Figure 1: Fever curves during febrile and afebrile conditions
The broken line represents the normal diurnal temperature variation in an afebrile person, peaking in the late afternoon and reaching a nadir in the early morning. The solid line is the temperature curve during a febrile illness. The diurnal variation is maintained but at a higher set point during infection. The temperature rises because of an increase in the hypothalamic set point (rising vertical dotted arrow) to a new higher set point (40º C). Heat is generated by shivering causing chills (C). Heat is lost by sweating (S) when the set point is lowered (falling vertical arrow) toward the “normal” set point. The solid arrow represents administration of an antipyretic. This artificially lowers the set point to a greater extent than would be expected during the normal diurnal variation of an infection causing a marked fall in temperature. The patient experiences a “drenching” night sweat.
Used with permission by Marcel Dekker Inc in Medical Management of Infectious Diseases, Ed C Grace, 2003.
Figure 2: Sagittal view of a mammalian brain.
This shows the position of the anterior hypothalamus, organum vasculosum lamina terminalis (OVLT), reticular formation (RF) and spinothalamic tract (STt) and the preoptic and septal nuclei of the hypothalamus.
Used with permission from Mackowiak PA, Concepts of Fever. Arch Intern Med 1998;158:1870-1881.
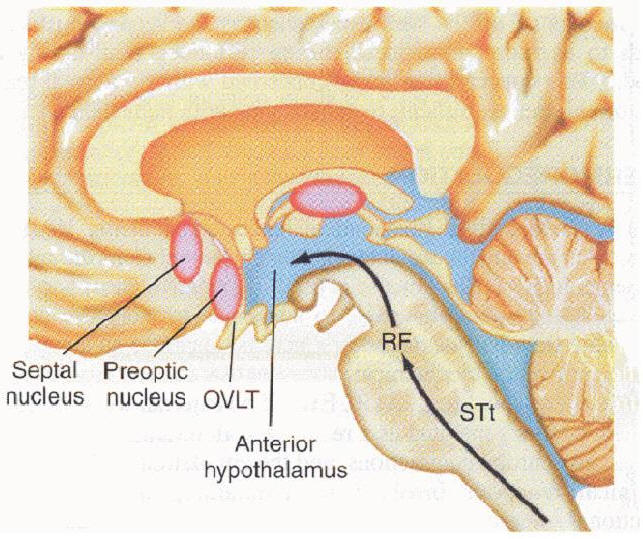
Figure 3: Fever, immunity and the inflammatory response
Exogenous pyrogen stimulates cytokine (endogenous pyrogen) release. IL-1, IL-6, TNF and INF reset the hypothalamic set point via the organum vasculosum of the lamina terminalis (OVLT). The body temperature is raised. Endogenous pyrogen also triggers immunologic, inflammatory and metabolic responses that in turn help control the exogenous pyrogen (dashed lines). Elevation in body temperature also improves the immunologic and inflammatory responses (dotted lines).
WBC = white blood cell, IL-1=interleukin-1, IL-6 = interleukin-6, TNF = tumor necrosis factor, INF = interferon, NK = Natural Killer, Zn = zinc, Fe = iron, Cu = copper
Used with permission by Marcel Dekker Inc in Medical Management of Infectious Diseases, Ed C Grace, 2003.
Figure 4: Prostaglandin E2 production
Prostaglandin E2 is synthesized from membrane bound phospholipid by phospholipase A2 and cyclooxygenase (COX). Corticosteroids inhibit phospholipase A2 while aspirin and non-steroidal anti-inflammatory drugs inhibit COX. Metabolites of acetaminophen can inhibit COX isoenzymes.
IL-1 = interleukin –1, TNF = tumor necrosis factor, IL-6 = interleukin-6, IFN = interferons, ASA = acetylsalicylic acid, NSAIDS = non-steroid anti-inflammatory drugs
Used with permission by Marcel Dekker Inc in Medical Management of Infectious Diseases, Ed C Grace, 2003.
Table 1: Direct and indirect effects of Interleukin - 1
|
Metabolic |
Physiologic |
Immunologic |
|
|
|
Table 2: Benefits of fever
|
Teleological:
|
|
In vitro temperature elevation:
|
|
In vivo studies in cold blooded fish and lizards:
|
Table 3: Hyperthermia
|
Heat stroke
|
|
Malignant hyperthermia
|
|
Neuroleptic malignant syndrome
|