
Fever in Organ Transplant Recipients
Authors: Patricia Muñoz MD, Ph.D., Nina Singh, M.D., Emilio Bouza MD, Ph.D.
INTRODUCTION
Fever is a nonspecific but sensitive indicator of disease both for the patient and the physician. Solid organ transplant (SOT) recipients are usually well aware of the potential importance of fever that may foretell the existence of an infectious or non-infectious complication (rejection, cancer, etc). Antimetabolite immunosuppressive drugs, such as mycophenolate mofetil and azathioprine are associated with significantly lower maximum temperatures and leukocyte counts (158). However, in general, the immunosuppression caused by transplantation does not abolish the inflammatory response, so most transplant recipients with a significant infection will have fever and most fevers will have an infectious etiology in this setting. For example 87% of the febrile episodes occurring in the transplant patients hospitalized in the ICU were due to infections (173).
Very few studies have specifically addressed the problem of post-transplant fever (22, 29, 119, 175) from a general perspective. In transplant recipients, fever has been defined as an oral temperature of 37.8ºC or greater on at least two occasions during a 24-hour period (184). Regarding prolonged fevers, none of the definitions of fever of unknown origin (classic, nosocomial, immune-deficiency and HIV-related) are completely accurate for the SOT population and these criteria are an open field for future research (22).
The importance of careful history and physical examination cannot be overemphasized. As in other immunocompromised hosts, the temporal sequence of the events is critical. The most probable site and etiology of the fever will be greatly influenced by the time after transplantation when it occurs, antecedent surgical complications or rejection episodes, intensity of iatrogenic immunosuppression, risk of primary acquisition of infections, prophylactic regimens, exposures, etc. Infections detected in the first month after transplantation are usually hospital-acquired bacterial complications related to surgical or technical problems. Bloodstream infections, catheter-related infections, nosocomial pneumonia, and surgical site infections predominate (103, 154). Reactivation of latent infections and early fungal and viral infections account for a smaller proportion of febrile episodes during this period. Opportunistic infections will appear later unless an expected exposure has occurred.
Febrile and hypothermic episodes in a transplant recipient should be promptly evaluated by careful physical examination, blood and urine cultures and a chest radiograph. Timing of infection and clinical and laboratory data suggestive of a particular site should guide the pursuit of other diagnostic tests. Empiric antibiotic therapy is often necessary and should be selected considering the most probable site of infection, possibility of antimicrobial resistance in particular institution, and prior receipt of antimicrobials. Evaluation of febrile patients with specific organ involvement will be discussed in detail below. The use of antipyretic agents is not recommended in most cases. If administered, they should be given at regular intervals to minimize recurrent rigors.
In this chapter we have followed a syndromic instead of an etiologically-oriented approach since we believe that it may reflect more accurately the initial clinical evaluation of the patient. Our aim is to provide a practical approach to differential diagnosis, diagnostic procedures and empirical therapy of most frequently encountered clinical scenarios associated with post-transplant fever.

FEVER AND NEUROLOGIC COMPLICATIONS
The frequency of neurologic complications in SOT patients ranges from 13%-48% (25, 69, 141, 206). Central nervous system (CNS) opportunistic infections are very rare nowadays (1.5% in our series of heart transplantation, accounting for 7.6% of the neurologic complications), while peripheral herpes zoster accounts for a significant morbidity in this population. However, due to their severity and clinical sequelae, CNS infections should always be suspected in a febrile patient with headache, altered mental status, seizures, focal neurologic deficit, or a combination of these neurologic manifestations. Seizures, hypoxia, hypoperfusion and malignancies must also be considered (145). It is important to remember that altered mental status in the transplant setting can also result from vascular, toxic or metabolic etiologies, including side-effects of immunosuppressive agents (176), but CNS infections always warrant exclusion in this setting (177).
As a result of immunosuppression, solid organ transplant recipients are at risk of neurologic opportunistic infections that include cytomegalovirus (CMV), herpes simplex virus (HSV), varicella zoster virus (VZV), L. monocytogenes, Nocardia spp., mycobacteria, C. neoformans, Aspergillus, zygomycetes, and toxoplasmosis.
The initial step in the evaluation of a febrile patient with neurologic symptoms or signs is usually a neuroimaging study to determine the presence and characteristics of the CNS lesion. Up to 10-20% of SOT patients will require an MRI due to severe neurologic disorders and depending on the neuroimaging findings, CNS infections can be characterized as those presenting with focal or mass lesions (brain abscesses), non focal lesions, and those without a discernable neuroimaging abnormality or meningitis (meningoencephalitis). Time after transplantation, result of the neuroimaging test and speed of evolution may guide the etiologic diagnosis (Table 2).
Focal or Mass Lesions
Focal neurological symptoms are usually caused by focal parenchymal brain disease, usually corresponding to brain abscesses or tumors. However, metastases or hematogenous infections affecting the gray/white matter junction may cause similar clinical manifestations.
Brain abscesses are relatively uncommon (0.6%) in SOT patients and most of them (78%) are caused by fungi (mostly Aspergillus and less commonly Mucorales, phaeohyphomycetes or dematiaceous fungi), followed byToxoplasma gondii and (162). Focal brain manifestations (seizures or focal neurologic abnormalities) may also be caused by T. gondii, Nocardia spp., or post-transplantation lymphoproliferative disease. Fever is not common and was documented in only 45% of the liver transplant recipients with brain abscesses. As discussed herein, the characteristics that may help in the differential diagnosis are the time of appearance of the lesion and the presence of concomitant extra-neural disease (predominantly pulmonary) which is very common in patients with fungal brain abscesses (70%). Such lesions usually provide an early clue to the diagnosis. If extraneural involvement is not documented a brain biopsy should be performed to establish the etiological diagnosis. Empiric therapy of brain abscesses in SOT recipients should include antifungal, and not antibacterial or antiviral therapy.
Aspergillus is the most common cause of CNS space occupying lesions in our experience (4% of the patients with a neurologic complication and 0.8% of the heart transplant patients) and cerebral aspergillosis usually occurs in the early post-transplantation period. Although invasive aspergillosis it may present as primary CNS disease, most cases occur in the setting of disseminated disease in patients with known risk factors (CMV disease, renal failure, high doses of corticosteroids, etc) (90, 194). Overall, disseminated Aspergillus disease has been described in 9-36% of kidney recipients, 15-20% of lung recipients, 20-35% of heart recipients and 50-60% of liver recipients with invasive aspergillosis (IA) (16, 57, 139). Disseminated infection with CNS involvement occurred in 17% of the cases in Spain (49). Liver transplant recipients appear to be uniquely susceptible to dissemination of Aspergillus beyond the lungs and to CNS involvement (16, 177).
Most common clinical manifestations of CNS aspergillosis include alteration of mental status, which may be rapidly progressive, diffuse CNS depression and seizures (up to 41%). Focal neurologic deficit or symptoms and headache are less common and meningism is rare (139, 194). Leptomeningeal involvement or subarachnoid hemorrhage secondary to rupture of the mycotic aneurysm may account for this (16, 49, 57, 139,). The CSF fluid is almost always sterile. Concomitant lung lesions usually permit an earlier diagnosis. Prognosis is grave and the mainstay of therapy is voriconazole.
Scedosporium, zygomycetes and other uncommon fungi are being increasingly detected as significant CNS pathogens in transplant recipients (65, 131). Brain abscesses due to dematiaceous fungi are described a median of 3 months posttransplantation, but may occur as late as 2 years later (168). These fungi are noteworthy for their neurotropic potential and their predilection to cause brain abscesses. CNS lesions caused by these microorganisms may be single or multiple and appear as ring enhancing images. Concomitant cutaneous or pulmonary involvement is present in 20% of the cases and permits an easier diagnosis. Infections due to the agents of zygomycosis seem to be increasing in the transplant population and nearly 50% are of the rhinocerebral form (11, 67, 165).
Intracranial abscesses due to bacterial pathogens are notably rare in transplant recipients with the exception of nocardiosis. The incidence of nocardiosis has significantly decreased since the introduction of routine use of trimethoprim-sulfamethoxazole, however one third of the reported patients with nocardiosis were receiving prophylaxis. Nocardiosis is usually observed between 1-6 months posttransplantation (mean 120 days). The clinical presentation ofnocardiosis includes pneumonia, CNS focal lesions and cutaneous involvement (7, 63, 135, 161, 177). Brain abscesses due to Nocardia are multiple in up to 40% of the cases and may show ring enhancement. Diagnosis may be established by direct observation of biological samples using modified Ziehl-Neelsen staining or Gram stain. Respiratory, cutaneous or soft tissue samples can be an important tool for establishing the microbiologic diagnosis of the CNS lesion. It is uncertain whether new species of Nocardia are emerging as pathogens or if changes in taxonomy and improvements in identification have led to the reclassification Nocardia isolates that cause disease. The mainstays of treatment aresulphonamides or cotrimoxazole, although some authorities recommend induction therapy with a combination of drugs including carbapenem derivatives.
Toxoplasmosis is an uncommon disease in SOT that receives prophylaxis with cotrimoxazole (13, 111). The incidence is higher in heart transplant recipients since cardiac tissue represents the site of latency of T. gondii cysts. The disease usually occurred within 3 months post-transplantation; however, late-onset disease has been reported. Fever (74%), changes in mental status (45%) and seizures (35%) are the main clinical features. Headache, pneumonia and chorioretinitis may also be found (27, 66, 133, 150, 151, 205). Diagnosis can be established by serology and by direct examination, culture, or polymerase chain reaction of biological samples. In heart transplant recipients the diagnosis may be provided by the endomyocardial biopsy (199). The CNS lesions of T. gondii are usually multiple, have preferential periventricular localization and may or may not demonstrate ring enhancement. Rarely, the lesions of toxoplasmosis may be hemorrhagic. The mortality rate was high (around 60%). Therapy may be complicated by obstructive urinary tract lithiasis due to sulfadiazine crystals (51). Disseminated toxoplasmosis should be considered in the differential diagnosis of immunocompromised patients with culture-negative sepsis syndrome, particularly in the presence of combination of neurologic and respiratory manifestations (8). Other parasitic infections such as Chagas disease, neurocysticercosis,schistosomiasis, and strongyloidiasis are exceedingly rare and the epidemiological history is usually a diagnostic clue (200). Brain abscesses due to M. tuberculosis have also been described but are rare and generally unlikely to occur in the early posttransplant period (31, 104).
Non-Focal Lesions
Organ transplant patients may have non-focal lesions, meningoencephalitis or meningitis, without lesions in the CT study. If the lesions affect the white matter the most probable diagnosis are immunosuppressive associated leukoencephalopathy or posterior multifocal leukoencephalopathy. If the lesions affect the gray and white matter the differential diagnosis should include viral encephalitis and early bacterial or fungal cerebritis. Meningitis may be infectious or non-infectious (eg, OKT3-induced meningitis). Meningoencephalitis in SOT recipients is predominantly due to viruses, e.g., herpesviruses, and less frequently, due to Listeria monocytogenes, Toxoplasma gondii, and Cryptococcus.
HHV-6 has been proposed to be most neuroinvasive of the herpesviruses although very few cases of encephalitis have reported to date (15, 84, 89, 102, 128, 149, 178). Encephalitis due to HHV-6 occurs in the early post-transplant period; the median time to onset in transplant recipients is ~45 days. Mental status changes, ranging from confusion to coma (92%), seizures (25%) headaches (25%), and speech disturbance (25%) were the predominant clinical manifestations of HHV-6 encephalitis (178). Fever was present in only 25% of the patients, but characteristically febrile patients may have very high temperatures (up to 40oC). HHV-6 viremia was documented in 78% of the patients with HHV-6 encephalitis. Cerebrospinal fluid pleocytosis is generally lacking, with 50% of the patients having ≤ 5 cells/mm3. Fifty-eight percent (7/12) of the patients had elevated CSF protein, and none had hypoglycorrhachia. Neuroimaging abnormalities on CT or MRI likewise are usually absent. When detectable, the lesions are nonenhancing, involve both gray and white matter, and have no preferential cortical localization (178). Diagnosis is based on a positive HHV-6 PCR in a patient with CNS symptoms.
Encephalitis due to herpes simplex virus or CMV is rare in SOT patients. As with other herpes viruses, the detection of viral genome by polymerase chain reaction in the cerebrospinal fluid allows a rapid diagnosis.
Bacterial meningitis was the most common CNS infection in our cohort of heart transplant recipients, accounting for 5.12% of all neurologic complications patients and 1.04% of all the heart patients. Listeria monocytogenes can cause isolated bacteremia, meningitis, meningoencephalitis, myocarditis or even myocardial abscesses at any time after transplantation, although most infections occur in the late post-transplant period (55, 88, 177). Listeria may cause a unique syndrome of brainstem encephalitis or rhomboencephalitis characterized by cranial nerve palsies or pontomedullary signs. Portal of entry is usually gastrointestinal and some patients may have diarrhea or abdominal pain. We suggest a cranial CT scan in all transplant patients with a Listeria recovered from a clinical sample even if no overt neurological manifestations are present. Therapy consists of a three week antibiotic course with ampicillin and gentamicin or cotrimoxazole.
Cryptocococcosis affects an average of 2.6%-5% of the transplant recipients and CNS is involved in 25-72% of the patients (2, 62, 96, 171). Lung involvement is proven in 54% of the SOT with cryptocococcosis (182). Cryptococcal infections generally occur late after transplantation (>3 months), however, rare cases of early fulminant infections have been reported. Cryptococcal meningitis is by far the most frequently encountered clinical presentation of cryptocococcosis presenting with headache, visual symptoms, and altered mental status. Cryptococcomas are rare (183). CSF analysis in cryptococcal meningitis in transplant recipients has revealed moderate pleocytosis (0 - 485 white blood cells/mm3). Hypoglycorrhachia has been reported in 40% of patients. Diagnosis is based on a positive CSF culture for Cryptococcus or positive CSF cryptococcal antigen (182). No correlation was found between CSF or serum cryptococcal antigen titer and evolution or CSF sterilization at 2 weeks.
A CT scan is recommended in all cases given that CNS lesions may be detectable in ~30% of the SOT recipients with CNS cryptocococcosis. Reported findings include patchy or diffuse leptomeningeal enhancement, hydrocephalus, parenchymal mass lesions or cryptococcomas, gelatinous pseudocysts, and dilation of the perivascular (Virchow-Robin) spaces. In our multicentric study, leptomeningeal lesions, mass lesions, and hydrocephalus were observed in 14%, 12%, and 4% of the patients with cryptococcal disease, respectively. Whereas a majority of the lesions were documented at baseline, 19% of the CNS lesions developed after initiation of antifungal therapy (182). These cases may represent an immune reconstitution syndrome resulting from an enhanced inflammatory response due to reversal of cryptococcal induced immunosuppression, initiation of antifungal therapy, and reduction of immunosuppression (179, 180). Mortality in SOT patients with cryptocococcosis ranges from 20-40%.
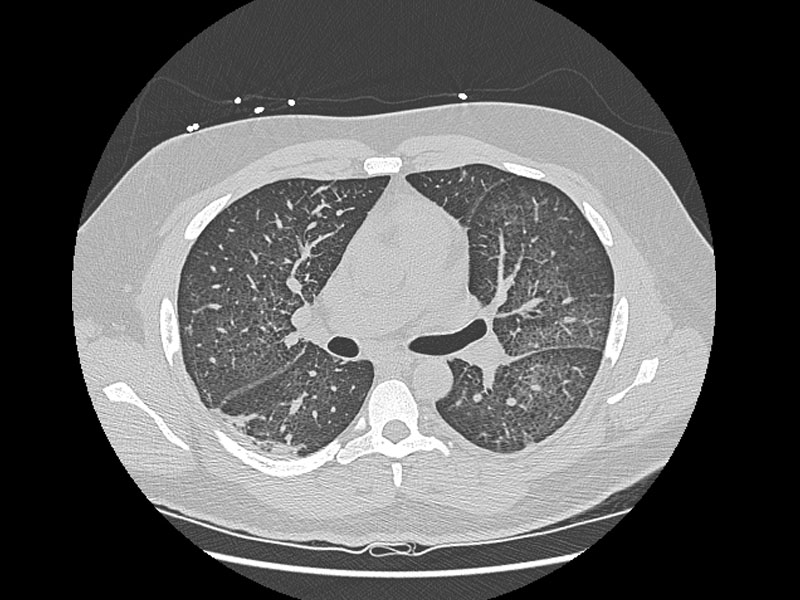
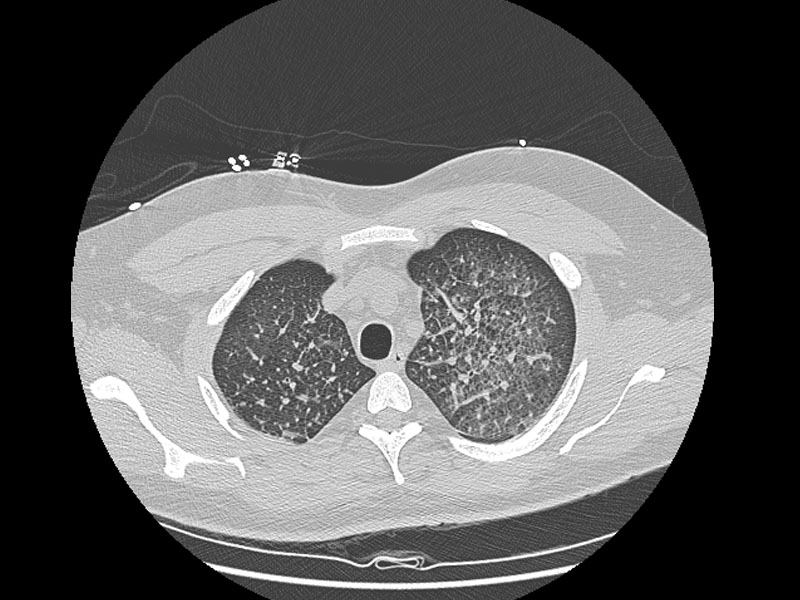
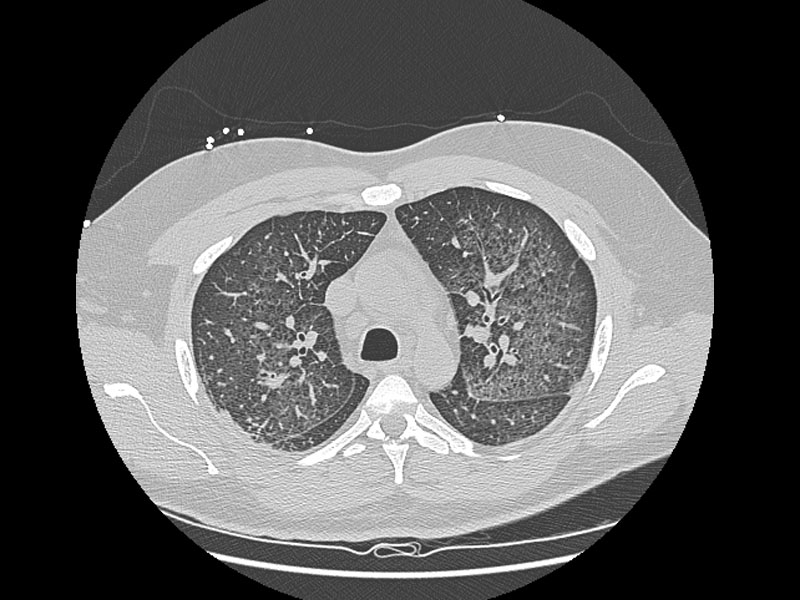
FEVER AND PULMONARY INFILTRATES
Pneumonia accounts for 30-80% of all infections in SOT recipients and for a great majority of the episodes of fever (41% of all febrile infections during the first 7 days of ICU stay and 14% of those after 7 days) (173). The incidence of bacterial pneumonia is highest in recipients of heart-lung (22%) and liver transplants (13-34%), intermediate in recipients of heart transplants (5%), and lowest in renal transplant patients (1 to 2%) (30, 52, 151). Pneumonias occur predominantly in the early postoperative period, especially in the patients who require prolonged ventilation or are colonized or infected before transplantation. Up to 95% of post-transplant pneumonias occur within the first 6 months (26). The net state of immunosuppression is the main risk factor in late-onset pneumonias. The crude mortality of bacterial pneumonia in solid organ transplantation has exceeded 40% in most series (71, 98).
The type of transplant, time of appearance, specific risk factors of the patient, rate of progression, and the radiological manifestations may help in the differential diagnosis and in the selection of empirical therapy. The classification of pneumonias occurring in SOT recipients according to the site of acquisition- community acquired or nosocomial- is more difficult than in other populations since the incubation period of opportunistic pathogens is highly variable and these patients are frequently exposed to the health care system.
The differential diagnosis of a SOT with a lung infiltrate is broad and includes infectious and non infectious causes. Singh et al have recently analyzed 40 orthotopic liver transplant (OLT) recipients who developed lung infiltrates in the ICU (174). The etiology was: pulmonary edema 40%, pneumonia 38%, atelectasias 10%, acute respiratory distress syndrome (ARDS) 8%, contusion 3%, and unknown 3%. The signs that suggest an infectious origin were: CPISscore >6 (73% vs. 6%), abnormal temperature (73% vs 28%), and creatinine level >1.5 mg/dl (80% vs 50%) (174).
Regarding the infectious etiology, opportunistic microorganisms account for 60% of the pneumonias, nosocomial pathogens for 25% and community-acquired bacteria and mycobacteria for 15% in a series in heart transplant (HT) patients (26). However, the relative importance of each group of microorganisms is influenced by the time after transplantation when the pneumonia is diagnosed. In this series, Gram-negative rods (median 9 days) and Gram-positive cocci (11 days) caused early pneumonias, while fungi (80 days), M. tuberculosis, Nocardia spp. (145 days) and virus (230 days) appeared later. In another series of heart transplant patients, etiology could be established in 61% of the pneumonias and bacteria caused 91% of the cases, fungi 9% and virus 6% (71). Table 1 summarizes the common etiologies according to their radiological pattern and the form of presentation. We shall briefly review the characteristics of the predominant pathogens causing pneumonia in SOT patients.
CMV used to be the most frequent organism infecting the lungs in solid transplant recipients, but the incidence has significantly decreased with the widespread use of antiviral prophylaxis. CMV may be the sole causal agent of pneumonia after SOT or appear as a co-pathogen with other microorganisms such as P. jiroveci or Aspergillus (129). The main risk factor is primary infection. CMV pneumonitis commonly manifests as diffuse interstitial infiltrates, but focal and even nodular infiltrates are described in up to one-third of patients. CMV may cause severe pneumonia with ARDS requiring ICU admission 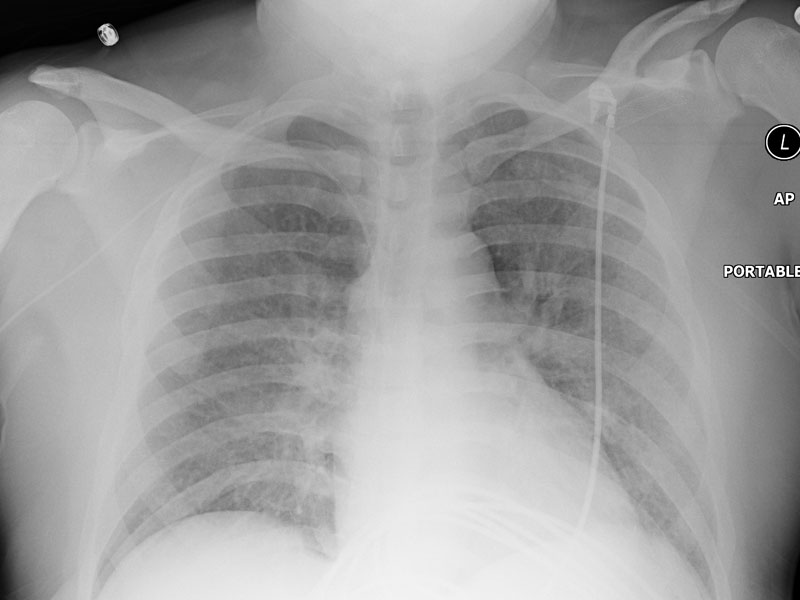 . Herpes simplex (87, 201) and VZV may also cause pneumonia in the transplant population, sometimes before the appearance of skin rash or “sine herpete”. HHV-6 has been reported to cause diverse clinical symptoms including fever, skin rash, pneumonia, bone marrow suppression, encephalitis, and rejection.
. Herpes simplex (87, 201) and VZV may also cause pneumonia in the transplant population, sometimes before the appearance of skin rash or “sine herpete”. HHV-6 has been reported to cause diverse clinical symptoms including fever, skin rash, pneumonia, bone marrow suppression, encephalitis, and rejection.
{kind=link}
{kind=link}
{kind=link}
The respiratory viruses, particularly respiratory syncytial virus, influenza, parainfluenza, adenovirus, and picornaviruses are increasingly recognized as significant pathogens in this population. Respiratory syncytial virus and influenza have been found to be the most common of the respiratory viruses causing severe infections in transplant recipients (14, 79, 80, 97, 185, 197, 204). Adenovirus may cause pneumonia, occasionally with dysfunction of the allograft (42). Finally, a new virus, the human metapneumovirus may be a significant respiratory pathogen in immunocompromised transplant recipients (68). Respiratory viruses may be associated with high morbidity, particularly in lung transplant recipients and may appear as “culture-negative” pneumonia. Molecular methods, such as reverse transcription-polymerase chain reaction assays allow the identification of respiratory viruses in BAL specimen (43). Advances in prevention, particularly with regard to infection control practices, and to lesser extent treatment have had a substantial impact on the frequency and outcomes of this infection. New antiviral agents may lead to improved outcomes of picornavirus infections in this population.
Bacterial pneumonia may occur at any time after transplantation, but the period of greater risk is the first month after the procedure. Need for mechanical ventilation and intensive care in this period are among the most important predisposing factors. However, SOT recipients requiring mechanical ventilation in the ICU are also at increased risk of developing aspergillosis. In a series of liver transplant recipients, methicillin resistant S. aureus, P. aeruginosa andAspergillus caused 70% of all pneumonias in the ICU (173). All Aspergillus and 75% of MRSA pneumonias, but only 14% of the Gram-negative pneumonias occurred within 30 days of transplantation (70, 169).
Legionella should always be included in the differential diagnosis (41, 59, 129, 166). Legionella has been reported in 2-27% of SOT recipients with pneumonia, although the incidence has wide regional differences (5, 33, 99,132, 164). A prodrome of influenza-like symptoms is followed sometimes by an "explosive" pneumonia with patchy lobular or interstitial infiltrates on chest radiograph. High fever, hypothermia, abdominal pain, and mental status changes are sometimes seen. Pneumonia is the most common presentation, but some patients have only fever (59). Other less common manifestations are liver abscesses, pericarditis, cellulitis, peritonitis or hemodialysis fistula infections (81). Infiltrate is usually lobar, but Legionella must be included in the differential diagnosis of lung nodules, cavitating pneumonia and lung abscess (41). Legionella infections can be overlooked unless specialized laboratory methodology (cultured on selective media, urinary antigen) are applied routinely on all cases of pneumonia (166). Routine culture on the water supply for Legionella is recommended in all transplant centers and in intensive care units with cases of legionellosis (28). The use of impregnated filter systems may help prevent nosocomial legionellosis in high-risk patient care areas (198).
Late community-acquired bacterial pneumonias are tenfold more frequent in cardiac transplant recipients than in the general population (2.6 cases/100 cardiac transplants) (26). The etiological agents are similar to those of the general population (S. pneumoniae, H. influenzae, etc) with the exception of lung transplant patients who may suffer recurrent pneumonias caused by P. aeruginosa or B. cepacia (137).
Rhodococcus equi (116, 118) and Nocardia (73, 130, 146, 196, 203) are well-known causes of respiratory tract infection in transplant recipients. They should be considered in sub-acute late pneumonias appearing radiologically as multiple bilateral nodules. The incidence of nocardiosis has been significantly reduced since the widespread use of cotrimoxazole prophylaxis. However, its use does not exclude nocardiosis. Nocardia farcinica may be resistant to cotrimoxazole prophylaxis and cause particularly aggressive disease (203). The coexistence of CNS, and/or skin lesions should suggest the possibility of Nocardia. Clinicians should consider R. equi when evaluating a solid organ recipient with an asymptomatic lung nodule, particularly when cultures fail to identify Mycobacteria, Nocardia or fungal organisms. Clinical microbiology laboratories should be alerted when a Rhodoccocus equi infection is suspected, since it could be mistaken for a contaminant diphtheroid and will not respond to the standard empirical therapy.
The frequency of Mycobacterium tuberculosis disease in receptors of solid organ transplantation in most developed countries ranges from 1.2% to 6.4%, but in transplant patients living in areas of high-level endemicity it might reach up to 15% (117, 124, 138, 172). Although there is a large regional variability, in general SOT incidence is 20-74 times higher than in the general population, with a mortality rate of up to 30%. The most frequent form of acquisition of tuberculosis after transplantation is the reactivation of latent tuberculosis in patients with previous exposure. Tuberculosis develops a mean of 9 months after transplantation (0.5 to 13 months). Risk factors for early onset tuberculosis are non-renal transplant, allograft rejection, immunosuppressive therapy with OKT3 or anti-T cell antibodies and previous exposure to M. tuberculosis without prophylaxis. Clinical presentation is frequently atypical and diverse, with unsuspected and elusive sites of involvement (115). A large series of tuberculosis in transplant recipients described pulmonary involvement in 51% of patients, extrapulmonary tuberculosis in 16% and disseminated infection in 33% (172). In lungs, radiographic appearance may vary between focal or diffuse interstitial infiltrates, nodules, pleural effusion or cavitary lesions. Manifestations include fever of unknown origin, allograft dysfunction, gastrointestinal bleeding, peritonitis or ulcers. In transplant patients, M. tuberculosis infection was also described in skin, muscle, osteoarticular system, CNS, genitourinary tract, lymph nodes, larynx, adrenal glands and thyroid (1, 172). Ocular lesions may be an early way to detect dissemination (18). Coinfection with other pathogens is not uncommon. Treatment requires awareness and careful consideration of interactions between antituberculous drugs and immunosuppressive therapy. A high index of suspicion is recommended, so if diagnosis of pneumonia is uncertain in the first 24-48 hours, specific cultures and PCR for M. tuberculosis should be considered.
Fungal infections have been reported to occur in 5-20% of SOT recipients and although these have decreasing proportionally, the absolute numbers of patients with fungal infections have increased as more transplantation procedures are performed each year. Rates vary according to the type of transplant recipient and are greatly influenced by the degree of immunosuppression, use of prophylaxis, rate of surgical complications, and of renal failure among the transplant population. Fungal pathogens more likely to cause pneumonia in this population are Aspergillus, P. jiroveci, Candida spp. and Cryptococcus spp.
The incidence of aspergillosis has decreased in SOT patients and ranges now from 0.3% in kidney transplant to 3.9% in pancreas recipients (45). In lung and heart-lung transplantation, the incidence may approach 14-35% if no prophylaxis is employed, but has significantly decreased since universal or preemptive prophylaxis is administered (34, 101). invasive aspergillosis (IA) is usually an early event and most patients were still in the ICU with evidence of organ dysfunction when the disease was diagnosed (138, 167). In heart transplantation, Aspergillus is the predominant fungal isolate and accounts for 38% of all lung nodular lesions (120). It appears a median of 50±63 days after heart transplantation (HT) (112). Aspergillus may appear late after transplantation, mainly in patients with a neoplastic disease (44).
After heart transplantation, postoperative hemodialysis, CMV disease, reoperation and other episodes of aspergillosis in the ward close to the transplantation date are major risk factors for invasive aspergillosis (IA). Retransplantation is also an independent risk factor (167, 170). However, aspergillosis may develop in low-risk patients after significant exposure (122). Accordingly, intensive care units caring for transplant patients should maintain a good quality of air control (109).
Pulmonary involvement is documented in 90% of the cases, but CNS or disseminated manifestations may predominate (139). In single lung transplant patients, invasive aspergillosis (IA) more commonly affects the native lung than the transplanted lung and may arise immediately post-operatively due to pre-existent disease in pretransplant immunosuppressed patients. In lung and heart-lung transplant recipients the types of disease presentation include bronchial anastomosis dehiscence, vascular anastomosis erosion, bronchitis, tracheobronchitis, invasive lung disease, aspergilloma, empyema, disseminated disease, endobronchial stent obstruction and mucoid bronchial impaction. Ulcerative tracheobronchitis is a semi-invasive disease involving the anastomosis site and the large airways (78).
Although the lung is the primary site of infection, other presentations have also been described (surgical wound, primary cutaneous infection, infection of a biloma, endocarditis, endophthalmitis, etc). The isolation of Aspergillusfrom any SOT recipient sample is always a warning clue. Voriconazole is the mainstay of therapy; although combined therapy may be indicated in specially severe cases (114).
Scedosporium species are increasingly recognized as significant pathogens, particularly in immunocompromised hosts. These fungi now account for ~25% of all non-Aspergillus mould infections in organ transplant recipients (64). We have found that 46% of Scedosporium infections in organ transplant recipients were disseminated and that patients may occasionally present with shock and sepsis- like syndrome (65). Fungemia and CNS involvement is especially frequent when S. prolificans is involved. Overall, mortality rate for Scedosporium infections in transplant recipients was 58%. Scedosporium species are generally resistant to amphotericin B. S. prolificans in particular is also resistant to most currently available antifungal agents. When adjusted for disseminated infection, voriconazole as compared to amphotericin B was associated with a lower mortality rate that approached statistical significance (p=.06).
Pneumocystis jiroveci (former P. carinii) is now rarely seen in SOT receiving prophylaxis. In the absence of prophylaxis, its incidence is approximately 5%, and may approach 80% in lung transplant recipients. PCP was diagnosed a median of 75 days after transplant (range, 37-781 d). Clinical presentation is usually acute (less than 48 hours) with fever (89%), dyspnea (84%), dry cough (74%), and hypoxia (63%). Cytomegalovirus was isolated from lung or blood in 74% of patients. Chest X-ray usually showed interstitial pneumonia (84%). Some patients required ventilatory support. Mortality was 26% (107). Week-end prophylaxis (1 double-strength tablet, 160/800 mg, every 12 hours on Saturdays and Sundays) has been shown to be a practical and an efficacious approach to prevention that has also eliminated Listeria and Nocardia infections.
Cryptococcus neoformans affects the lung in 40-55% of solid organ transplants with cryptocococcosis (181, 182). However, the disease is uncommon and appears a median of 24 months after transplantation (1 mo – 17y). An immune reconstitution syndrome- like entity may occur in organ transplant recipients with C. neoformans infection. This entity may be interpreted as failure of therapy. Immunomodulatory agents may have a role as adjunctive therapy in such cases (180).
Although Candida is frequently recovered from the lower respiratory tract of ventilated patients, Candida pneumonia is exceedingly rare (36). It has been reported in lung transplant recipients and the diagnosis requires histological confirmation, since the recovery of Candida may represent colonization. In lung transplant recipients, infection with Candida may be associated with very severe complications such as the necrosis of bronchial anastomoses (50, 60, 134,136).
Pneumonia in SOT patients predominantly shows alveolar or interstitial infiltrates of variable extent in the chest X-rays. However, nodular lesions are not uncommon (Table 2). The differential diagnosis of a lung nodule in a normal host includes many malignant and benign processes. However, in immunosuppressed patients the most common causes are potentially life-threatening opportunistic infections that are potentially treatable and preventable. We have detected single or multiple lung nodules on the chest radiograph in 10% of our heart transplant patients (108). CT is more sensitive than standard chest X-ray in identifying the number of lesions and may assist guided biopsy. It is important to bear in mind that some drugs, such as sirolimus, may cause pulmonary infiltrates, dyspnea, cough, fatigue and sometimes fever (56). Characteristic radiological changes are bilateral lower zone haziness. The presentation range from insidious to fulminant and usually there is a rapid response to sirolimus withdrawal.
As evident from the aforementioned discussion, pneumonia in SOT recipients is a complex clinical syndrome with multiple potential etiologies. Considering the high mortality of some of these pathogens, prompt detection of the etiology, although challenging at times, is of the utmost importance. As with other critically ill patients, differentiating pneumonia from other etiologies of pulmonary infiltrates can be extremely difficult.
Etiologic diagnosis is mandatory since only 50% of the empiric treatments of pneumonia in heart transplant patients are appropriate (26). For this reason, rapid and reliable diagnostic procedures that guide antimicrobial treatment are necessary. A variety of diagnostic techniques may be used to establish the diagnosis and these need to carefullyl tailored to an individual patient. The expected rate of bacteremia in patients with pneumonia is 16-29% (175). Once pneumonia is identified, blood cultures, respiratory samples for culture of bacteria, mycobacteria, fungi and viruses and urine for Legionella and S. pneumoniae antigen detection must be submitted to the laboratory (if possible, before starting antimicrobials). Direct microscopic examination of the respiratory samples (Gram stain, potassium hydroxide or cotton blue preparations) are very useful and in one series were positive in 3/5 cases of aspergillosis and in 3/4 cases of nocardiosis (108). Demonstration of pathogenic microorganisms (M. tuberculosis, Legionella, Cryptococcus spp., R. equi or P. jiroveci) in a sputum sample is diagnostic. PCR techniques may help improving diagnostic sensitivity (124). A bronchoscopic sample with bronchial biopsy is preferable for CMV, Aspergillus or P. jiroveci pneumonia. If pleural fluid is present it should also be analyzed. In patients with focal nodular infiltrates, percutaneous needle aspiration is superior to BAL. Transbronchial biopsy in conjunction with BAL is particularly valuable in lung transplant recipients for differentiating allograft rejection from CMV pneumonitis. Open lung biopsy should be reserved only for patients with progressive infiltrate refractory to antimicrobial agents in whom other diagnostic procedures have not yielded a diagnosis. A serum sample should also be submitted.
In our series of nodular lesions in heart patients, etiological diagnosis was established within a median of 8 days (0-24) and a median of 1.8 invasive techniques per patient were necessary. Overall diagnostic yield was 60% for transtracheal aspiration, 70% for BAL and 75% for transthoracic aspiration. BAL was the first positive diagnostic approach in 58% of the patients. The only complications were a minor pneumothorax after a transbronchial biopsy and minorhemoptysis after a transthoracic needle aspiration.
Pneumonia is an infection with the highest related mortality rate in SOT recipients so prompt empirical therapy is highly recommended for patients in critical conditions after obtaining adequate samples and in most SOT recipients with a CPIS score >6 (174). The selection of empirical therapy should be guided by the characteristics of the patient and the clinical situation.
POSTSURGICAL INFECTIONS
Complications in the proximity of the surgical area may be a cause of fever in the transplant patient. In the early post–transplantation period, renal and pancreas transplant recipients may develop perigraft hematomas, lymphoceles, and urinary fistula. Incisional surgical site infections were detected in 55/1400 consecutive renal transplants in Spain a median of 20 days after transplantation. The most frequently isolated pathogens were Escherichia coli (31.7%),Pseudomonas aeruginosa (13.3%), Enterococcus faecalis (11.6%), Enterobacter spp. (10%), and coagulase-negative staphylococci (8.3%). Risk factors were diabetes, and use of sirolimus (148). Surgical site infection requires rapid debridement and effective antimicrobial therapy and should prompt the exclusion of adjacent cavities or organ involvement.
In orthotopic liver transplant (OLT) recipients intra-abdominal infections may be responsible of 50% of bacterial complications and cause significant morbidity (58); they include intraabdominal abscesses, biliary tree infections and peritonitis. In non-abdominal transplantations, intraabdominal infections may be caused by pre-existing problems such as biliary tract lithiasis, diverticulitis, CMV disease, etc.
These complications should always be considered in patients with fever and a complicated surgery, particularly if transfusion of large volumes of blood products were required, use of a choledochojejunostomy as opposed to choledochostomy (duct-to-duct) for biliary anastomosis, or in the face of vascular problems of the allograft (for example thrombosis of the hepatic artery or the ischemia of the biliary tract may lead to cholangitis and liver abscesses). Occasionally, the complications will appear after the performance of a procedure such as a liver biopsy or a cholangiography.
In a series published by Singh et al. the biliary tree was the origin of 9% of infections associated with fever in the ICU (173). Biliary anastomosis leaks may result in peritonitis or perihepatic collections, cholangitis, or liver abscesses (144, 152, 191). Orthotopic liver transplant (OLT) recipients are especially predisposed to cholangitis. Recent data suggest that duct-to-duct biliary anastomosis stented with a T tube tends to be associated with more postoperative complications (37). A percutaneous aspirate with culture of the fluid is required to confirm infection. Culture of T-tube is unreliable, since it may only reflect colonization. Infected bilomas present with fever, abdominal pain and elevated hepatic enzymes and are confirmed by CT and radiographically guided aspiration. Most patients will respond to percutaneous drainage and prolonged anti-infective therapy.
In a recent series including 1222 liver transplant (LT) patients, 107 (8.7%) developed a surgical site infection. The predominant infection sites were incisional wound (53 episodes) and peritonitis (40 episodes). Enterococcus spp.,Escherichia coli, Staphylococcus aureus, and Acinetobacter baumannii were the predominant causative agents. Choledochojejunal or hepatico-jejunal reconstruction (odds ratio, 4.2; 95% confidence interval, 1.6-10.7), previous liver or kidney transplant (odds ratio, 2.6; 95% confidence interval, 1.1-6.3), and more than 4 red blood cell units transfused (odds ratio, 2.0; 95% confidence interval, 1.1-3.4) were independently associated with the development of surgical site infections (10).
Hepatic abscess is usually a later complications frequently associated with hepatic artery thrombosis (187). In one series, median time from transplant to hepatic abscess was 386 days (range 25-4,198). Clinical presentation of hepatic abscess was similar to that described in non-immunosuppressed patients. Occasionally the only manifestations are unexplained fever and relapsing subacute bacteremia. In fact 40-45% of the liver abscesses are associated with bacteremia. Prolonged antibiotic therapy, drainage, and even re-transplantation may be necessary in these patients. Catheter drainage was successful in 70% of cases. Mortality rate was 42% (190).
Ultrasonography, CT or MRI of the abdomen are the techniques used to identify intraabdominal or biliary infections. However, sterile fluid collections are so common after liver transplantation that an aspirate is necessary to diagnose infection.
Heart transplant recipients are at risk for mediastinitis and infection at the aortic suture line, with resultant mycotic aneurysm, and lung transplantation recipients are at risk for disruption of the bronchial anastomosis. In general, surgical problems leading to devitalized tissue, anastomotic disruption, or fluid collections markedly predispose the transplant recipient to potentially lethal infection. Among a population of 292 consecutive patients who underwent heart transplantation in Spain, 17 surgical site infections were documented in 14 patients (4.8%) after a median of 14 days after transplantation (range 3–75). Coagulase-negative Staphylococcus (7 cases) was the most common pathogen (147).
In febrile heart and lung transplant recipients, the possibility of mediastinitis (2-9%) should always be considered (38, 53). Heart patients have a higher risk of postsurgical mediastinitis and sternal osteomyelitis than other heart surgical patients (106). It may initially manifest simply as fever or bacteremia of unknown origin and inflammatory signs in the sternal wound, sternal dehiscence and purulent drainage may appear later. The most commonly involved microorganisms are staphylococci but gram-negative rods represent at least a third of our cases. Mycoplasma, Legionella, mycobacteria and other less common pathogens should be suspected in “culture-negative” wound infections (86,192). A bacteremia of unknown origin during the first month after heart transplantation should always suggest the possibility of mediastinitis. Risk factors are prolonged hospitalization before surgery, early chest re-exploration, low output syndrome in adults and nasal carriage of S. aureus before surgery (126). Therapy consists of surgical debridement and repair, and antimicrobial therapy given for 3 to 6 weeks.
URINARY TRACT INFECTIONS
Urinary tract infections (UTI) are the most common form of bacterial complication following renal transplantation (121, 193). The incidence in patients not receiving prophylaxis varies from 5 to 48% in different series (46, 72,186). Pre-transplant history of UTI increases the risk of infection after transplantation (153). Some authors have found a cumulative incidence of acute pyelonephritis (APN) after KT of 18.7%. The risk of developing APN was higher in female (64%) than in male recipients, and correlated with the frequency of recurrent UTIs and rejection episodes. Multivariate analysis revealed that APN represents an independent risk factor associated with the decline of renal function (p = 0.034) (140).
The most common pathogens include enterobacteriaceae, enterococci, staphylococci and Pseudomonas. However, other less frequent microorganisms like Salmonella, Candida or Corynebacterium urealyticum pose specific management problems in this population (91). It is also important to remember the possibility of infection caused by unusual pathogens like Mycoplasma hominis, M. tuberculosis or BK and JC viruses. BKV may cause allograft injury after SOT, but fever is not a common manifestation (40, 123).
Examination of the iliac fossa is particularly important after kidney transplantation. Tenderness, erythema, fluctuance or increase in the allograft size may indicate the presence of a deep infection or rejection. Ultrasound or CT-guided aspiration may facilitate the diagnosis. Unless another source of fever is readily apparent, any febrile kidney transplant patient with an abrupt deterioration of renal function should be treated with empiric antibacterial therapy aimed at gram negative bacteria, including Pseudomonas aeruginosa, after first obtaining blood and urine cultures (143). Prolonged administration of antimicrobial therapy has been typically recommended for the treatment of early infections, although no double-blind, comparative study is available (121). Antimicrobial resistance to drugs commonly used, such as cotrimoxazole or quinolones is common, so they should not be selected for empirical therapy of severe UTIs (160). Recurrent late infections may result in graft scarring and deterioration of renal function (35).
GASTROINTESTINAL INFECTIONS
The presence of gastrointestinal manifestations, with or without fever, is common in SOT recipients. It has been reported that if properly questioned, 51-68% of transplant recipients have GI complaints ranging from mild to severe, and more than 15% will warrant endoscopic, radiologic or surgical procedures (47, 93, 163, 175).
Abdominal pain is the most frequently-reported complaint (20-61%), followed by dyspepsia (52%), diarrhea (40-51%), and nausea (34%). Digestive perforation was the GI disorder that most affected patients daily living (47). Other manifestations include odynophagia or dysphagia, jaundice, gastrointestinal bleeding, hepatobiliary or pancreatic complications, peritonitis, intraabdominal infections or just weight loss (82). If ascites is present, it should be immediately analyzed and properly cultured to exclude peritonitis. Samples should be sent to the laboratory before starting antimicrobial therapy. We recommend bedside inoculation in blood-culture bottles due to its higher yield of positive results.
CMV and C. difficile are the most common causes of proven infectious diarrhea in SOT patients in the developed world (4, 48, 75, 77). Accordingly, the first step of the management of a patient with fever and diarrhea or abdominal pain should be directed to exclude these pathogens. If clinical manifestations persist despite exclusion of these, a wider differential diagnosis and more sophisticated diagnostic techniques should be considered since there are reports of SOT recipients with infections caused by Norwalk virus (39), rotavirus (189), adenovirus (83), Epstein-Barr virus (61), Cryptosporidium parvum (32), Isospora belli (12, 76) etc.
It is important to remember that the etiology of a diarrheal episode will vary widely depending upon the geographic region. In a recent Turkish study where 52 diarrheal episodes among 43 SOT recipients were evaluated, a specific diagnosis was established in 43 patients (82.6%) and was infectious in 33 of the 43 episodes (76.7%). The most common pathogens were: Giardia lamblia (9), Cryptosporidium parvum (7), cytomegalovirus (6) and Clostridium difficile(3). Non-infectious etiologies were found for 10 episodes (23.3%) (9).
We will begin by reviewing the main clinical manifestations and the diagnostic and therapeutic approach to CMV gastrointestinal disease and to C. difficile associated diarrhea in transplant recipients (CDAC).
CMV may involve any part of the gastrointestinal tract, although duodenum and stomach are the most frequent sites involved (74). Infection of the upper gastrointestinal tract with CMV used to be a major cause of morbidity in transplant patients (155), although its incidence is much lower in recent years (94). The natural history of CMV disease associated with solid organ transplantation has evolved as a result of the widespread use of potent immunosuppressant drugs and prolonged antiviral prophylaxis. The disease has practically disappeared during the first months after transplantation, but late severe forms are now encountered (17).
Most common clinical presentation of gastrointestinal CMV disease include fever, abdominal pain or diarrhea; nausea and gastrointestinal bleeding. The diarrhea may occasionally be severe enough to precipitate renal failure (3). Some patients present with isolated elevation of the alkaline phosphatase (3). The possibility of colonic perforation in corticosteroid–treated patients or gastrointestinal CMV disease should always be considered.
The diagnosis is many times suggested by the presence of ulcers in the endoscopy. In one series 53/201 heart transplant patients had persistent upper gastrointestinal symptoms. Of these 53 patients, 16 (30.2%) had diffuse erythema or ulceration of the gastric mucosa (14), esophagus (1), and duodenum (1) and positive biopsy results for CMV cultures (incidence, 8%). Recurrence was demonstrated in 6 patients (37.5%) who required repeated therapy withganciclovir. None of the 16 patients died as a result of gastrointestinal CMV infection. Endoscopic lesions caused by CMV may sometimes have a stenosing or pseudoneoplastic appearance (95).
Practically all patients with gastrointestinal CMV will have a positive PCR in blood. However, occasionally, severe intestinal CMV disease may occur in patients with negative antigenemia, especially in patients on mycophenolate mofetil (105). PCR is also an accurate method for the detection of CMV in the mucosa of the gastrointestinal tract (142). Hypogammaglobulinemia should be excluded in patients with relapsing forms of CMV after solid organ transplantation (24, 156, 157). Differential diagnosis should include diverticulitis, intestinal ischemia, cancer, and EBV-associated lymphoproliferative disorders. Recommended therapy is intravenous ganciclovir, which can be followed by oral valganciclovir (85).
Solid organ transplant recipients have many risk factors for developing C. difficile associated diarrhea (CDAD): surgery, frequent hospital admissions, antimicrobials exposure and immunosuppression. Clostridium difficile should be suspected in transplant patients who present with nosocomial diarrhea, usually early after transplantation (6, 110, 125, 188, 202). C. difficile colitis accounted for 5% of all febrile episodes in orthotopic liver transplant (OLT) in the ICU (173).
Most common clinical presentation is diarrhea, which occasionally may be unusually severe (20, 100, 127). In a recent series, 5.7% of the kidney or pancreas transplant recipients developed fulminant CDAD that presented with toxic megacolon, and underwent colectomy. One of them died; the other patient survived after colectomy (75). Absence of diarrhea is a poor prognostic factor. In these cases significant leukocytosis may be a very useful clue and the pathogen may be demonstrated with a rectal swab. Occasionally patients present with an acute abdomen (159) or inflammatory pseudotumor (92).
Fresh stool samples should be analyzed for the presence of toxin producer C. difficile. The reference method for diagnosis is the cell culture cytotoxin test which detects toxin B in a cellular culture of human fibroblasts (20). Culture in specific media is also recommended since it allows resistance study, molecular analysis of the strains, and the performance of a ''second-look" cell culture assay that enhances the potential for diagnosis (19). C. difficile colitis may occur in coincidence with CMV gastrointestinal infection (110, 195).
The first step in managing diarrhea and colitis caused by C. difficile is discontinuation of the antibiotic therapy that precipitated the disease, whenever possible. About 15-25% of patients respond within a few days. Patients with severe disease should be treated with oral vancomycin or with IV metronidazole. Oral metronidazole (500 mg tid or 250 mg every 6 hrs) and standard dose oral vancomycin (125 mg every 6 hrs) can be used for patients with less sever forms (21). The administration of probiotics such as Saccharomyces boulardii, or Lactobacillus sp. for prophylaxis of CDAD remains controversial and we do not recommend these in critically ill patients since the occurrence of severe invasive disease by S. boulardii has been described (113).
Approximately 10-25% of the patients will suffer a relapse 3-10 days after treatment has been discontinued, even with no further antibiotic therapy. Relapse usually results from either failure to eradicate C. difficile spores from the colon or due to re-infection from the environment. Nearly all patients respond to another course of antibiotics if given early. The frequency of relapses does not seem to be affected by the antibiotic selected for treatment, the dose of these drugs, or the duration of treatment. Multiple relapses may be difficult to manage. Several measures have been suggested: gradual tapering of the dosage of vancomycin over 1-2 months, administration of "pulse-dose" vancomycin, use of anion-exchange resins to absorb C. difficile toxin A, administration of vancomycin plus rifampin or administration of immunoglobulins.
Infectious enteritis is especially frequent in intestinal transplant recipients (39%) and it is caused by viruses in two thirds of the cases. In a recent series there were 14 viral enteritis (one cytomegalovirus, eight rotavirus, fouradenovirus, one Epstein-Barr virus), three bacterial (C. difficile), and three protozoal infections (one Giardia lamblia, two Cryptosporidium). Bacterial infections tended to present earlier than the viral infections, and the most frequent presenting symptom was diarrhea (207).
As noted earlier, immunosuppressive drugs such as mycophenolate mofetil (MMF), cyclosporine A (CSA), tacrolimus, and sirolimus are all known to be associated with diarrhea. The incidence of diarrhea ranged from 13-38% for regimens containing CSA and MMF and 29-64% for regimens with tacrolimus and MMF (23). However a systematic diagnostic approach should be performed before reducing the dose of these immunosuppressive agents. Lymphoproliferative disorder, de novo inflammatory bowel disease (54), or colon cancer may present also as diarrhea. Flare-up of preexisting IBD is also not uncommon after liver transplantation. However, the cause of acute diarrhea remains unidentified in 1 of 3 patients (48). All types of diarrhea significantly increased the risk of graft loss in a large series of kidney transplant recipients (23).
REFERENCES
1. Aguado JM, Herrero JA, Gavalda J, Torre-Cisneros J, Blanes M, Rufi G, Moreno A, Gurgui M, Hayek M, Lumbreras C, Cantarell C. Clinical presentation and outcome of tuberculosis in kidney, liver, and heart transplant recipients in Spain. Spanish Transplantation Infection Study Group, GESITRA. Transplantation 1997;63:1278-86. [PubMed]
2. Alexander BD. Cryptococcosis after solid organ transplantation. Transpl Infect Dis 2005;7:1-3. [PubMed]
3. Alhyraba M, Grim SA, Benedetti E, Clark NM. Unusual presentation of cytomegalovirus enteritis after liver and kidney transplantation. Transpl Infect Dis 2007;9:343-6. [PubMed]
4. Altiparmak MR, Trablus S, Pamuk ON, Apaydin S, Sariyar M, Ozturk R, Ataman R, Serdengecti K, Erek E. Diarrhoea following renal transplantation. Clin Transplant 2002;16:212-6. [PubMed]
5. Ampel NM, Wing EJ. Legionella infection in transplant patients. Semin Respir Infect 1990;5:30-7. [PubMed]
6. Apaydin S, Altiparmak MR, Saribas S, Ozturk R. Prevalence of Clostridium difficile toxin in kidney transplant recipients. Scand J Infect Dis 1998;30:542. [PubMed]
7. Arduino RC, Johnson PC, Miranda AG. Nocardiosis in renal transplant recipients undergoing immunosuppression with cyclosporine. Clin Infect Dis 1993;16:505-12. [PubMed]
8. Arnold SJ, Kinney MC, McCormick MS, Dummer S, Scott MA. Disseminated toxoplasmosis. Unusual presentations in the immunocompromised host. Arch Pathol Lab Med 1997;121:869-73. [PubMed]
9. Arslan H, Inci EK, Azap OK, Karakayali H, Torgay A, Haberal M. Etiologic agents of diarrhea in solid organ recipients. Transpl Infect Dis 2007;9:270-5 Epub 2007 May 19. [PubMed]
10. Asensio A, Ramos A, Cuervas-Mons V, Cordero E, Sanchez-Turrion V, Blanes M, Cervera C, Gavalda J, Aguado JM, Torre-Cisneros J. Effect of antibiotic prophylaxis on the risk of surgical site infection in orthotopic liver transplant. Liver Transpl 2008;14:799-805. [PubMed]
11. Aslani J, Eizadi M, Kardavani B, Khoddami-Vishteh HR, Nemati E, Hoseini SM, Einollahi B. Mucormycosis after kidney transplantations: Report of seven cases. Scand J Infect Dis 2007;39:703-6. [PubMed]
12. Atambay M, Bayraktar MR, Kayabas U, Yilmaz S, Bayindir Y. A rare diarrheic parasite in a liver transplant patient: Isospora belli. Transplant Proc 2007;39:1693-5. [PubMed]
13. Baden LR, Katz JT, Franck L, Tsang S, Hall M, Rubin RH, Jarcho J. Successful toxoplasmosis prophylaxis after orthotopic cardiac transplantation with trimethoprim-sulfamethoxazole. Transplantation 2003;75:339-43. [PubMed]
14. Barton TD, Blumberg EA. Viral pneumonias other than cytomegalovirus in transplant recipients. Clin Chest Med 2005;26:707-20, viii. [PubMed]
15. Benito N, Ricart MJ, Pumarola T, Marcos MA, Oppenheimer F, Camacho AM. Infection with human herpesvirus 6 after kidney-pancreas transplant. Am J Transplant 2004;4:1197-9. [PubMed]
16. Bonham CA, Dominguez EA, Fukui MB, Paterson DL, Pankey GA, Wagener MM, Fung JJ, Singh N. Central nervous system lesions in liver transplant recipients: prospective assessment of indications for biopsy and implications for management. Transplantation 1998;66(12):1596-604. [PubMed]
17. Boobes Y, Al Hakim M, Dastoor H, Bernieh B, Abdulkhalik S. Late cytomegalovirus disease with atypical presentation in renal transplant patients: case reports. Transplant Proc 2004;36(6):1841-3. [PubMed]
18. Bouza E, Merino P, Muñoz P, Sánchez-Carrillo C, Yáñez J, Cortés C. Ocular tuberculosis: A prospective study in a General Hospital. Medicine (Baltimore). 1997;76:53-61. [PubMed]
19. Bouza E, Pelaez T, Alonso R, Catalan P, Muñoz P, Creixems MR. "Second-look" cytotoxicity: an evaluation of culture plus cytotoxin assay of Clostridium difficile isolates in the laboratory diagnosis of CDAD. J Hosp Infect 2001;48(3):233-7.[PubMed]
20. Bouza E, Muñoz P, Alonso R. Clinical manifestations, treatment and control of infections caused by Clostridium difficile. Clin Microbiol Infect 2005;11(Suppl 4):57-64. [PubMed]
21. Bouza E, Burillo A, Muñoz P. Antimicrobial Therapy of Clostridium difficile-Associated Diarrhea. Med Clin North Am 2006;90(6):1141-63. [PubMed]
22. Bouza E, Loeches B, Muñoz P. Fever of unknown origin in solid organ transplant recipients. Infect Dis Clin North Am 2007;21(4):1033-54, ix-x. [PubMed]
23. Bunnapradist S, Neri L, Wong W, Lentine KL, Burroughs TE, Pinsky BW, Takemoto SK, Schnitzler MA. Incidence and risk factors for diarrhea following kidney transplantation and association with graft loss and mortality. Am J Kidney Dis 2008;51(3):478-86. [PubMed]
24. Carbone J, Sarmiento E, Palomo J, Fernandez-Yañez J, Muñoz P, Bouza E, Rodriguez-Molina J, Lanio N, Fernandez-Cruz E. The potential impact of substitutive therapy with intravenous immunoglobulin on the outcome of heart transplant recipients with infections. Transplant Proc 2007;39(7):2385-8. [PubMed]
25. Cemillan CA, Alonso-Pulpon L, Burgos-Lazaro R, Millan-Hernandez I, del Ser T, Liano-Martinez H. [Neurological complications in a series of 205 orthotopic heart transplant patients]. Rev Neurol 2004;38(10):906-12. [PubMed]
26. Cisneros JM, Muñoz P, Torre-Cisneros J, Gurguí M, Rodríguez-Hernandez JM, Aguado JM, Echaniz A, the Spanish Transplantation Infection Study Group a. Pneumonia after heart transplantation: a multiinstitutional study. Clin Infect Dis 1998;27:324-31. [PubMed]
27. Conrath J, Mouly-Bandini A, Collart F, Ridings B. Toxoplasma gondii retinochoroiditis after cardiac transplantation. Graefes Arch Clin Exp Ophthalmol 2003;241(4):334-8 Epub 2003 Mar 22. [PubMed]
28. Chaberny IF, Ziesing S, Gastmeier P. [Legionella prevention in intensive care units]. Anasthesiol Intensivmed Notfallmed Schmerzther 2004;39(3):127-31. [PubMed]
29. Chang FY, Singh N, Gayowski T, Wagener MM, Marino IR. Fever in liver transplant recipients: changing spectrum of etiologic agents. Clin Infect Dis 1998;26(1):59-65. [PubMed]
30. Chang GC, Wu CL, Pan SH, Yang TY, Chin CS, Yang YC, Chiang CD. The diagnosis of pneumonia in renal transplant recipients using invasive and noninvasive procedures. Chest 2004;125(2):541-7. [PubMed]
31. Delisle MB, Bouissou H, Saidi A. What's new in cerebral pathology in acquired immune deficiencies? Pathol Res Pract 1986;181(1):85-92. [PubMed]
32. Denkinger CM, Harigopal P, Ruiz P, Dowdy LM. Cryptosporidium parvum-associated sclerosing cholangitis in a liver transplant patient. Transpl Infect Dis 2008;10(2):133-6. Epub 2007 Jul 1. [PubMed]
33. Dowling JN, Pasculle AW, Frola FN, Zaphyr MK, Yee RB. Infections caused by Legionella micdadei and Legionella pneumophila among renal transplant recipients. J Infect Dis 1984;149(5):703-13. [PubMed]
34. Dummer JS, Lazariashvilli N, Barnes J, Ninan M, Milstone AP. A survey of anti-fungal management in lung transplantation. J Heart Lung Transplant 2004;23(12):1376-81. [PubMed]
35. Dupont PJ, Psimenou E, Lord R, Buscombe JR, Hilson AJ, Sweny P. Late recurrent urinary tract infections may produce renal allograft scarring even in the absence of symptoms or vesicoureteric reflux. Transplantation 2007;84(3):351-5.[PubMed]
36. el-Ebiary M, Torres A, Fabregas N, de la Bellacasa JP, Gonzalez J, Ramirez J, del Bano D, Hernandez C, Jimenez de Anta MT. Significance of the isolation of Candida species from respiratory samples in critically ill, non-neutropenic patients. An immediate postmortem histologic study. Am J Respir Crit Care Med 1997;156(2 Pt 1):583-90. [PubMed]
37. Elola-Olaso AM, Diaz JC, Gonzalez EM, Garcia Garcia I, Domene PO, Olivares S, Sanz RG, Suarez YF, Calvo J. Preliminary study of choledochocholedochostomy without T tube in liver transplantation: a comparative study. Transplant Proc 2005;37(9):3922-3. [PubMed]
38. Farinas MC, Gald Peralta F, Bernal JM, Rabasa JM, Revuelta JM, Gonzalez-Macias J. Suppurative mediastinitis after open-heart surgery: a case-control study covering a seven-year period in Santander, Spain. Clin Infect Dis 1995;20(2):272-9.[PubMed]
39. Florescu DF, Hill LA, McCartan MA, Grant W. Two cases of Norwalk virus enteritis following small bowel transplantation treated with oral human serum immunoglobulin. Pediatr Transplant 2008;12(3):372-5 Epub 2008 Jan 24.[PubMed]
40. Fogeda M, Muñoz P, Luque A, Morales MD, Bouza E. Cross-sectional study of BK virus infection in pediatric kidney transplant recipients. Pediatr Transplant 2007;11(4):394-401. [PubMed]
41. Fraser TG, Zembower TR, Lynch P, Fryer J, Salvalaggio PR, Yeldandi AV, Stosor V. Cavitary Legionella pneumonia in a liver transplant recipient. Transpl Infect Dis 2004;6(2):77-80. [PubMed]
42. Friedrichs N, Eis-Hubinger AM, Heim A, Platen E, Zhou H, Buettner R. Acute adenoviral infection of a graft by serotype 35 following renal transplantation. Pathol Res Pract 2003;199(8):565-70. [PubMed]
43. Garbino J, Gerbase MW, Wunderli W, Deffernez C, Thomas Y, Rochat T, Ninet B, Schrenzel J, Yerly S, Perrin L, Soccal PM, Nicod L, Kaiser L. Lower respiratory viral illnesses: improved diagnosis by molecular methods and clinical impact. Am J Respir Crit Care Med 2004;170(11):1197-203 Epub 2004 Sep 10. [PubMed]
44. Gavalda J, Len O, San Juan R, Aguado JM, Fortun J, Lumbreras C, Moreno A, Muñoz P, Blanes M, Ramos A, Rufi G, Gurgui M, Torre-Cisneros J, Montejo M, Cuenca-Estrella M, Rodriguez-Tudela JL, Pahissa A. Risk factors for invasive aspergillosis in solid-organ transplant recipients: a case-control study. Clin Infect Dis 2005;41(1):52-9 Epub 2005 May 26. [PubMed]
45. Gavaldà J, Len O, Rovira M, Borrell N, Cámara R, Cisneros J, Fortún J, Lumbreras C, Montejo M, Muñoz P, Peña F, Ramos A, De La Torre J, Cuenca-Estrella M, Rodríguez-Tudela J, Pahissa A. Epidemiology of Invasive Fungal Infections (IFI) in Solid Organ (SOT) and Hematopoeitic Stem Cell (HSCT) Transplant Recipients: a Prospective Study from RESITRA. 45th Interscience Conference On Antimicrobial Agents And Chemoterapy 2005:(M-990/461).
46. Ghasemian SM, Guleria AS, Khawand NY, Light JA. Diagnosis and management of the urologic complications of renal transplantation. Clin Transplant 1996;10(2):218-23. [PubMed]
47. Gil-Vernet S, Amado A, Ortega F, Alarcon A, Bernal G, Capdevila L, Crespo JF, Cruzado JM, De Bonis E, Esforzado N, Fernandez AM, Franco A, Hortal L, Jimenez C. Gastrointestinal complications in renal transplant recipients: MITOS study. Transplant Proc 2007;39(7):2190-3. [PubMed]
48. Ginsburg PM, Thuluvath PJ. Diarrhea in liver transplant recipients: etiology and management. Liver Transpl 2005;11(8):881-90. [PubMed]
49. Goldberg SL, Cicogna CE, Rowley SD, Pecora AL. Vaccinations against infectious diseases in hematopoietic stem cell transplant recipients. Oncology (Huntingt) 2003;17(4):539-54, 559; discussion 559-60, 564-5. [PubMed]
50. Grossi P, Farina C, Fiocchi R, Dalla Gasperina D. Prevalence and outcome of invasive fungal infections in 1,963 thoracic organ transplant recipients: a multicenter retrospective study. Italian Study Group of Fungal Infections in Thoracic Organ Transplant Recipients. Transplantation 2000;70(1):112-6. [PubMed]
51. Guitard J, Kamar N, Mouzin M, Borde JS, Tran-Van T, Durand D, Rostaing L. Sulfadiazine-related obstructive urinary tract lithiasis: an unusual cause of acute renal failure after kidney transplantation. Clin Nephrol 2005;63(5):405-7.[PubMed]
52. Gupta RK, Jain M, Garg R. Pneumocystis carinii pneumonia after renal transplantation. Indian J Pathol Microbiol 2004;47(4):474-6. [PubMed]
53. Gurgui M, Muñoz P. [Infection in heart transplantation]. Enferm Infecc Microbiol Clin 2007;25(9):587-97; quiz 598.[PubMed]
54. Halim MA, Al-Otaibi T, Elsisi A, El-Sayed A, Nair P, Said T, Balaha MA, Nampoory M. Denovo post renal transplantation inflammatory bowel disease. Saudi J Kidney Dis Transpl 2008;19(4):624-6. [PubMed]
55. Hall WA, Martinez AJ, Dummer JS, Griffith BP, Hardesty RL, Bahnson HT, Lunsford LD. Central nervous system infections in heart and heart-lung transplant recipients. Arch Neurol 1989;46(2):173-7. [PubMed]
56. Haydar AA, Denton M, West A, Rees J, Goldsmith DJ. Sirolimus-induced pneumonitis: three cases and a review of the literature. Am J Transplant 2004;4(1):137-9. [PubMed]
57. Higashibeppu N, Oida E, Furutani H, Segawa H, Adachi T, Fukuda K. [Anesthesia for living-donor liver transplantation in a patient with adult polycystic liver disease]. Masui 2003;52(3):264-7. [PubMed]
58. Ho MC, Wu YM, Hu RH, Ko WJ, Ni YH, Chang MH, Yang PM, Lai MY, Lin MH, Lin HY, Lee PH. Surgical complications and outcome of living related liver transplantation. Transplant Proc 2004;36(8):2249-51. [PubMed]
59. Horbach I, Fehrenbach FJ. Legionellosis in heart transplant recipients. Infection 1990;18(6):361-3. [PubMed]
60. Horvath J, Dummer S, Loyd J, Walker B, Merrill WH, Frist WH. Infection in the transplanted and native lung after single lung transplantation. Chest 1993;104(3):681-5. [PubMed]
61. Hranjec T, Bonatti H, Roman AL, Sifri C, Borowitz SM, Barnes BH, Flohr TR, Pruett TL, Sawyer RG, Schmitt TM. Benign transient hyperphosphatasemia associated with epstein-barr virus enteritis in a pediatric liver transplant patient: a case report. Transplant Proc 2008;40(5):1780-2. [PubMed]
62. Husain S, Wagener MM, Singh N. Cryptococcus neoformans infection in organ transplant recipients: variables influencing clinical characteristics and outcome. Emerg Infect Dis 2001;7(3):375-81. [PubMed]
63. Husain S, McCurry K, Dauber J, Singh N, Kusne S. Nocardia infection in lung transplant recipients. J Heart Lung Transplant 2002;21(3):354-9. [PubMed]
64. Husain S, Alexander BD, Muñoz P, Avery RK, Houston S, Pruett T, Jacobs R, Dominguez EA, Tollemar JG, Baumgarten K, Yu CM, Wagener MM, Linden P, Kusne S, Singh N. Opportunistic mycelial fungal infections in organ transplant recipients: emerging importance of non-Aspergillus mycelial fungi. Clin Infect Dis 2003;37(2):221-9 Epub 2003 Jul 9. [PubMed]
65. Husain S, Muñoz P, Forrest G, Alexander BD, Somani J, Brennan K, Wagener MM, Singh N. Infections due to Scedosporium apiospermum and Scedosporium prolificans in transplant recipients: clinical characteristics and impact of antifungal agent therapy on outcome. Clin Infect Dis 2005;40(1):89-99 Epub 2004 Dec 8. [PubMed]
66. Ionescu DN, Dacic S. Persistent fever in a lung transplant patient. Arch Pathol Lab Med 2005;129(6):e153-4. [PubMed]
67. Islam MN, Cohen DM, Celestina LJ, Ojha J, Claudio R, Bhattacharyya IB. Rhinocerebral zygomycosis: an increasingly frequent challenge: update and favorable outcomes in two cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104(5):e28-34. [PubMed]
68. Ison MG, Hayden FG. Viral infections in immunocompromised patients: what's new with respiratory viruses? Curr Opin Infect Dis 2002;15(4):355-67. [PubMed]
69. Jarquin-Valdivia AA, Wijdicks EF, McGregor C. Neurologic complications following heart transplantation in the modern era: decreased incidence, but postoperative stroke remains prevalent. Transplant Proc 1999;31(5):2161-2. [PubMed]
70. Jensen WA, Rose RM, Hammer SM, al. e. Pulmonary complications of orthotopic liver transplantation. Transplantation 1986;42(6):484. [PubMed]
71. Jimenez-Jambrina M, Hernandez A, Cordero E, Gurgui M, Alonso L, Blanes M, Muñoz P, Peña F, Cisneros J, Resitra Network. Pneumonia after Heart Transplantation in the XXI Century: a Multicenter Prospective Study. 45th Interscience Conference On Antimicrobial Agents And Chemoterapy 2005:(K-1561/370).
72. Kahan BD, Flechner SM, Lorber MI, Golden D, Conley S, Van Buren CT. Complications of cyclosporine-prednisone immunosuppression in 402 renal allograft recipients exclusively followed at a single center for from one to five years. Transplantation 1987;43(2):197-204. [PubMed]
73. Kahraman S, Genctoy G, Arici M, Cetinkaya Y, Altun B, Caglar S. Septic arthritis caused by Nocardia asteroides in a renal transplant recipient. Transplant Proc 2004;36(5):1415-8. [PubMed]
74. Kaplan B, Meier-Kriesche HU, Jacobs MG, Friedman G, Bonomini L, DeFranco P, Gelfand E, Mulgaonkar S. Prevalence of cytomegalovirus in the gastrointestinal tract of renal transplant recipients with persistent abdominal pain. Am J Kidney Dis 1999;34(1):65-8. [PubMed]
75. Keven K, Basu A, Re L, Tan H, Marcos A, Fung JJ, Starzl TE, Simmons RL, Shapiro R. Clostridium difficile colitis in patients after kidney and pancreas-kidney transplantation. Transpl Infect Dis 2004;6(1):10-4. [PubMed]
76. Koru O, Araz RE, Yilmaz YA, Erguven S, Yenicesu M, Pektas B, Tanyuksel M. Case report: Isospora belli infection in a renal transplant recipent. Turkiye Parazitol Derg 2007;31(2):98-100. [PubMed]
77. Kottaridis PD, Peggs K, Devereux S, Goldstone AH, Mackinnon S. Simultaneous occurrence of Clostridium difficile and Cytomegalovirus colitis in a recipient of autologous stem cell transplantation. Haematologica 2000;85(10):1116-7.[PubMed]
78. Kramer MR, Denning DW, Marshall SE, Ross DJ, Berry G, Lewiston NJ, Stevens DA, Theodore J. Ulcerative tracheobronchitis after lung transplantation. A new form of invasive aspergillosis. Am Rev Respir Dis 1991;144(3 Pt 1):552-6.[PubMed]
79. Kumar D, Erdman D, Keshavjee S, Peret T, Tellier R, Hadjiliadis D, Johnson G, Ayers M, Siegal D, Humar A. Clinical impact of community-acquired respiratory viruses on bronchiolitis obliterans after lung transplant. Am J Transplant 2005;5(8):2031-6. [PubMed]
80. Kumar D, Humar A. Emerging viral infections in transplant recipients. Curr Opin Infect Dis 2005;18(4):337-41. [PubMed]
81. La Scola B, Michel G, Raoult D. Isolation of Legionella pneumophila by centrifugation of shell vial cell cultures from multiple liver and lung abscesses. J Clin Microbiol 1999;37(3):785-7. [PubMed]
82. Laskin B, Goebel J. Clinically "silent" weight loss associated with mycophenolate mofetil in pediatric renal transplant recipients. Pediatr Transplant 2008;12(1):113-6. [PubMed]
83. Lee BE, Pang XL, Robinson JL, Bigam D, Monroe SS, Preiksaitis JK. Chronic norovirus and adenovirus infection in a solid organ transplant recipient. Pediatr Infect Dis J 2008;27(4):360-2. [PubMed]
84. Lehto JT, Halme M, Tukiainen P, Harjula A, Sipponen J, Lautenschlager I. Human herpesvirus-6 and -7 after lung and heart-lung transplantation. J Heart Lung Transplant 2007;26(1):41-7. [PubMed]
85. Len O, Gavalda J, Aguado JM, Borrell N, Cervera C, Cisneros JM, Cuervas-Mons V, Gurgui M, Martin-Davila P, Montejo M, Muñoz P, Bou G, Carratala J, Torre-Cisneros J, Pahissa A. Valganciclovir as treatment for cytomegalovirus disease in solid organ transplant recipients. Clin Infect Dis 2008;46(1):20-7. [PubMed]
86. Levin T, Suh B, Beltramo D, Samuel R. Aspergillus mediastinitis following orthotopic heart transplantation: case report and review of the literature. Transpl Infect Dis 2004;6(3):129-31. [PubMed]
87. Liebau P, Kuse E, Winkler M, Schlitt HJ, Oldhafer K, Verhagen W, Flik J, Pichlmayr R. Management of herpes simplex virus type 1 pneumonia following liver transplantation. Infection 1996;24(2):130-5. [PubMed]
88. Limaye AP, Perkins JD, Kowdley KV. Listeria infection after liver transplantation: report of a case and review of the literature. Am J Gastroenterol 1998;93(10):1942-4. [PubMed]
89. Ljungman P, Singh N. Human herpesvirus-6 infection in solid organ and stem cell transplant recipients. J Clin Virol 2006;37 Suppl 1:S87-91. [PubMed]
90. Loire R, Tabib A, Bastien O. [Fatal aspergillosis after cardiac transplantation. About 26 cases]. Ann Pathol 1993;13(3):157-63. [PubMed]
91. Lopez-Medrano F, Garcia-Bravo M, Morales JM, Andres A, San Juan R, Lizasoain M, Aguado JM. Urinary tract infection due to Corynebacterium urealyticum in kidney transplant recipients: an underdiagnosed etiology for obstructive uropathy and graft dysfunction-results of a prospective cohort study. Clin Infect Dis 2008;46(6):825-30. [PubMed]
92. Lykavieris P, Fabre M, Pariente D, Lezeau YM, Debray D. Clostridium difficile colitis associated with inflammatory pseudotumor in a liver transplant recipient. Pediatr Transplant 2003;7(1):76-9. [PubMed]
93. Machnicki G, Pefaur J, Gaite L, Linchenko AM, Raimondi C, Schiavelli R, Otero A, Margolis MK. Gastrointestinal (GI)-Specific patient reported outcomes instruments differentiate between renal transplant patients with or without GI symptoms: results from a South American cohort. Health Qual Life Outcomes 2008;6(1):53. [PubMed]
94. Maes B, Hadaya K, de Moor B, Cambier P, Peeters P, de Meester J, Donck J, Sennesael J, Squifflet JP. Severe diarrhea in renal transplant patients: results of the DIDACT study. Am J Transplant 2006;6(6):1466-72. [PubMed]
95. Maiorana A, Torricelli P, Giusti F, Bellini N. Pseudoneoplastic appearance of cytomegalovirus-associated colitis in nonimmunocompromised patients: report of 2 cases. Clin Infect Dis 2003;37(5):e68-71 Epub 2003 Aug 13. [PubMed]
96. Marik PE. Fungal infections in solid organ transplantation. Expert Opin Pharmacother 2006;7(3):297-305. [PubMed]
97. Mazzone PJ, Mossad SB, Mawhorter SD, Mehta AC, Mauer JR. Cell-mediated immune response to influenza vaccination in lung transplant recipients. J Heart Lung Transplant 2004;23(10):1175-81. [PubMed]
98. Mermel LA, Maki DG. Bacterial pneumonia in solid organ transplantation. Semin Respir Infect 1990;5(1):10-29.[PubMed]
99. Miller R, Burton NA, Karwande SV, Jones KW, Doty DB, Gay WA, Jr. Early, aggressive open lung biopsy in heart transplant recipients. J Heart Transplant 1987;6(2):96-9. [PubMed]
100. Mistry B, Longo W, Solomon H, Garvin P. Clostridium difficile colitis requiring subtotal colectomy in a renal transplant recipient: a case report and review of literature. Transplant Proc 1998;30(7):3914. [PubMed]
101. Monforte V, Roman A, Gavalda J, Bravo C, Tenorio L, Ferrer A, Maestre J, Morell F. Nebulized amphotericin B prophylaxis for Aspergillus infection in lung transplantation: study of risk factors. J Heart Lung Transplant 2001;20(12):1274-81.[PubMed]
102. Montejo M, Ramon Fernandez J, Testillano M, Valdivieso A, Aguirrebengoa K, Varas C, Olaizola A, De Urbina JO. Encephalitis caused by human herpesvirus-6 in a liver transplant recipient. Eur Neurol 2002;48(4):234-5. [PubMed]
103. Moreno A, Cervera C, Gavalda J, Rovira M, de la Camara R, Jarque I, Montejo M, de la Torre-Cisneros J, Miguel Cisneros J, Fortun J, Lopez-Medrano F, Gurgui M, Muñoz P, Ramos A, Carratala J. Bloodstream infections among transplant recipients: results of a nationwide surveillance in Spain. Am J Transplant 2007;7(11):2579-86 Epub 2007 Sep 14. [PubMed]
104. Mrowka C, Heintz B, Reul J, Sieberth H. Cerebral tuberculoma 11 years after renal transplantation. Am J Nephrol 1998;18(6):557-9. [PubMed]
105. Mugnani G, Bergami M, Lazzarotto T, Bedani PL. [Intestinal infection by cytomegalovirus in kidney transplantation: diagnostic difficulty in the course of mycophenolate mofetil therapy]. G Ital Nefrol 2002;19(4):483-4. [PubMed]
106. Muñoz P, Menasalvas A, Bernaldo de Quiros JC, Desco M, Vallejo JL, Bouza E. Postsurgical mediastinitis: a case-control study. Clin Infect Dis 1997;25(5):1060-4. [PubMed]
107. Muñoz P, Muñoz RM, Palomo J, Rodriguez-Creixems M, Muñoz R, Bouza E. Pneumocystis carinii infection in heart transplant recipients. Efficacy of a weekend prophylaxis schedule. Medicine (Baltimore) 1997;76(6):415-22. [PubMed]
108. Muñoz P, Palomo J, Guembe P, Rodriguez-Creixems M, Gijon P, Bouza E. Lung nodular lesions in heart transplant recipients. J Heart Lung Transplant 2000;19(7):660-7. [PubMed]
109. Muñoz P, Burillo A, Bouza E. Environmental surveillance and other control measures in the prevention of nosocomial fungal infections. Clin Microbiol Infect 2001;7(Suppl 2):38-45. [PubMed]
110. Muñoz P, Palomo J, Yañez J, Bouza E. Clinical microbiological case: a heart transplant recipient with diarrhea and abdominal pain. Recurring Clostridium difficile infection. Clin Microbiol Infect 2001;7(8):451-2, 458-9. [PubMed]
111. Muñoz P, Arencibia J, Rodriguez C, Rivera M, Palomo J, Yañez J, Bouza E. Trimethoprim-sulfamethoxazole as toxoplasmosis prophylaxis for heart transplant recipients. Clin Infect Dis 2003;36(7):932-3; author reply 933. [PubMed]
112. Muñoz P, Rodriguez C, Bouza E, Palomo J, Yañez JF, Dominguez MJ, Desco M. Risk factors of invasive aspergillosis after heart transplantation: protective role of oral itraconazole prophylaxis. Am J Transplant 2004;4(4):636-43. [PubMed]
113. Muñoz P, Bouza E, Cuenca-Estrella M, Eiros JM, Perez MJ, Sanchez-Somolinos M, Rincon C, Hortal J, Pelaez T. Saccharomyces cerevisiae fungemia: an emerging infectious disease. Clin Infect Dis 2005;40(11):1625-34 Epub 2005 Apr 25.[PubMed]
114. Muñoz P, Singh N, Bouza E. Treatment of solid organ transplant patients with invasive fungal infections: should a combination of antifungal drugs be used? Curr Opin Infect Dis 2006;19(4):365-70. [PubMed]
115. Muñoz P, Rodriguez M, Giannella M, Vega A, Anaya F, Serrano MJ, Bouza E. A painful hand in a kidney transplant recipient. Nephrol Dial Transplant 2007;22(3):971-2. [PubMed]
116. Muñoz P, Palomo J, Guinea J, Yañez J, Giannella M, Bouza E. Relapsing Rhodococcus equi infection in a heart transplant recipient successfully treated with long-term linezolid. Diagn Microbiol Infect Dis 2008;60(2):197-9. [PubMed]
117. Muñoz P, Palomo J, Muñoz R, Rodríguez-Creixéms M, Pelaez T, Bouza E. Tuberculosis in heart transplant recipients. Clin Infect Dis 1995;21:398-402. [PubMed]
118. Muñoz P, Burillo A, Palomo J, Rodríguez-Creixéms M, Bouza E. Rhodococcus equi infection in transplant recipients: Case report and review of the literature. . Transplantation 1997;65:449-53. [PubMed]
119. Muñoz P, Bouza E. Postrransplant fever in critically ill transplant recipients. Infectious complications in transplant patients. Kluwer Academic publishers. 2000; N. Singh, JM Aguado editors. ISBN 0-7923-7972-1:133-148. [PubMed]
120. Muñoz P, Palomo J, Rodríguez-Creixéms M, Bouza E. Lung nodular lesion in Heart Transplant recipients. Heart and Lung Transplantation 2000;In Press. [PubMed]
121. Muñoz P. Management of urinary tract infections and lymphocele in renal transplant recipients. Clin Infect Dis 2001;33(Suppl 1):S53-7. [PubMed]
122. Muñoz P, Guinea J, Pelaez T, Duran C, Blanco JL, Bouza E. Nosocomial invasive aspergillosis in a heart transplant patient acquired during a break in the HEPA air filtration system. Transpl Infect Dis 2004;6(1):50-4. [PubMed]
123. Muñoz P, Fogeda M, Bouza E, Verde E, Palomo J, Banares R. Prevalence of BK virus replication among recipients of solid organ transplants. Clin Infect Dis 2005;41(12):1720-5 Epub 2005 Nov 10. [PubMed]
124. Muñoz P, Rodriguez C, Bouza E. Mycobacterium tuberculosis infection in recipients of solid organ transplants. Clin Infect Dis 2005;40(4):581-7 Epub 2005 Jan 25. [PubMed]
125. Muñoz P, Giannella M, Alcala L, Sarmiento E, Fernandez Yañez J, Palomo J, Catalan P, Carbone J, Bouza E. Clostridium difficile-associated diarrhea in heart transplant recipients: is hypogammaglobulinemia the answer? J Heart Lung Transplant 2007;26(9):907-14. [PubMed]
126. Muñoz P, Hortal J, Giannella M, Barrio JM, Rodríguez-Créixems M, Pérez MJ, Rincón C, Bouza E. Nasal carriage of S. aureus increases the risk of surgical site infection after major heart surgery. Journal of Hospital Infection 2007; 68(1):25-31. [PubMed]
127. Nadir A, Wright HI, Naz-Nadir F, Cooper DK, Zuhdi N, Van Thiel DH. Atypical Clostridium difficile colitis in a heart transplant recipient. J Heart Lung Transplant 1995;14(3):606-7. [PubMed]
128. Nash PJ, Avery RK, Tang WH, Starling RC, Taege AJ, Yamani MH. Encephalitis owing to human herpesvirus-6 after cardiac transplant. Am J Transplant 2004;4(7):1200-3. [PubMed]
129. Nichols L, Strollo DC, Kusne S. Legionellosis in a lung transplant recipient obscured by cytomegalovirus infection and Clostridium difficile colitis. Transpl Infect Dis 2002;4(1):41-5. [PubMed]
130. Nouza M, Prat V. [Lung infection after kidney transplantation. I. Etiology, pathogenesis and clinical picture]. Cas Lek Cesk 1990;129(21):641-4. [PubMed]
131. Nucci M. Emerging moulds: Fusarium, Scedosporium and Zygomycetes in transplant recipients. Curr Opin Infect Dis 2003;16(6):607-12. [PubMed]
132. Ogunc G, Ozdemir T, Vural T, Suleymanlar G, Akaydin M, Karpuzoglu T. [Legionnaires' disease following kidney transplantation]. Mikrobiyol Bul 1993;27(2):137-42. [PubMed]
133. Ortonne N, Ribaud P, Meignin V, Sarfati C, Esperou H, Devergie A, Gluckman E, Socie G, Janin A. Toxoplasmic pneumonitis leading to fatal acute respiratory distress syndrome after engraftment in three bone marrow transplant recipients. Transplantation 2001;72(11):1838-40. [PubMed]
134. Palmer SM, Perfect JR, Howell DN, Lawrence CM, Miralles AP, Davis RD, Tapson VF. Candidal anastomotic infection in lung transplant recipients: successful treatment with a combination of systemic and inhaled antifungal agents. J Heart Lung Transplant 1998;17(10):1029-33. [PubMed]
135. Palomares M, Martinez T, Pastor J, Osuna A, Bravo JA, Alvarez G, Asensio C. Cerebral abscess caused by Nocardia asteroides in renal transplant recipient. Nephrol Dial Transplant 1999;14(12):2950-2. [PubMed]
136. Park KY, Park CH. Candida infection in a stent inserted for tracheal stenosis after heart lung transplantation. Ann Thorac Surg 2005;79(3):1054-6. [PubMed]
137. Patel R, Paya CV. Infections in solid-organ transplant recipients. Clin Microbiol Rev 1997;10(1):86-124. [PubMed]
138. Paterson DL, Singh N, Gayowski T, Marino IR. Pulmonary nodules in liver transplant recipients. Medicine 1998;77(1):50-8. [PubMed]
139. Paterson DL, Singh N. Invasive aspergillosis in transplant recipients. Medicine 1999;78(2):123-38. [PubMed]
140. Pelle G, Vimont S, Levy PP, Hertig A, Ouali N, Chassin C, Arlet G, Rondeau E, Vandewalle A. Acute pyelonephritis represents a risk factor impairing long-term kidney graft function. Am J Transplant 2007;7(4):899-907 Epub 2007 Feb 7. [PubMed]
141. Perez-Miralles F, Sanchez-Manso JC, Almenar-Bonet L, Sevilla-Mantecon T, Martinez-Dolz L, Vilchez-Padilla JJ. Incidence of and risk factors for neurologic complications after heart transplantation. Transplant Proc 2005;37(9):4067-70. [PubMed]
142. Peter A, Telkes G, Varga M, Sarvary E, Kovalszky I. Endoscopic diagnosis of cytomegalovirus infection of upper gastrointestinal tract in solid organ transplant recipients: Hungarian single-center experience. Clin Transplant 2004;18(5):580-4. [PubMed]
143. Peterson PK, Anderson RC. Infection in renal transplant recipients. Current approaches to diagnosis, therapy, and prevention. Am J Med 1986;81(1A):2-10. [PubMed]
144. Piecuch J, Witkowski K. Biliary tract complications following 52 consecutive orthotopic liver transplants. Ann Transplant 2001;6(1):36-8. [PubMed]
145. Ponticelli C, Campise MR. Neurological complications in kidney transplant recipients. J Nephrol 2005;18(5):521-8. [PubMed]
146. Queipo-Zaragoza JA, Broseta-Rico E, Alapont-Alacreu JM, Santos-Durantez M, Sanchez-Plumed J, Jimenez-Cruz JF. Nocardial infection in immunosuppressed kidney transplant recipients. Scand J Urol Nephrol 2004;38(2):168-73. [PubMed]
147. Ramos A, Asensio A, Munez E, Torre-Cisneros J, Blanes M, Carratala J, Segovia J, Muñoz P, Cisneros JM, Bou G, Aguado JM, Cervera C, Gurgui MM. Incisional surgical infection in heart transplantation. Transplant Infectious Diseases 2008;In Press. [PubMed]
148. Ramos A, Asensio A, Munez E, Torre-Cisneros J, Montejo M, Aguado JM, Cofan F, Carratala J, Len O, Cisneros JM. Incisional surgical site infection in kidney transplantation. Urology 2008;72(1):119-23 Epub 2008 Feb 15. [PubMed]
149. Razonable RR, Paya CV. The impact of human herpesvirus-6 and -7 infection on the outcome of liver transplantation. Liver Transpl 2002;8(8):651-8. [PubMed]
150. Renoult E, Georges E, Biava MF, Hulin C, Frimat L, Hestin D, Kessler M. Toxoplasmosis in kidney transplant recipients: a life-threatening but treatable disease. Transplant Proc 1997;29(1-2):821-2. [PubMed]
151. Renoult E, Georges E, Biava MF, Hulin C, Frimat L, Hestin D, Kessler M. Toxoplasmosis in kidney transplant recipients: report of six cases and review. Clin Infect Dis 1997;24(4):625-34. [PubMed]
152. Rerknimitr R, Sherman S, Fogel EL, Kalayci C, Lumeng L, Chalasani N, Kwo P, Lehman GA. Biliary tract complications after orthotopic liver transplantation with choledochocholedochostomy anastomosis: endoscopic findings and results of therapy. Gastrointest Endosc 2002;55(2):224-31. [PubMed]
153. Rizvi SJ, Chauhan R, Gupta R, Modi P. Significance of pretransplant urinary tract infection in short-term renal allograft function and survival. Transplant Proc 2008;40(4):1117-8. [PubMed]
154. Rodriguez C, Muñoz P, Rodriguez-Creixems M, Yañez JF, Palomo J, Bouza E. Bloodstream infections among heart transplant recipients. Transplantation 2006;81(3):384-91. [PubMed]
155. Sarkio S, Halme L, Arola J, Salmela K, Lautenschlager I. Gastroduodenal cytomegalovirus infection is common in kidney transplantation patients. Scand J Gastroenterol 2005;40(5):508-14. [PubMed]
156. Sarmiento E, Fernandez-Yañez J, Muñoz P, Palomo J, Rodriguez-Molina JJ, Bermejo J, Catalan P, Bouza E, Fernandez-Cruz E, Carbone J. Hypogammaglobulinemia after heart transplantation: use of intravenous immunoglobulin replacement therapy in relapsing CMV disease. Int Immunopharmacol 2005;5(1):97-101. [PubMed]
157. Sarmiento E, Rodriguez-Molina JJ, Fernandez-Yañez J, Palomo J, Urrea R, Muñoz P, Bouza E, Fernandez-Cruz E, Carbone J. IgG monitoring to identify the risk for development of infection in heart transplant recipients. Transpl Infect Dis 2006;8(1):49-53. [PubMed]
158. Sawyer RG, Crabtree TD, Gleason TG, Antevil JL, Pruett TL. Impact of solid organ transplantation and immunosuppression on fever, leukocytosis, and physiologic response during bacterial and fungal infections. Clin Transplant 1999;13(3):260-5. [PubMed]
159. Schenk P, Madl C, Kramer L, Ratheiser K, Kranz A, Zauner C, Stain C, Birsan T, Klepetko W, Muller C. Pneumatosis intestinalis with Clostridium difficile colitis as a cause of acute abdomen after lung transplantation. Dig Dis Sci 1998;43(11):2455-8. [PubMed]
160. Senger SS, Arslan H, Azap OK, Timurkaynak F, Cagir U, Haberal M. Urinary tract infections in renal transplant recipients. Transplant Proc 2007;39(4):1016-7. [PubMed]
161. Shin JH, Lee HK. Nocardial brain abscess in a renal transplant recipient. Clin Imaging 2003;27(5):321-4. [PubMed]
162. Simon DM, Levin S. Infectious complications of solid organ transplantations. Infect Dis Clin North Am 2001;15(2):521-49. [PubMed]
163. Singh G. The study of prolonged fevers. J Assoc Physicians India 2000;48(4):454-5. [PubMed]
164. Singh N, Muder RR, Yu VL, Gayowski T. Legionella infection in liver transplant recipients: implications for management. Transplantation 1993;56(6):1549-51. [PubMed]
165. Singh N, Gayowski T, Singh J, Yu VL. Invasive gastrointestinal zygomycosis in a liver transplant recipient: case report and review of zygomycosis in solid- organ transplant recipients. Clin Infect Dis 1995;20(3):617-20. [PubMed]
166. Singh N, Gayowski T, Wagener M, Marino IR, Yu VL. Pulmonary infections in liver transplant recipients receiving tacrolimus. Changing pattern of microbial etiologies. Transplantation 1996;61(3):396-401. [PubMed]
167. Singh N, Arnow PM, Bonham A, Dominguez E, Paterson DL, Pankey GA, Wagener MM, Yu VL. Invasive aspergillosis in liver transplant recipients in the 1990s. Transplantation 1997;64(5):716-20. [PubMed]
168. Singh N, Chang FY, Gayowski T, Marino IR. Infections due to dematiaceous fungi in organ transplant recipients: case report and review. Clin Infect Dis 1997;24(3):369-74. [PubMed]
169. Singh N, Gayowski T, Wagener MM. Intensive care unit management in liver transplant recipients: beneficial effect on survival and preservation of quality of life. Clin Transplant 1997;11(2):113-20. [PubMed]
170. Singh N, Gayowski T, Wagener MM, Doyle H, Marino IR. Invasive fungal infections in liver transplant recipients receiving tacrolimus as the primary immunosuppressive agent. Clin Infect Dis 1997;24(2):179-84. [PubMed]
171. Singh N, Gayowski T, Wagener MM, Marino IR. Clinical spectrum of invasive cryptococcosis in liver transplant recipients receiving tacrolimus. Clin Transplant 1997;11(1):66-70.[PubMed]
172. Singh N, Paterson DL. Mycobacterium tuberculosis infection in solid-organ transplant recipients: impact and implications for management. Clin Infect Dis 1998;27(5):1266-77. [PubMed]
173. Singh N, Chang FY, Gayowski T, Wagener M, Marino IR. Fever in liver transplant recipients in the intensive care unit. Clin Transplant 1999;13(6):504-11. [PubMed]
174. Singh N, Gayowski T, Wagener MM, Marino IR. Pulmonary infiltrates in liver transplant recipients in the intensive care unit. Transplantation 1999;67(8):1138-44. [PubMed]
175. Singh N. Postrransplant fever in critically ill transplant recipients. Infectious complications in transplant patients. Kluwer Academic publishers. 2000; N. Singh, JM Aguado editors. ISBN 0-7923-7972-1:113-132.
176. Singh N, Bonham A, Fukui M. Immunosuppressive-associated leukoencephalopathy in organ transplant recipients. Transplantation 2000;69(4):467-72. [PubMed]
177. Singh N, Husain S. Infections of the central nervous system in transplant recipients. Transpl Infect Dis 2000;2(3):101-11.[PubMed]
178. Singh N, Paterson DL. Encephalitis caused by human herpesvirus-6 in transplant recipients: relevance of a novel neurotropic virus. Transplantation 2000;69(12):2474-9. [PubMed]
179. Singh N, Lortholary O, Alexander BD, Gupta KL, John GT, Pursell K, Muñoz P, Klintmalm GB, Stosor V, del Busto R, Limaye AP, Somani J, Lyon M, Houston S, House AA, Pruett TL, Orloff S, Humar A, Dowdy L, Garcia-Diaz J, Kalil AC, Fisher RA, Husain S. An immune reconstitution syndrome-like illness associated with Cryptococcus neoformans infection in organ transplant recipients. Clin Infect Dis 2005;40(12):1756-61 Epub 2005 Apr 29. [PubMed]
180. Singh N, Lortholary O, Alexander BD, Gupta KL, John GT, Pursell K, Muñoz P, Klintmalm GB, Stosor V, delBusto R, Limaye AP, Somani J, Lyon M, Houston S, House AA, Pruett TL, Orloff S, Humar A, Dowdy L, Garcia-Diaz J, Fisher RA, Husain S. Allograft loss in renal transplant recipients with Cryptococcus neoformans associated immune reconstitution syndrome. Transplantation 2005;80(8):1131-3. [PubMed]
181. Singh N, Lortholary O, Alexander BD, Gupta KL, John GT, Pursell KJ, Muñoz P, Klintmalm GB, Stosor V, Del Busto R, Limaye AP, Somani J, Lyon M, Houston S, House AA, Pruett TL, Orloff S, Humar A, Dowdy LA, Garcia-Diaz J, Kalil AC, Fisher RA, Heitman J, Husain S. Antifungal management practices and evolution of infection in organ transplant recipients with cryptococcus neoformans infection. Transplantation 2005;80(8):1033-9. [PubMed]
182. Singh N, Alexander BD, Lortholary O, Dromer F, Gupta KL, John GT, del Busto R, Klintmalm GB, Somani J, Lyon GM, Pursell K, Stosor V, Muñoz P, Limaye AP, Kalil AC, Pruett TL, Garcia-Diaz J, Humar A, Houston S, House AA, Wray D, Orloff S, Dowdy LA, Fisher RA, Heitman J, Wagener MM, Husain S. Pulmonary cryptococcosis in solid organ transplant recipients: clinical relevance of serum cryptococcal antigen. Clin Infect Dis 2008;46(2):e12-8.[PubMed]
183. Singh N, Lortholary O, Dromer F, Alexander BD, Gupta KL, John GT, Busto R, Klintmalm GB, Somani J, Lyon GM, Pursell K, Stosor V, Muňoz P, Limaye AP, Kalil AC, Pruett TL, Garcia-Diaz J, Humar H, Houston S, House AA, Orloff S, Dowdy LA, Fisher RA, Heitman J, Wagener MM, Husain S. Central nervous system cryptococcosis in solid organ transplant recipients: clinical relevance of abnormal neuroimaging findings. Transplantation 2008;86(5):647-51. [PubMed]
184. Singhal S, Mehta J. Reimmunization after blood or marrow stem cell transplantation. Bone Marrow Transplant 1999;23(7):637-46. [PubMed]
185. Slifkin M, Doron S, Snydman DR. Viral prophylaxis in organ transplant patients. Drugs 2004;64(24):2763-92.[PubMed]
186. Sqalli TH, Laboudi A, Arrayhani M, Benamar L, Amar Y, Ouzeddoun N, Bayahia R, Rhou H. Urinary tract infections in renal allograft recipients from living related donors. Saudi J Kidney Dis Transpl 2008;19(4):551-3. [PubMed]
187. Stange BJ, Glanemann M, Nuessler NC, Settmacher U, Steinmuller T, Neuhaus P. Hepatic artery thrombosis after adult liver transplantation. Liver Transpl 2003;9(6):612-20. [PubMed]
188. Stelzmueller I, Goegele H, Biebl M, Wiesmayr S, Berger N, Tabarelli W, Ruttmann E, Albright J, Margreiter R, Fille M, Bonatti H. Clostridium difficile colitis in solid organ transplantation--a single-center experience. Dig Dis Sci 2007;52(11):3231-6 Epub 2007 Apr 4. [PubMed]
189. Stelzmueller I, Wiesmayr S, Swenson BR, Biebl M, Goegele H, Margreiter R, Bonatti H. Rotavirus enteritis in solid organ transplant recipients: an underestimated problem? Transpl Infect Dis 2007;9(4):281-5 Epub 2007 Jul 1. [PubMed]
190. Tachopoulou OA, Vogt DP, Henderson JM, Baker M, Keys TF. Hepatic abscess after liver transplantation: 1990-2000. Transplantation 2003;75(1):79-83. [PubMed]
191. Testa G, Malago M, Broelseh CE. Complications of biliary tract in liver transplantation. World J Surg 2001;25(10):1296-9. [PubMed]
192. Thaler F, Gotainer B, Teodori G, Dubois C, Loirat P. Mediastinitis due to Nocardia asteroides after cardiac transplantation. Intensive Care Med 1992;18(2):127-8. [PubMed]
193. Tolkoff Rubin NE, Rubin RH. Urinary tract infection in the immunocompromised host. Lessons from kidney transplantation and the AIDS epidemic. Infect Dis Clin North Am 1997;11(3):707-17. [PubMed]
194. Torre-Cisneros J, Lopez OL, Kusne S, Martinez AJ, Starzl TE, Simmons RL, Martin M. CNS aspergillosis in organ transplantation: a clinicopathological study. J Neurol Neurosurg Psychiatry 1993;56(2):188-93. [PubMed]
195. Veroux M, Puzzo L, Corona D, Buffone A, Tallarita T, Murabito P, Veroux P. Cytomegalovirus and Clostridium difficile ischemic colitis in a renal transplant recipient: a lethal complication of anti-rejection therapy? Urol Int 2007;79(2):177-9; discussion 180. [PubMed]
196. Vigano SM, Edefonti A, Ferraresso M, Ranzi ML, Grossi P, Righini A, Rusconi R, Santambrogio L, Ghio L. Successful medical treatment of multiple brain abscesses due to Nocardia farcinica in a paediatric renal transplant recipient. Pediatr Nephrol 2005;20(8):1186-8 Epub 2005 Jun 10. [PubMed]
197. Vilchez RA, McCurry K, Dauber J, Lacono A, Griffith B, Fung J, Kusne S. Influenza virus infection in adult solid organ transplant recipients. Am J Transplant 2002;2(3):287-91. [PubMed]
198. Vonberg RP, Eckmanns T, Bruderek J, Ruden H, Gastmeier P. Use of terminal tap water filter systems for prevention of nosocomial legionellosis. J Hosp Infect 2005;60(2):159-62. [PubMed]
199. Wagner FM, Reichenspurner H, Uberfuhr P, Weiss M, Fingerle V, Reichart B. Toxoplasmosis after heart transplantation: diagnosis by endomyocardial biopsy. J Heart Lung Transplant 1994;13(5):916-8. [PubMed]
200. Walker M, Zunt JR. Parasitic central nervous system infections in immunocompromised hosts. Clin Infect Dis 2005;40(7):1005-15 Epub 2005 Mar 2. [PubMed]
201. Weiss RL, Colby TV, Spruance SL, Salmon VC, Hammond ME. Simultaneous cytomegalovirus and herpes simplex virus pneumonia. Arch Pathol Lab Med 1987;111(3):242-5. [PubMed]
202. West M, Pirenne J, Chavers B, Gillingham K, Sutherland DE, Dunn DL, Matas AJ. Clostridium difficile colitis after kidney and kidney-pancreas transplantation. Clin Transplant 1999;13(4):318-23. [PubMed]
203. Wiesmayr S, Stelzmueller I, Tabarelli W, Bargehr D, Graziadei I, Freund M, Ladurner R, Steurer W, Geltner C, Mark W, Margreiter R, Bonatti H. Nocardiosis following solid organ transplantation: a single-centre experience. Transpl Int 2005;18(9):1048-53. [PubMed]
204. Wright JJ, O'Driscoll G. Treatment of parainfluenza virus 3 pneumonia in a cardiac transplant recipient with intravenous ribavirin and methylprednisolone. J Heart Lung Transplant 2005;24(3):343-6. [PubMed]
205. Wulf MW, van Crevel R, Portier R, Ter Meulen CG, Melchers WJ, van der Ven A, Galama JM. Toxoplasmosis after renal transplantation: implications of a missed diagnosis. J Clin Microbiol 2005;43(7):3544-7. [PubMed]
206. Zierer A, Melby SJ, Voeller RK, Guthrie TJ, Al-Dadah AS, Meyers BF, Pasque MK, Ewald GA, Moon MR, Moazami N. Significance of neurologic complications in the modern era of cardiac transplantation. Ann Thorac Surg 2007;83(5):1684-90. [PubMed]
207. Ziring D, Tran R, Edelstein S, McDiarmid SV, Gajjar N, Cortina G, Vargas J, Renz JF, Cherry JD, Krogstad P, Miller M, Busuttil RW, Farmer DG. Infectious enteritis after intestinal transplantation: incidence, timing, and outcome. Transplantation 2005;79(6):702-9. [PubMed]
Tables
Table 1. Clinical and Radiological Characteristics of CNS Infections According to Radiological Presentation
|
Time after transplantation |
Clinical characteristics |
Radiological characteristics |
Diagnostic approach |
|---|---|---|---|---|
FOCAL OR MASS LESSIONS |
|
|
|
|
Aspergillus fumigatus and other species |
First month |
Rapidly progressive alteration of mental status and seizures Focal neurologic symptoms less common Pulmonary involvement >80% Risk factors (renal failure, CMV disease, prolonged intubation, reintervention,..) |
Ring-enhanced lesions |
Lung CT Biopsy of skin lesions Respiratory tract samples for bacteria, Mycobacteria, fungi and Toxoplasma investigation Serum sample for Platelia, Glucatell, Mycobacterium PCR. If no skin or lung lessions present, perform brain biopsy |
Scedosporium or unusual mycelial fungi, e.g., phaeohyphomycetes ordematiaceous fungi |
3 mo.-2 years |
Alteration of mental status and seizures Skin or pulmonary involvement 20% |
Ring-enhanced lesions |
Brain biopsy usually needed |
Nocardia spp. |
1-6 months |
Pulmonary lesions >40% Skin lesions 20% Cases described despite cotrimoxazoleprophylaxis |
Ring-enhanced lesions |
Lung CT Biopsy of skin lesions Gram stain or modified Ziehl-Neelsen of respiratory or skin samples, prolonged culture
|
1-3 months |
Fever (74%), changes in mental status (45%), seizures (35%), headache (25%) Pulmonary lesions, chorioretinitis Recipient -/Donor +. Heart Tx recipient |
Multiple periventricular lesions |
Serology, culture, PCR, endomyocardial biopsy in HT |
|
MENINGOENCEPHALITIS |
|
|
|
|
1-2 months |
Coma (92%), seizures (25%) headaches (25%), speech disturbance (25%) and very high fever (25%) |
Neuroimaging abnormalities usually absent When detectable: nonenhancing, involve gray and white matter, and have no preferential cortical localization |
CSF pleocytosis 50%, elevated proteins 58% no hypoglycorrhachia. HHV-6 PCR in blood and CSF |
|
Late after Tx |
Rhomboencephalitis with cranial nerve palsies or pontomedullary signs |
|
Isolation in blood and CSF |
|
>3 m after Tx |
Chronic meningitis Disseminated infection (lung, skin, prostate) |
Leptomeningeal enhancement, hydrocephalus, parenchymal mass lesions or cryptococcomas |
CSF culture or positive CSF cryptococcal antigen Exclude intracranial hypertension |
Table 2. Diagnostic Approach and Potential Etiology of Lung Infiltrates in Solid Organ Transplant Recipients in Relation to the Radiological Pattern and to the Speed of Progression.
Radiological study : Chest X-ray, Thoracic CT |
||
|---|---|---|
Radiological pattern |
Acute onset* |
Subacute onset |
Consolidation |
Bacteria (S. pneumoniae Gram negative rods, Legionella, S. aureus) (1-2 weeks) Embolism, atelectasis Hemorrhage Acute graft rejection in lung transplant recipients Cytomegalovirus (2-3 month or later if prophylaxis) |
Aspergillus (36 days), Nocardia, Tuberculosis (9-23 months), Drugs P. jiroveci, Legionella, HSV, VZV, Toxoplasma Bronchiolitis obliterans
|
Interstitial |
Edema Transfusions [Bacteria] |
Virus (CMV, Influenza, Parainfluenza, RSV, EBV), P. jiroveci, Drugs [Fungi, Nocardia, Tuberculosis] |
Nodular |
[Bacteria, Edema] |
Fungi, Nocardia, R. equi, Tuberculosis [P. jiroveci, CMV] |
Other diagnostic assays |
||
§ Blood samples for bacterial cultures, for Mycobacteria and PCR for CMV § Serum sample: Mycoplasma, Chlamydia, Q fever, Legionella, Cryptococcus, § Sputum: for stains and rapid examination (Gram, Ziehl-Neelsen, potassium hydroxide or cotton blue preparations, stains for P. jiroveci) and for culture (bacteria if good quality, Mycobacteria with PCR, Nocardia, Fungus, Nocardia) § Urine: Antigen detection of Legionella and S. pneumoniae § BAL: same as for sputum § If clinically indicated: echocardiogram, § If skin lesions: biopsy and culture |
||
* These entities require attention in < 24 hours. Less common possibilities are within brackets.