
Approach to Fever and Back Pain
Authors: Michael J. Tan, MD, FACP
INTRODUCTION
Back pain and fever are not uncommon complaints in either the outpatient or inpatient setting. A thorough history and physical exam will aid the clinician in diagnosing the underlying cause. Localization of the discomfort in addition to pertinent cultures and radiographic studies are invaluable for identifying possible causes. When safe to do so, it is advisable to avoid starting antimicrobial therapy until an idea of the infectious process is established. This chapter will offer an approach to diagnosing potential causes of fever and back pain.
Problem
Back pain can occur at any level of the vertebral column; however, not all back pain is vertebral in origin. It is important to consider pain that is referred from other areas. For example, patients with acute cholecystitis will often have scapular pain. Patients with pancreatitis may have pain that shoots to the mid-back. Back pain is also not necessarily due to an infectious process, and non-infectious causes must be considered. See Table 1 for potential infectious and non-infectious causes based on their localizing areas. Identifying the location of the pain, and incorporating associated symptoms will help determine if the pain is referred or radiating, and whether or not it is due to an infectious process.
Differential Diagnosis
Certain musculoskeletal infections can occur at any vertebral level (Table 1). These include discitis, osteomyelitis, paraspinal and epidural abscesses. A recent history of bacteremia is often suggestive of potential bone or disc infection, especially if there is a history of prolonged bacteremia or pyogenic arthritis. Negative blood cultures, however, do no rule out a musculoskeletal infection. Common pathogens in patients who were recently bacteremic include Staphylococcus aureusand Streptococcus spp. In patients with newly diagnosed musculoskeletal infections of the spine with no recent history of bacteremia or surgery, occult infection and endocarditis should be ruled out. Common pathogens often seen after orthopedic procedures also include Staphylococcus aureus and Streptococcus spp., but also include coagulase-negative Staphylococci. Not common in the United States, but deserving mention, is vertebral tuberculosis (Pott’s Disease). As an extra-pulmonary manifestation of tuberculous disease, patients with spinal erosive changes seen on pathology or radiology should be assessed for tuberculosis risk factors, and appropriate staining should be done to look for acid-fast bacilli or granuloma formation. Some non-infectious causes of musculoskeletal disease include myopathy or muscle spasm, osteoarthritis, osteoporosis, disc herniation, compression fractures, and spinal stenosis. Metastatic disease to the spine should also be considered as approximately 30-70% of patients with a primary tumor have spinal metastasis at autopsy. It is the third most common site of metastasis after lung and liver. The most common malignancy sources of spinal metastasis include lung, breast, gastrointestinal, and prostate (Table 2). Non-infectious causes of back pain like sacroileitis may have an infectious inciting event such as brucellosis or infections that are associated with reactive arthritis. Table 1 provides a differential diagnosis of common problems presenting with fever and back pain. It should also be considered that fever may be associated with the condition, but it may also be coincidental.

Clinical Manifestations
Patients will present with varying degrees of fever and varying degrees of back pain. Pain can be localized or radiating. More often than not, symptoms alone will not help differentiate whether or not the presentation is infectious or non-infectious. Clues from history that help support a diagnosis of infectious etiology include history of a) previous infection in the particular area, b) previous bacteremia, c) intravenous drug use, d) recent trauma or surgery. Accordingly, a positive culture sample, pathology suggestive of infection (such as acute inflammation or necrotizing granulomas) or abnormal laboratory values (such as leukocytosis or elevated sedimentation rates) strongly support an infectious diagnosis. Clues that support non-infectious etiologies include history of a) rheumatologic disease, b) repeated negative cultures, c) radiographic evidence unsupporting of infection, and d) pathology or laboratory values not supporting of infection.
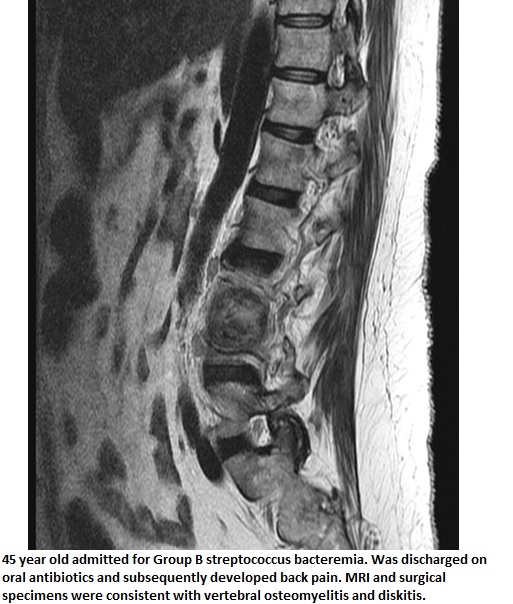
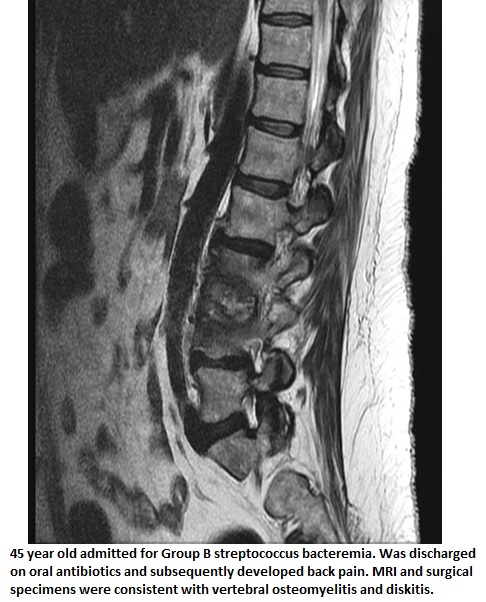
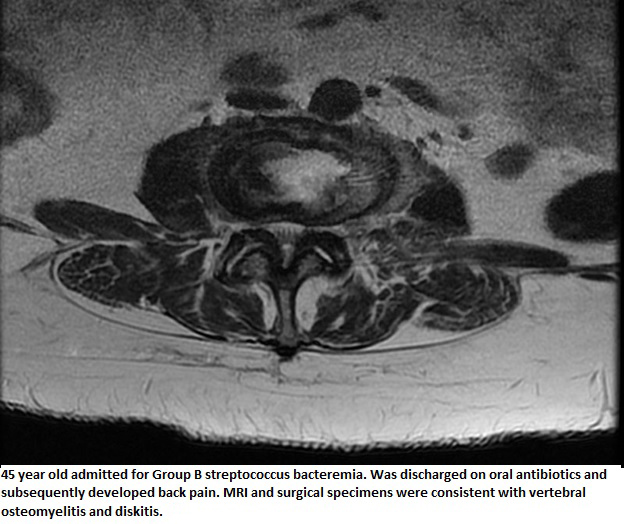
In addition to the clues from history that support a diagnosis of infectious etiology, certain elements should also serve as “red flags” or causes for concern. A patient with fever and pain back who has a history of intravenous drug abuse should undergo immediate imaging to evaluate for vertebral osteomyelitis or discitis associated with bacteremia and endocarditis. Similarly, a patient who was recently diagnosed with or treated for bacteremia who presents with new back pain should also be considered highly suspicious for vertebral osteomyelitis or discitis as a result of hematogenous seeding ![]() . This clinical suspicion should include hemodialysis patients and those with chronic indwelling intravenous lines. C-reactive protein and erythrocyte sedimentation rate tend to be very non-specific, however, when very elevated, should be used as a prompt for further evaluation and search for occult infection. See Table 3 for potential red flags that suggest an infectious etiology for back pain.
. This clinical suspicion should include hemodialysis patients and those with chronic indwelling intravenous lines. C-reactive protein and erythrocyte sedimentation rate tend to be very non-specific, however, when very elevated, should be used as a prompt for further evaluation and search for occult infection. See Table 3 for potential red flags that suggest an infectious etiology for back pain.
{kind=link}
{kind=link}
{kind=link}
Physical Examination
Complete physical examination should be performed; however, special attention to be paid to the particular systems of the presenting complaints. The following examination findings may increase suspicion for certain conditions. Pain to percussion at any level of the spine can be significant for vertebral osteomyelitis or discitis. Radiating pain along the back, from the back, or to the legs, may be suggestive of disc disease, abscess, or inflammation that irritates the nerves. For patients who have had recent surgical procedures performed, especially along the back, the skin near the incisions should be inspected closely, and if there is drainage, the wounds should be explored to see if they tunnel deeper. This may indicate a deep back wound infection, abscess, or vertebral infection. Pain in the flanks is often suggestive of pyelonephritis or infections along the urologic collecting system. Abdominal exam may be helpful if there is suggestion of pancreatic or gall bladder disease with radiating back pain. Respiratory exams with crackles, evidence of consolidation, or abnormal breath sounds may help isolate pneumonia, abscess, or effusion. Patients with back pain that have difficulty with straight leg raising or bending may have other symptoms or lab values consistent with meningitis or psoas abscess. Similarly pain in the cervical spine is almost always raises concern for meningitis, aseptic or bacterial. Rashes: vesicular, crusted, or papular that have a dermatomal distribution are consistent with Varicella-zoster. Table 4 provides diagnostic clues that can be identified during the physical examination.
Laboratory Findings
Patients presenting with fever and back pain should have diagnostic laboratory studies to help focus the differential diagnosis (Table 5). Two blood culture sets done prior to antibiotic administration should be performed for all patients. Though perhaps more directed toward the thoracic spine and urinary tract complaints, urinalysis and culture may also be helpful as often, urinary pathogens also signify blood stream infections. Erythrocyte sedimentation rate and C - reactive protein are non-specific markers, but if markedly elevated may support a diagnosis of deep-seated infection such as osteomyelitis or endocarditis. Routine complete blood count and comprehensive metabolic panel with liver enzymes should be performed. Elevation of the white blood cell count may be present but does not exclude serious disease if normal. Creatinine abnormalities may support infectious renal pathology or simply call attention the need for antibiotic dose adjustment. Liver enzyme abnormalities may suggest a biliary or hepatic source. If draining wounds are present, a sterile site culture is invaluable for identifying specific pathogens. If osteomyelitis, discitis, or paravertebral abscess are suspected, cultures and biopsies from the site are of utmost importance and will not only help direct initial therapy, but also help tailor therapy for specific pathogens.
Acquisition of tissue in the area of question for pathology, cytology, and tissue culture can not be over emphasized. Pathology samples will often display pathognomonic appearances for specific diagnoses. Often, pathology samples will reveal microorganisms that will aid in the diagnosis, especially if they are not growing on culture. This is especially true of organisms that are sometimes difficult to isolate such as acid-fast organism, moulds and fungi. In addition, pathology helps include or exclude non-infectious conditions (such as in malignancy) that may cloud the diagnosis. As with fluid collection, tissue samples allow for a greater quantity for analysis and will improve the possibility to culturing pathogenic organisms. Tissue or biopsy can be obtained by numerous means. The preferred means is typically surgical tissue collection; however, this is not always practical or feasible. In cases where surgery is required, surgical specimens are optimal, especially if they are obtainable before administration of antibiotics. If a drainable foci or abscess is seen, CT or ultrasound-guided biopsies are safe and rapid methods to obtain tissue samples. CT-guided biopsy is also an acceptable way to obtain bone for pathology and culture in cases of suspected vertebral osteomyelitis or vertebral lesions when surgery is not immediately possible. It also allows for the acquisition of tissue quickly thereby providing tissue prior to antimicrobial administration. Interventional radiology biopsies such as CT or ultrasound-guided procedures should not be a substitute for surgical debridement; however, they should be used as an adjunct to diagnosis, and occasionally therapy.
For patients with a tuberculosis exposure history or risk factors for tuberculosis, a tuberculin skin test should be performed. A negative skin test does not rule out tuberculosis; however, and a positive test may be falsely positive due to reader error, or placement error. A new option in tuberculosis diagnostics is the QuantiFERON-TB Gold (Cellestis, Valencia CA, USA) assay that helps detect latent tuberculosis infection and may possibly play a role in the diagnosis of active disease. This ELISA test detects interferon-gamma in fresh heparinized whole blood from sensitized persons when incubated with mixtures of synthetic peptides simulating two proteins present in Mycobacterium tuberculosis. Because it does not react to proteins commonly encountered in non-tuberculous mycobacteria, it is more specific. Though not necessarily providing a definite diagnosis, it may be helpful in the appropriate clinical setting.
Radiology
All radiologic studies have some limitation because of the possible overlap of potential infectious and non-infectious etiologies in their radiologic appearance. A summary of potential initial radiographic tests is listed in Table 6. Plain radiographs of the site of concern may be helpful but are often limited at detecting acute disease. Most beneficial of all plain radiographs is probably chest radiography especially if it demonstrates pneumonia or lung abscess. Abdominal radiographs may demonstrate calcifications consistent with stones in the collecting system. Radiographs of the spine are generally limited diagnostically for patient with fever and back pain; however, patients with long-standing osteomyelitis who have bony erosion may have positive radiographic findings. Of course, findings like these often will require follow-up with further radiographic testing.
Computed Tomography (CT)
Scanning diagnostically yields more information than any other radiographic test. As it offers a more dimensional view of the body, it is helpful for diagnosing back pain etiologies at any level of the spine. CT scanning is fairly sensitive at detecting osteomyelitis and discitis. It also has reasonable ability to detect paravertebral abscesses and other soft tissue defects. For the purposes of fever and back pain, its biggest strength is probably its ability to pick up other findings that may cause referral to the back such as 1) pulmonary causes: pneumonia, pulmonary embolus, pleural effusion, empyema, 2) biliary tree defects: cholecystitis, pancreatitis, pancreatic phlegmon, liver abscess, 3) renal abnormalities: nephrolithiasis, hydronephrosis, lobar nephronia, 4) other musculoskeletal or gastrointestinal abnormalities: psoas abscess or appendicitis. CT scanning also offers the ability of guided needle biopsy, culture collection, and drainage.
Magnetic Resonance Imaging (MRI)
It has much of the same benefits as CT scanning; however, it is probably more sensitive and specific for vertebral column abnormalities such as osteomyelitis or discitis. MRCP however, may also help with biliary tree imaging. Because of the high sensitivity and specificity and ability to differentiate between infected bone and adjacent tissue, MRI can be utilized as the sole test in evaluation of osteomyelitis. Its benefit is greatest in patients who have no acute fractures or existing metallic hardware that can leave artifact. In the setting of fever and back pain, MRI is probably the best test to use to identify potential bone lesions that may have resulted from infectious or non-infectious sources.
Nuclear Scanning
It is probably more limited in the setting of fever and back pain; however, they can be helpful, especially in cases where an identifiable focus is elusive. Scans that are often employed include three phase bone scans or the Technetium-99m scan, Gallium-67 scan, and Indium-111 scan. These scans tend to be very non-specific and as such should be interpreted with caution. Sensitivity and pre-test probability varies widely depending on the circumstances. Bone scans tend to be helpful to localize specific bony abnormalities. They are very sensitive for detection of osteomyelitis, but they are not very specific; there are many false positives because of the tests ability to detect non-infectious and infectious bony abnormality. They are useful at detecting bony metastasis. Gallium scans are fairly sensitive at detecting spinal abnormalities in the setting where MRI is not possible. Like other nuclear scans, the findings are not specific, and gallium should not be used alone to diagnose osteomyelitis. Indium white blood cell scanning is helpful for localizing areas where leukocytes migrate or for detecting areas of inflammation. They are fairly sensitive, but because tissue cannot be differentiated by Indium scan, the definition is limited. Indium scan’s asset probably lies in the ability to find potential foci of infection that were previously undetectable. Results do need to be interpreted with caution, however, as specific tissues or systems can not always be deduced. Of note, nuclear scans should be selected with caution as the half-life of the isotopes may prohibit further nuclear scans for days to weeks. As with all radiographic tests, interpretation accuracy is operator dependent, and the usefulness of these tests varies widely from person to person.
Ultrasound
may have some benefit for imaging of the abdominal aorta, the kidneys, and the biliary tree. Ultrasound often times offers the ability of guided biopsy or fluid aspiration as well. It is generally rapid and non-invasive, but its sensitivity is limited except in specific diagnostic situations such as diagnosing aortic aneurysms and evaluating the renal pelvis and biliary tree.
EMPIRIC ANTIMICROBIAL THERAPY
For patients who are not acutely ill, antibiotic therapy should be held until sufficient diagnostic tests have been performed to contribute to the microbiologic diagnosis including cultures and tissue samples. These samples should be obtained with rapidity so as not to delay early treatment. Once the suspected site of infection is ascertained, empiric antimicrobial therapy can be initiated. Initial empiric therapy should only be continued until a specific pathogen is isolated at which time targeted therapy should be employed to complete the treatment course. With fever and back pain, most empiric therapy is started intravenously as potential infections are usually serious. Some infections may be managed with oral antibiotics and outpatient therapy if patients are stable. Empiric therapy should be started according to the suspected systems involved (Table 7).
Patients with surgical wound infections along the vertebral column should be covered for skin flora as well as possible hospital acquired pathogens, including resistant gram-positive organisms. Common pathogens seen in this setting areStaphylococcus aureus, Streptococcus sp. (including Enterococcus sp.) and coagulase-negative Staphylococci. Occasionally, hospital-associated gram-negative bacilli are isolated. A reasonable choice for gram-positive cocci and resistant gram-positive cocci coverage is vancomycin 15mg/kg q12h for normal renal function. Cefepime 2g q12h, piperacillin-tazobactam 3.375g q6h, or ciprofloxacin 400mg q12h are options for gram-negative bacilli coverage. Cefepime and piperacillin-tazobactam have an advantage of further gram positive coverage and piperacillin-tazobactam also adds anaerobic coverage if it is suspected. For patients with beta-lactam allergy, aztreonam 2g q8h is a reasonable choice. Linezolid 600mg q12h,daptomycin 4mg/kg q24h soft tissue, 6mg/kg q 24h for osteomyelitis, and tigecycline 100mg once followed by 50mg q12h are also reasonable choices for infections caused by resistant gram-positive cocci. Tigecycline has the added benefit of gram-negative, resistant gram-negative, and anaerobic coverage. There are few studies to suggest that spine infection and epidural abscess can be managed non-operatively. Most infectious disease authorities would not endorse this approach. Evidence supports surgical debridement and appropriate courses of target-directed antimicrobial therapy. Non-operative approaches will more frequently lead to recurrence of infection or treatment failure. Occasionally epidural abscesses can be drained with the help of interventional radiology, and some sources suggest this to be an acceptable adjunct to antibiotic therapy. Surgical debridement, however, should not be withheld, if there is suspicion of osteomyelitis, or if a focus does not look to be draining adequately.
For patients with suspected intraabdominal infections, pathogens covered should include enteric flora including gram-negative bacilli, anaerobes, and gram-positive cocci. If bowel perforation is suspected with significant fecal contamination, yeast should also be considered as a pathogen. Reasonable choices include vancomycin and piperacillin-tazobactam. Clindamycin 900mg q8h and metronidazole 500mg q8h are alternatives for anaerobic coverage in the penicillin allergic patient. Fluconazole 200-400mg daily is reasonable for initial yeast coverage. If vancomycin-resistant enterococcus is suspected, linezolid should take the place of vancomycin.
Patients with genitourinary infections should be covered primarily for gram-negative bacilli. However, patients who have had instrumentation in their urogenital tracts, or have had catheterization, recurrent hospitalization, or polymicrobial urinary tract infections may have gram-positive cocci infections as well. Reasonable first choices include piperacillin-tazobactam, ciprofloxacin, aztreonam, or cefepime. Coverage for resistant organisms should be considered in patients with a known history of infection with resistant pathogens.
For patients with a suspected pulmonary infection, treatment should consider risk factors and the setting of the infection. For cases of community acquired pneumonia, treatment should follow guidelines set by the American Thoracic Society and Infectious Disease Society of America. Nosocomial infections should include coverage for gram-negative bacilli and resistant pathogens, and often addition of linezolid or vancomycin for resistant gram-positive cocci may be necessary. Coverage of resistant gram-negatives may require use of imipenem-cilastatin 500mg q6h or meropenem 1g q8h. As always, once pathogens are isolated, antibiotic choices should be narrowed for directed therapy. In cases where there is a pulmonary abscess or empyema, culture and drainage of the fluid is of utmost importance. For patients with pulmonary disease consistent with septic emboli, treatment should be directed at the suspected blood-borne pathogen. These are usually but not always gram-positive cocci.
Non-Antibiotic Management
As a general rule in infectious diseases, a patient with a drainable focus of infection must have that focus removed for antimicrobial therapy to be effective. For patients with fever and back pain, there are several potential areas where non-antimicrobial management would be beneficial. Whenever possible, abscesses should be drained, and necrotic tissue should be debrided. For deep tissue infections, especially osteomyelitis and discitis, surgical intervention is the most important step toward achieving microbiologic cure. Non-antibiotic therapy such as pain control and sometimes steroids should be considered on a case-by-case basis for infectious and non-infectious causes of back pain. In particular, steroids for patients with back pain due to metastatic disease will often help for symptomatic relief of pain due to bony destruction, and occasionally neurologic pain that originates from nerve impingement. Antipyretics are essential for maintaining patient comfort; however, they should be used only when needed and not necessarily as a response to an elevated temperature. In many cases, patients who have fever are asymptomatic, and an altered fever curve as a result of anti-pyretics or steroids may mask infection declaration.
ENDPOINTS FOR MONITORING THERAPY
Most infections without a deep focus and without osteomyelitis or discitis require 14 days of antibiotics therapy in addition to removal of the focus of infection. For instance, in a case of a soft tissue abscess, fourteen days of appropriate antibiotic given after drainage of an abscess should be sufficient. For cases where there may be residual infection or where antibiotic tissue penetration is uncertain, longer courses may be needed. As a general rule, osteomyelitis and discitis require at least six weeks of antibiotic therapy after incision and drainage. Most outcomes are measured on the basis of clinical success. Occasionally repeat radiographic studies especially for vertebral osteomyelitis and discitis may be helpful in guiding therapy duration and to ensure resolution of inflammation. For cases of spinal osteomyelitis, follow-up imaging can be a useful modality for evaluating improvement. Follow-up imaging should be performed near the close of a course of antibiotic therapy. Patients who have had operative management and a course of antibiotics should have improvement in radiographic appearance. There may still be some residual inflammation, and further treatment will be a clinical decision. Patients who have worsening in appearance will likely require further surgical debridement and longer courses of antibiotics. In patients who have not had operative management in addition to an antibiotic course, cure rates are generally lower. If there has been improvement, longer courses of antibiotics should be considered; however, if there has been worsening, surgical debridement should be performed before any further antimicrobial therapy is administered. In any case where surgical intervention is required, further cultures and samples should be obtained to ensure adequate coverage of pathogenic organisms.
COMPLICATIONS AND MANAGEMENT
Patients with fever and back pain have the potential for complicated courses if not handled appropriately the first time. Persistent infection of the vertebral column can lead to erosion of the vertebral bodies, vertebral collapse, neurologic damage or chronic pain, and potentially paralysis. Undrained abscesses of the abdomen may lead to extension of the abscess and occasionally bacteremia. Biliary tree infections may also progress to overwhelming sepsis. Psoas abscesses may also form as a result of contiguous structure involvement. Complications such as these should be managed on a case-by-case basis and appropriate management should be used to curtail further worsening and hopefully lead to improvement.
CONCLUSION
Fever and back pain can be a diagnostic challenge. The keys to successful diagnosis and treatment include thorough history and physical examination and use of red flags and key history components to narrow the differential. Often premature antimicrobial therapy can reduce the window of microbiologic diagnosis if adequate diagnostic specimens have not been obtained prior to therapy. Whenever possible, antibiotics should be withheld from the non-acutely ill patient until these specimens can be obtained. This should be done with rapidity so as not to delay early treatment. For patients who are acutely ill, empiric therapy should be initiated, but appropriate diagnostic studies should also be carried out in a timely fashion. Radiographic tests are helpful for localizing disease or confirming a diagnosis. Once a microbiologic diagnosis has been made, antimicrobial therapy should be narrowed to target specific pathogens.
READING LIST
1. Calhoun JH, Manring MM. Adult osteomyelitis. Infect Dis Clin N Am. 2005;19:756-786. [PubMed]
2. Darouiche RO. Spinal Epidural Abscess. N Engl J Med. 2006;355:2012-20. [PubMed]
3. Lazzarini L, Lipsky BA, Mader JT. Antibiotic treatment of osteomyelitis. Int J Inf Dis. 2005;9(3):127-138. [PubMed]
4. Mazurek GH, Jereb J, LoBue P, Iademarco MF, Metchock B, Vernon A. Guidelines for using the QuantiFERON-TB Gold Test for Detecting Mycobacterium tuberculosis Infection, United States. MMWR 2005;54(RR15):49-55. [PubMed]
5. Baron MJ, Madoff LC. Pancreatic Infections. Principles and Practice of Infectious Diseases, 6ed. Mandell GL, Bennett JE, Dolin R. 2005; 959-966.
Tables
Table 1: Differential Diagnosis of Common Problems Presenting with Fever and Back Pain
Specific Level |
Infectious |
Non-Infectious (coincidental or associated fever) |
|---|---|---|
Cervical
|
Musculoskeletal - Discitis - Paraspinal abscess - Epidural abscess - Cellulitis/Abscess/Ulcer Neurologic |
Musculoskeletal - Osteoarthritis - Osteoporosis - Spinal stenosis - Disc herniation - Compression fractures - Myopathy/Muscle spasm Metabolic - Rhabdomyolysis Malignancy/Metastatic Disease |
Thoracic |
Musculoskeletal - Discitis - Osteomyelitis - Paraspinal abscess - Epidural abscess - Spinal tuberculosis Renal - Renal abscess, Nephronia GI - Cholangitis - Perforated ulcer/Peritonitis - Hepatic abscess - Hepatitis Pulmonary - Lung abscess Skin - Cellulitis/Abscess/Ulcer Neurologic - Meningitis |
Musculoskeletal - Osteoarthritis - Osteoporosis - Spinal stenosis - Disc herniation - Compression fractures - Myopathy/Muscle spasm Metabolic - Rhabdomyolysis Renal - Nephrolithiasis GI - Cholecystitis - Cholelithiasis/choledocholithiasis - Pancreatic cysts Vascular - Aortic aneurysm Malignancy/Metastatic disease |
Lumbar/Sacral |
Musculoskeletal - Discitis - Paraspinal abscess - Epidural abscess - Spinal tuberculosis GU GI - Diverticulitis - Appendicitis Skin - Cellulitis/Abscess ulcer Neurologic - Meningitis |
Musculoskeletal - Osteoarthritis - Osteoporosis - Spinal stenosis - Disc herniation - Compression fractures - Sacroileitis - Myopathy/Muscle spasm - Ankylosing spondylitis Metabolic - Rhabdomyolysis Vascular - Mesenteric insufficiency Malignancy/Metastatic disease
|
Dermatologic |
Nerve Root impingement Malignancy/Metastatic disease |
Table 2: Common Causes of Musculoskeletal Back Pain
Myopathy/Muscle Spasm Osteoarthritis Osteoporosis Spinal stenosis Disc herniation Compression fractures Myopathy, muscle spasm Metastatic Disease: Breast Lung Gastrointestinal Prostate Lymphoma Melanoma Unknown Renal Other |
Table 3: Causes for Concern in Patients with Fever and Back Pain and Questions to Ask
Causes for concern |
Potential Questions |
|---|---|
Clinical History - Recent prior bacteremia - Chronic intravenous catheters - Vertebral osteomyelitis history - Prosthetic valves with recent dental procedures - Cancer - Recent back surgery |
Any recent treatment for - a blood stream infection? - a heart valve infection? - bone infection in your spine? Have you had or do you have any long term IV lines? Have you had any recent surgical or dental procedures? Do you have any new hardware in your body such as heart valves or joints? Have you had any back surgery? Do you have any cancer history? When was your last - breast exam? - colonoscopy? - Pap/pelvic? |
Social History - Intravenous drug use - Recent hospitalization |
Do you use or have you used any recreational drugs such as cocaine, marijuana, or any IV drugs? Have you been recently hospitalized? |
Lab Findings - Elevated C-reactive Protein - Elevated erythrocyte sedimentation rate >100 - Positive aspirate culture from vertebral source |
|
Radiographic Findings - Vertebral radiolucencies on CT scan - Paraspinal or epidural abscesses - Positive bone scans or radionucleide scans with vertebral localization - MRI findings suggestive of osteomyelitis |
|
Table 4: Potential Infectious Diagnoses for Specific Findings in a Patient with Fever and Back Pain
Finding |
Potential Diagnosis |
|---|---|
Nuchal rigidity Kernig sign Brudzinski sign |
Meningeal irritation, meningitis |
Costovertebral angle (CVA) tenderness |
Pyelonephritis, renal abscess
|
Pain to blunt percussion on the spine |
Abscess, osteomyelitis, discitis |
Pain to blunt percussion on the posterior thorax |
Pneumonia, lung abscess |
Oslers nodes Janeway lesions Cardiac murmurs Nail bed splinter hemorrhages Roth spots Conjunctival hemorrhages |
Endocarditis with the potential for seeding of the vertebral column or abscess |
Dermatomal vesicular or evolving rash |
|
Vertebral pain with flexion, extension of the spinal column |
Musculoskeletal abnormalities, infectious or non-infectious |
Radiating limb numbness or weakness |
Spinal cord irritation, nerve root impingement from discitis,vertebral osteomyelitis, compression fractures |
Pain with bending or straight leg raising |
Meningitis, psoas abscess |
Pulsatile abdominal mass |
Abdominal aortic aneurysm |
Abdominal Tenderness, right upper quadrant, epigastric |
Abdominal pathology, peritonitis, cholecystitis, cholangitis,pancreatic, pancreatic phlegmon |
Abnormal lung exam findings, such as crackles, areas of consolidation, dullness to percussion, diminished breath sounds |
Pneumonia, pleural effusion, lung abscess |
Table 5: Suggested Initial Laboratory Work-up in a Patient with Fever and Back Pain
Two sets of blood cultures Erythrocyte sedimentation rate or C-reactive protein Urinalysis and urine culture Sputum culture and sensitivity Site cultures if abscess or osteomyelitis Complete blood count with differential Complete metabolic panel Pathology or biopsy and culture of suspected infectious sites |
Table 6: Suggested Initial Radiologic Work-up Based on Suspected Source
Thorax, pulmonary |
Two view Chest radiography CT scan of the thorax |
Abdominal |
Abdominal ultrasound Renal ultrasound Plain abdominal series CT scan with contrast |
Vertebral column |
Plain radiograph MRI |
Uncertain Source |
CT scan, thorax, abdomen, pelvis Bone Scan Indium Scan |
Table 7: Suggested Empiric Therapy Fever and Back Pain of Selected Sources
**For patients who are not acutely ill, antibiotic therapy should be held until sufficient diagnostic tests, including cultures and tissue sample, may be obtained that might help contribute to the microbiologic diagnosis. Dosages listed are for normal renal function.
Location/Situation |
Antibiotic therapy |
Non-antibiotic therapy |
|---|---|---|
Surgical wound infections along the vertebral column, suspected osteomyelitis. |
Vancomycin 15mg/kg q12h
Other resistant Gram-positive cocci coverage Linezolid 600mg q12h Daptomycin 4mg/kg-6mg/kg q24h Tigecycline 100mg once then 50mg q12h
For gram negatives bacilli add, cefepime 2g q12h or piperacillin-tazobactam 3.375g q6h or ciprofloxacin 400mg q12h or aztreonam 2q q8h (PCN allergic)
|
Surgical debridement Wound care Analgesics Anti-pyretics
|
Vancomycin 15mg/kg q12h and Piperacillin-tazobactam 3.375g q6h
Imipenem-cilastatin 500mg q6h or meropenem1g q8h may be substituted for piperacillin-tazobactam
Other gram-negative bacilli coverage, requires further anaerobic coverage Cefepime 2g q8-12h or Ciprofloxacin 400mg q12h
PCN allergic anaerobic coverage: Clindamycin 900mg q8h or metronidazole 500mg q8h
For yeast coverage Fluconazole 200-400mg q24h
If VRE suspected Linezolid 600mg q12h in place of vancomycin |
Surgical debridement Radiology guided drainage Analgesics Anti-pyretics |
|
Genitourinary infections |
Piperacillin-tazobactam 3.375g IV 6h or Ciprofloxacin 400mg q12h or Aztreonam 2g q8h or Cefepime 2g q 12h
For gram positive cocci Vancomycin or linezolid if suspected |
Surgical debridement Remove hardware, stents, catheters Analgesics Anti-pyretics |
Pulmonary infections |
-refer to IDSA-ATS guidelines
Nosocomial pneumonia, consider resistant Gram Positive cocci, Gram Negative bacilli, and mouth anaerobes
Resistant Gram-Positive cocci: linezolid 600mg q 12h or vancomycin 15mg/kg q12h
Resistant Gram-Negatives bacilli: Imipenem-cilastatin 500mg q6h or meropenem 1g q8h
Anaerobes: Imipenem-cilastatin or meropenem or metronidazole 500mg q8h or clindamycin 900mg q8h
|
Chest tube drainage of empyema or persistent pleural effusion Analgesics, anti-tussives, anti-pyretics, expectorants Thoracotomy |