epidemiology
- Clinical Manifestations
- Laboratory Diagnosis
- Susceptibility in vitro and in vivo
- Antimicrobial Therapy
- Adjunctive Therapy
- Endpoints for Monitoring Therapy
- Vaccines
- Comments and Controversies