
Aerococcus urinae
Authors: Jens Jørgen Christensen, M.D., DMSc, Xiaohui Chen Nielsen, M.D., PhD
Previous Authors: Jens Jørgen Christensen, M.D., DMSc, Robert Skov, M.D.
Microbiology
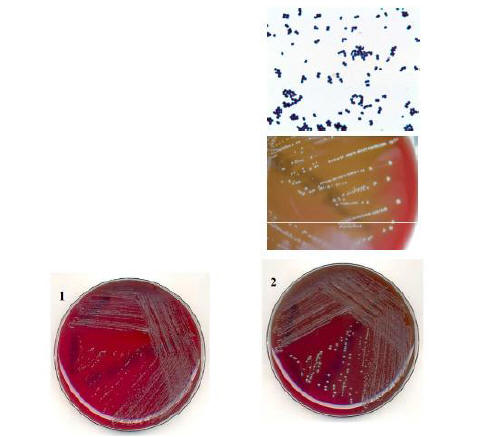
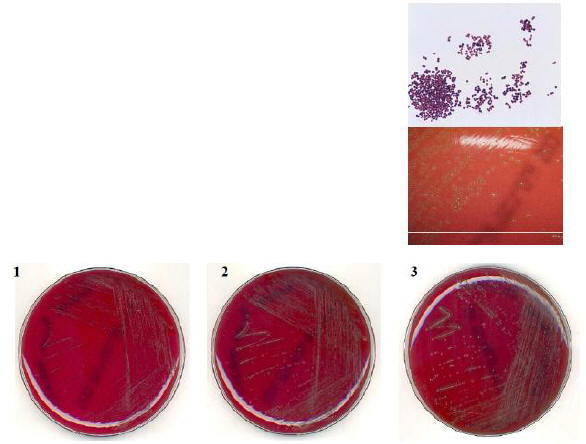
Aerococcus urinae and Aerococcus sanguinicola are newcomers to clinical and microbiological practice. The first report on A. urinae was published in 1989 (14) and the name designated in 1992 (1) and A.sanguinicola was named in 2001 (40). Isolates from both species were originally recognized by the cell-morphology (Staphylococcus-like in Gram stain, Figures 1, 2, 3), growth characteristics (resembling alpha haemolytic streptococci on blood agar), a negative catalase reaction, a consistent antibiogram demonstrating susceptibility to β-lactams and, for A. urinae resistance to sulfonamides and aminoglycosides. An external quality control in Norway revealed that A. urinae in urine specimen was correctly identified in only six of 24 laboratories (28, 52). Presumably, the diagnosis of infections caused by both organisms is still missed in many laboratories around the world (5, 43, 49).
{kind=link}
{kind=link}
{kind=link}
The Aerococcus genus now includes eight species of which Aerococcus viridans (1953) was the one originally described and for a long time the only species in the genus (23). In the last one to two decades additionally six species have been included in the genus: A. urinae (1992), Aerococcus christensenii (1999), Aerococcus urinae hominis (2001), A. sanguinicola (2001), Aerococcus urinaeequi (reclassification of Pediococcus urinae equi, 2005), Aerococcus suis (2007), and Aerococcus vaginalis (2014). All species, except A. suis (from pigs), A. urinae equi (from horses) and A. vaginalis (from beef cow), have been found as pathogens in human clinical situations such as urogenital infections, bacteremia/septicaemia and infective endocarditis. They may also appear as contaminants in clinical cultures. A. viridans occurs in many different habitats such as soil and air. It is a rare cause of infections in humans, but cases of urinary tract infection (UTI), bacteraemia, endocarditis and meningitis have been reported (51). A. urinaeand A. sanguinicola are described as pathogens in UTI in patients predisposed to infection (13, 14, 15, 24, 28, 34, 54, 68) and are also agents of bacteremia/septicaemia as well as infective endocarditis (5, 10,20, 21, 24, 34, 37, 61, 67). A. christensenii has been isolated from vaginal specimens (51), but little is known about the clinical relevance. Molecular analysis of the diversity of vaginal microbiota has strongly associated Aerococcus, as one of eight genera, with bacterial vaginosis (42). A. urinae hominis has been isolated from urine in a few cases (23).
Epidemiology
A. urinae is mainly associated with (UTI) especially in elderly patients with predisposing conditions (15, 28, 54, 49, 68). Studies from Europe have found a prevalence of A. urinae strains of 0.3-0.8% of urine specimens examined (14, 28, 54) and most recently Lupo et al. (43) and Guilarte et al. (29) observed a prevalence of 4%. Thus, A. urinae ranked sixth as a UTI pathogen. A. urinae strains causing urinary tract infections have been recognized worldwide (12, 13, 14, 15, 24, 28, 34, 49, 51, 54, 68). Throughout the world, A. urinae has also been isolated from blood from patients suffering from urogenic bacteraemia/septicemia, often complicated with endocarditis (4, 9, 10, 18, 20, 21, 26, 30, 31, 37, 39, 48, 49, 55, 58, 63, 65, 66, 67). A nationwide survey in Denmark has identified A. urinae in blood from more than 50 patients. It seems that the bacteremia may be complicated with endocarditis in approximately one third of cases. A review of the first 17 Danish patients has been reported (10). Recently all published endocarditis cases have been reviewed (21, 37, 56) and new case reports from over the globe are being reported. In addition single cases of soft tissue infections (phlegmon and balanitis), (55), spondylodiscitis (3), hip abscess (25), lymphadenitis (53), acute pyelonephritis (18), and peritonitis in connection to peritoneal dialysis (35, 46) have been reported. A. urinae may be a possible reason for malodorous urine (41).
A. sanguinicola, with respect to association to UTI, has a very similar epidemiology as seen for A. urinae, though less frequent identified (5, 24). Among 30 aerococci identified among 350 consecutively collected non-enterococcal Streptococcus-like strains in the period from March 2006 to November 2008, 20, 8 and 2 strains were by molecular methods identified as A. urinae, A. sanguinicola and A. viridans, respectively (5). A PubMed search revealed ten cases with positive blood cultures of A. sanguinicola (24, 34, 40). Four cases of septicemia, in whom a urological focus was present in two as was complicating infective endocarditis. In the remaining six bacteremia cases, one had a clinical suspicion of gall-bladder infection, one had UTI and one had pneumonia. In three cases the clinical diagnosis was unknown.
Clinical Manifestations
Urinary Tract Infection
A. urinae and A. sanguinicola most often causes UTI in elderly patients with a median age around 75 years and with a tendency to female predominance (5, 15, 28, 49, 54, 68). Acute pyelonephritis in a 12-year-old-boy has also been reported (45). Symptoms are the usual of urinary tract infections (dysuria, pyuria, and/or fever). Underlying conditions predisposing to infection either systemic or of urogenital/anatomical origin were common, irrespectively of whether A. urinae or A. sanguinicola was present singly or in admixture with other known uropathogens. The reported frequency of concomitant growth varies from 40 to 60%. Paraclinically, counts of >105 A. urinae or A. sanguinicola per ml urine and a positive leucocyte-esterase test has been found.
Septicemia and Endocarditis
A. urinae bacteremia is most often seen in the elderly. Nearly all of the patients have had a focus in the urinary tract and in approximately one third of the patients the septicemia was complicated by aortic- or mitral valve endocarditis (2, 4, 9, 10, 18, 20, 26, 30, 31, 37, 39, 48, 55, 56, 58, 63, 65, 66, 67). More than 50% of the patients had predisposing factors either underlying diseases i.e. cancer and diabetes mellitus or hyperplasia of the prostate and/or indwelling catheters (9, 56); this is probably a major reason for the very poor outcome seen in patients, where the bacteremia is complicated by endocarditis. In the review by Ebnöther et al (21) comprising 11 cases, only four survived.
Molecular examination (16S rRNA gene sequencing and subsequent BLAST examination) of aortic valve tissue has been successfully used for definitive diagnosis (21, 38, 44, 64).
A. urinae was grown from blood in admixture to Staphylococcus aureus, Actinobaculum schaalii,,and E. coli (9, 50, 65, 66). The sparse number of A. sanguinicola blood-culture positive cases does not allow for general descriptions of clinical manifestations (24, 34, 40).
![]()
Laboratory Diagnosis
A. urinae and A. sanguinicola resembles β-hemolytic streptococci by growth, and unless microscopy is performed (showing cocci in tetraeds or clusters), they can easily be misidentified. Incubation in CO2 is often required. The main task in the laboratory is in separating both species from staphylococci, β-hemolytic streptococci, enterococci and other gram-positive cocci. Staphylococcus aureus is easily separated from A. urinae because of catalase positivity and lack of β-hemolysis. Alpha-hemolytic streptococci and enterococci can be differentiated by microscopy by their chain formation.
Separating A. urinae and A. sanguinicola strains from other gram-positive, catalase-negative non-chain-forming cocci includes differentiation from other aerococci and related genera (Table 1). The non-Aerococcus genera, can be separated from the aerococci by inborn resistance to vancomycin (Pediococcus sp.), inability to grow in broth supplemented with 6.5% NaCl (Gemella sp.), weak catalase activity (Alloioicoccus) or being assaccharolytic (Dolosigranulum and Helcococcus), as only A. christensenii has been found asaccharolytic among the aerococci. A. urinae and A. christensenii shares the combination of being pyrrolidonyl aminopeptidase negative and leucine aminopeptidase positive. A. viridans exhibits the opposite pattern for these two reactions. A. sanguinicola is positive and A. urinae hominis negative for both these tests (Table 1). Among aerococci, esculin hydrolysis activity is present, except in strains of A. christensenii and A. urinae, though some strains of the latter have been found positive (11). Acid production from sucrose, trehalose, mannitol, maltose and lactose adds to separation of Aerococcus species. Commercial identification systems are highly dependent of the database used. A. viridans reaction patterns are included in the relevant databases, A. urinae patterns in some (API 20 STREP, ID 32 STREP, VITEK2 ID-GPC, Crystal-GP), whereas the remaining Aerococcus species patterns are not presently in the databases (5, 24). In best case non-A. viridans aerococci gives a correct A. urinae identification or an unacceptable profile. However, misidentifications are very common when examining non-A. viridans aerococci (5, 24). Additionally, the databases do not include the more recently described catalase negative, non-chain-forming Gram-positive cocci as well as new developments within established genera, for instance Gemella species.
Based on phenotypic characteristics two major patterns of A. urinae have been found. The majority of strains characteristically are aesculin-hydrolysis negative and β-glucuronidase negative, not producing acid from salicin and amygdalin, β-glucosidase positive, and producing acid from methyl-D-glucopyranoside. The second major group of strains exhibits opposite reactions in those tests (11, 16).
Strains of A. urinae are very homogeneous when performing 16S rDNA sequence analysis and DNA-DNA relatedness investigations (16). When using 16S rRNA gene sequence analysis as well A. urinae asA. sanguinicola shows close to 100% sequence identity to best taxon match and major differences in MaxScore between first and second best taxon matches ensuring convincing species identifications (8, 16,34). When examining A. urinae strains second best taxon match is A. sanguinicola and vice versa. A 1200 bp fragment of the ribosomal RNA gene was also used convincingly by Cattoir et al. (5), when examining as well A. urinae as A. sanguinicola strains. The approach of having a single molecular platform for strains resembling non-hemolytic streptococci based on 16S-23S Intergenic Spacer (ITS) Region sequence analysis has been examined by Nielsen et al. (47). ITS sequences of 29 type strains and 103 well-characterized clinical strains, within the genera Aerococcus, Abiotrophia, Alloiococcus, Dolosicoccus, Dolosigranulum, Facklamia, Granulicatella, Gemella, Ignavigranum, Leuconostoc, and Vagococcus were determined and BLAST analysis performed for species identification. All clinical strains, including 27 and 5 strains of A. urinae and A. sanguinicola, respectively, were convincingly identified to the species level. MALDI-TOF mass-spectrometry seems very promising with respect to identification of aerococci. Among available identification systems the MALDI Biotyper (Bruker Daltonics, Billerica, MA) and the VITEK MS (bioMérieux) are those by far most extensively used in daily routine. The Vitek database for routine use does not include information on A. urinae and A. sanguinicola. Employing the MALDI Biotyper (Bruker Daltonics, Billerica, MA (using MALDI Biotyper automation control 2.0.43.1 software) 51 culture collection strains and 90 well-characterized strains, including aerococci and related genera, have been examined showing excellent identification of aerococci and related genera (7). The following genera were represented: Aerococcus (n = 42), Gemella (n =30), Granulicatella (n = 11), Abiotrophia (n = 3), Lactococcus (n = 9), Globicatella (n = 7), Leuconostoc (n = 9), Rothia(n = 9), Facklamia (n = 7), Vagococcus (n = 2), Helcococcus (n = 4), Alloiococcus (n = 2), Pediococcus (n = 3), Ignavigranum (n = 1), Dolosicoccus (n = 1), and Dolosigranulum (n =1). The obtained mean score values illustrated diversity within the different species and also an effect on mean score values of different conditions for creating MSPs. The MSP dendrograms for Aerococcus, Gemella,Granulicatella, and Abiotrophia convincingly delineated the included species. Thus, for routine use, MALDI-TOF MS was shown to be robust. Likewise using the MALDI Biotyper version 2.0 (and an extension of the database) in a sensitivity and specificity study 41 and 44 aeroccal strains, approximately half of each being A. urinae and A. sanguinicola strains (as determined by 16S rRNA gene sequencing) were both convincingly identified to the species level and that the method has excellent sensitivity in this respect. (56). Also, using Bruker Biotyper and When employing direct transfer of material to the target plate and addition of formic acid, Schulthess et al. had 100% agreement in identification of 17 strains of Aerococcus (not species specified) out of totally 156 gram positive cocci when compared with results of conventional methods and 16S rRNA gene analysis Thus, MALDI ToF MS is a very powerful tool with respect to identification of also these two bacterial species.
![]()
Pathogenesis
The reservoir for A. urinae and A. sanguinicola is presently unknown. The gastrointestinal tract is a good candidate as a reservoir as for other urinary tract pathogens, though this has not been studied. Urinary tract infection is almost always the focus for an evolving bacteremia. A. urinae exhibits virulence strategies of importance for infective endocarditis (59). Five A. urinae strains isolated from human blood were shown to form biofilms in vitro, and biofilm formation was enhanced by the presence of human plasma. Four of the A. urinae isolates caused platelet aggregation in platelet-rich plasma from healthy donors. Plasma proteins at the bacterial surface were needed for platelet aggregation; and roles of the complement system, fibrinogen, and immunoglobulin G were demonstrated.
SUSCEPTIBILITY IN VITRO AND IN VIVO
Single Drug
Data on in vitro susceptibility of A. urinae are accumulating. Publications including data on more than 10 isolates and reporting MICs are accumulating (5, 9, 13, 27, 29, 32, 33, 36, 43, 54, 56, 62). The number of susceptibility reports on A. sanguinicola are sparse (5, 6, 24, 34). MIC results on the two species are given in Table 2. Table 3CLSIEUCAST. The lack of standardized susceptibility test methods and interpretive criteria for Aerococcus spp. are problematic for clinical laboratories and clinicians (32). A variety of test methods have been reported, and interpretive criteria for streptococci, staphylococci, and even enterococci have been applied (32). Most publications compare results to interpretive criteria for viridans group streptococci. Interpretive criteria are being evaluated by CLSI and EUCAST at present (personal communication).
Table 2 shows that A. urinae isolates exhibit an antimicrobial susceptibility pattern rather similar to that of β-haemolytic streptococci with susceptibility to penicillins and vancomycin and low level resistance towards aminoglycosides. Only minor inter-strain susceptibility variation was found, which is in accordance with the published disk/tablet diffusion data (15, 27, 36, 52, 54, 68). Most strains have low MICs to also other beta-lactams than penicillin. However for cefotaxime and ceftriaxone modal MICs has been found significantly higher than the modal MICs for penicillin and amoxicillin (32, 63).
A. urinae is further susceptible to clindamycin, teicoplanin, chloramphenicol, nitrofurantoin, and mupirocin and resistant to sulfonamides, colistin, mecillinam, and fosfomycin. A. urinae and A. sanguinicolaseems intrinsically susceptible to fluoroquinolones (6), but in the recent report by Cattoir et al. they found eight of 20 and seven of eight strains, respectively, being resistant to ciprofloxacin (6). Moxifloxacin was 4-16 times more active than ciprofloxacin/levofloxacin. As A. urinae primarily has been associated with urinary tract infections, it should be noted that A. urinae is resistant to several of the antibiotics used empirically for urinary tract infections, i.e. nalidixic acid, trimethoprim, sulfonamides, fosfomycin, and mecillinam. Cattoir et al. 2010 describes a contrast between A. sanguinicola and A. urinae with respect to co-trimoxazole and fosfomycin susceptibility being opposite for the two species (Table 2). SXT resistance has been a key feature of the identification of A. urinae;however, as stressed by Humphries et al. (33) there is a marked medium effect when considering SXT test results for this organism, as they found universal susceptibility among 107 isolates tested in CAMHB-LHB (see Table 2, comment c). CAMHB-LHB is the medium recommended by CLSI for antimicrobial susceptibility testing of Streptococcus species. As SXT is a drug of choice for the treatment of uncomplicated cystitis, clinical studies that investigate the efficacy of this drug for the treatment of UTIs caused by A. urinae are required to determine its clinical value. Otherwise, the antibiograms for the two species resembles each other, though for A. sanguinicola, the number of strains and antibiotics examined is less than for A. urinae. Shelton-Dodge et al (60) examined 30 strains of A. urinae and 41 strains of A. sanguinicolawith MIC determinations. Calculation of MIC50/MIC90 is not presented. Data on penicillin, ceftriaxone and vancomycin resembles the data presented in Table 2. Elevated erythromycin MICs were noted in 41% of A. sanguinicola and 17% of A. urinae isolates and elevated levofloxacin MICs were noted in 78% of A. sanguinicola and 33% of A. urinae isolates.
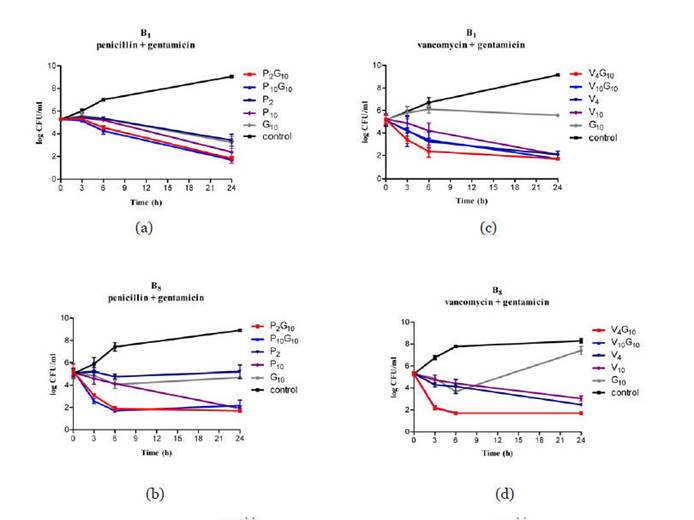
For A. urinae, time-kill studies have been reported for penicillin, gentamicin, netilmicin and vancomycin for only four strains (62, 67). None of the tested antibiotics individually exhibited constant bactericidal activity against the tested isolates.
No animal studies have been published on efficacy of antibiotic treatment.
Combination Drugs
Rapid and bactericidal effect of A. urinae has been reported both for the combination of penicillin and aminoglycosides as well as vancomycin and aminoglycosides (62, see Figure 4). However, only data on four strains have been published (62, 67).
{kind=link}
![]()
ANTIMICROBIAL THERAPY
Drug of Choice
Penicillins using standard doses have proven effective and are the drugs of choice for urinary tract infections.
Special Infections
Data on treatment outcome of serious infections caused by A. urinae are accumulating. More than 50 cases have been identified in Denmark and cases have been reported increasingly worldwide (4, 9, 10, 18,20, 26, 30, 31, 37, 39, 48, 55, 58, 63, 65, 66, 67). The outcome of the first 17 cases has been published (10). Most proven is penicillin or ampicillin in combination with gentamicin, whereas evidence for using cephalosporins in severe cases is lacking. In the review by Ebnöther et al 2002, 11 cases of infective endocarditis were discussed (21). Data on treatment outcome of serious infections caused by A.sanguinicola is even more limited; according to a Medline search 10 cases of bacteremia have been published. Data below, therefore, is mostly related to treating A. urinae infections, but the great resemblance of data on bacteriology and disease spectrum indicates that A. sanguinicola infections should be treated analogical.
Bacteremia/Septicemia
Intravenous penicillin G 2 million IU (1200 mg) t.i.d. with or without aminoglycosides have been effective (10, 21, 37).
Endocarditis
Cases of bacteremia complicated with endocarditis have had a poor outcome with fatal outcome in seven out of 12 patients (10, 21, 26, 37, 67). Most of these patients were elderly with severe underlying diseases.
The literature does not support firm recommendations of either dosage or length of treatment. Based on the reported clinical cases, our own unpublished observations, and the in vitro time kill results, patients with endocarditis on native valves should be treated with intravenous penicillin for at least four weeks in combination with an aminoglycoside for at least the first 14 days with monitoring of clinical and laboratory results. Due to the high mortality extending the combination therapy to six weeks might be considered which always should be the case in prosthetic valve endocarditis.
Underlying Diseases
Urinary Tract Infection
Approximately half of the patients have predisposing factors, either systemic (particularly diabetes mellitus and cancer) or local (indwelling catheter and/or hyperplasia of the prostate) (5, 9).
Bacteremia/Septicemia
Most patients had predisposing diseases, predominantly urinary (prostatic hyperplasia and cancer) or cardiac (ischemic heart disease) (10, 21, 37).
Alternative Therapy
Urinary Tract Infection
For patients allergic to penicillin, nitrofurantoin or a Gram-positive active fluoroquinolone seem to be good alternatives, preceded by susceptibility testing.
Bacteremia/endocarditis
No information is available for non-penicillin treatment except data from time kill experiments. In severe cases, i.e. endocarditis, the time-kill experiments suggest a benefit of a combination with gentamicin. In the penicillin-allergic patient, vancomycin represents the most obvious alternative.
ADJUNCTIVE THERAPY
Removal of urinary catheters may be beneficial.
ENDPOINTS FOR MONITORING THERAPY
Objective clinical signs, paraclinical data, and negative cultures can be used to monitor therapy.
VACCINES
There is no vaccine available for protection against A. urinae.
PREVENTION OR INFECTION CONTROL MEASURES
General measures recommendable for prevention and control of urinary tract infections are appropriate.
![]()
REFERENCES
1. Aguirre M, Collins MD. Phylogenetic analysis of some Aerococcus-like organisms from urinary tract infections: description of Aerococcus urinae sp. nov. J Gen Microbiol 1992;138:401-5. [PubMed]
2. Astudillo L, Sailler L, Porte L, Lefevre JC, Massip P, Arlet-Suau E. Spondylodiscitis due to Aerococcus urinae: a first report. Scand J Infect Dis. 2003;35:890-1. [PubMed]
3. Christensen JJ, Gutschik E, Friis-Moller A, Korner B. Urosepticemia and fatal endocarditis caused by aerococcus-like organisms. Scand J Infect Dis 1991;23:717-21. [PubMed]
4. Christensen JJ, Jensen IP, Faerk J, Kristensen B, Skov R, Korner B. Bacteremia/septicemia due to Aerococcus-like organisms: report of seventeen cases. Danish ALO Study Group. Clin Infect Dis 1995;21:943-7. [PubMed]
5. Cattoir V, Kobal A, Legrand P. Aerococcus urinae and Aerococcus sanguinicola, two frequently misidentified uropathogens. Scand J Infect Dis. 2010 Oct;42(10):775-80. [PubMed]
6. Cattoir V, Kobal A, Legrand P. First Molecular Characterization of Fluoroquinolone Resistance in Aerococcus spp. Antimicrob Agents Chemother. 2010 Nov 15. [PubMed]
7. Christensen JJ, Dargis R, Hammer M, Justesen US,Nielsen XC, Kemp M, Danish MALDI-TOF MS Study Group. Matrix-assisted laser desorption ionizationtime of flight mass spectrometry analysis of Gram-positive, catalase-negative cocci not belonging to the Streptococcus or Enterococcus genus and benefits of database extension. J Clin Microbiol 2012;50:1787-1791. [PubMed]
8. Christensen JJ, Andresen K, Justesen T and Kemp M. Ribosomal DNA sequencing: Experiences from use in the Danish Reference Laboratory for Identification of bacteria. APMIS 113:621-628, 2005. [PubMed]
9. Christensen JJ, Gutschik E, Friis-Moller A, Korner B. Urosepticemia and fatal endocarditis caused by aerococcus-like organisms. Scand J Infect Dis 1991;23:717-21. [PubMed]
10. Christensen JJ, Jensen IP, Faerk J, Kristensen B, Skov R, Korner B. Bacteremia/septicemia due to Aerococcus-like organisms: report of seventeen cases. Danish ALO Study Group. Clin Infect Dis 1995;21:943-7. [PubMed]
11. Christensen JJ, Kilian M, Fussing V, Andresen K, Blom J, Korner B, Steigerwalt AG. Aerococcus urinae: polyphasic characterization of the species. APMIS 2005; 517-25. [PubMed]
12. Christensen JJ, Korner B. Aerococcus urinae: A newcommer in clinical and microbiological practice. Antimicrobics and Infectious Diseases Newsletter 1996;15:78-80. [PubMed]
13. Christensen JJ, Korner B, Casals JB, Pringler N. Aerococcus-like organisms: use of antibiograms for diagnostic and taxonomic purposes. J Antimicrob Chemother. 1996;38:253-8. [PubMed]
14. Christensen JJ, Korner B, Kjaergaard H. Aerococcus-like organism--an unnoticed urinary tract pathogen. APMIS 1989;97:539-46. [PubMed]
15. Christensen JJ, Vibits H, Ursing J, Korner B. Aerococcus-like organism, a newly recognized potential urinary tract pathogen. J Clin Microbiol 1991;29:1049-53. [PubMed]
16. Christensen JJ, Whitney AM, Teixeira LM, Steigerwalt AG, Facklam RR, Korner B, Brenner DJ. Aerococcus urinae: intraspecies genetic and phenotypic relatedness. Int J Syst Bacteriol 1997;47:28-32. [PubMed]
17. CLSI: Performance standards for antimicrobial susceptibility testin; Twenty-first informational Supplement. CLSI document M100-S21 Clinical and Laboratory Standards Institute, Wayne, Pennsylvania, USA
18. Colakoglu S, Turunc T, Taskoparan M, Aliskan H, Kizilkilic E, Demiroglu YZ, Arslan H. Three cases of serious infection caused by Aerococcus urinae: a patient with spontaneous bacterial peritonitis and two patients with bacteremia. Infection. 2008;36:288-90. [PubMed]
19.Delsarte M. Aerococcus in human infections: Review on a series of 29 hospital cases from 2001-2001. Thesis, Toulouse, France, April 2010.
20. de Jong MF, Soetekouw R, ten Kate RW, Veenendaal D. Aerococcus urinae: severe and fatal bloodstream infections and endocarditis. J Clin Microbiol. 2010;48:3445-7. [PubMed]
21. Ebnöther C, Altwegg M, Gottschalk J, Seebach JD, Kronenberg A. Aerococcus urinae Endocarditis: Case Report and Review of the Literature. Infection. 2002:30: 310-13. [PubMed]
22. EUCAST: www.EUCAST....http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_ files/Disk_test_documents/EUCAST_breakpoints_v1.2_101220.xls last accessed 02-01-2011.
23. Euzeby JP. List of Prokaryotic names with Standing in Nomenclature. http://www.bacterio.cict.fr/index.html. Attended december 2014.
24. Facklam R, Lovgren M, Shewmaker PL, and Tyrrell G. Phenotypic description and antimicrobial susceptibilities of Aerococcus sanguinicola isolates from human clinical samples. J Clin Microbiol 2003;41:2587-2592. [PubMed]
25. Goetz LL, Powell DJ, Castillo TA, Adkins L, Klausner AP, Gater DR. Hip abscess due to Aerococcus urinae in a man with paraplegia: case report. Spinal Cord. 2013;51:929-30. [PubMed]
26. Gritsch W, Nagl M, Hausdorfer J, Gschwendtner A, Pechlaner C, Wiedermann CJ. Septicaemia and endomyocarditis caused by Aerococcus urinae. Wien Klin Wochenschr 1999;111:446-7. [PubMed]
27. Grude N, Jenkins A, Tveten Y, Kristiansen BE. Identification of Aerococcus urinae in urine samples. Clin Microbiol Infect. 2003;9:976-9. [PubMed]
28. Grude N, Tveten Y. Aerococcus urinae og urinveisinfesjon. Tidsskr Nor Laegeforen 2002;122:174-5.
29. Guilarte YN, Tinguely R, Lupo A, Endimiani A. Prevalence and characteristics of fluoroquinolone-resistant Aerococcus urinae isolates detected in Switzerland. Int J Antimicrob Agents. 2014;43:474-5. [PubMed]
30. Heilesen AM. Septicaemia due to Aerococcus urinae. Scand J Infect Dis 1994;26:759-60.
31. Ho E, Coveliers J, Amsel BJ, Stockman B, Walpot J, Ieven M, Rodrigus I. A case of endocarditis due to Aerococcus urinae. J Heart Valve Dis. 2010;19:264-6. [PubMed]
32. Humphries RM, Hindler JA. In vitro antimicrobial susceptibility of Aerococcus urinae. J Clin Microbiol. 2014 ;52:2177-80. [PubMed]
33. Humphries RM, Lee C, Hindler JA. Aerococcus urinae and trimethoprim-sulfamethoxazole. J Clin Microbiol. 2011;49:3934-5. [PubMed]
34. Ibler K, Truberg Jensen K, Ostergaard C, Sönksen UW, Bruun B, Schønheyder HC, Kemp M, Dargis R, Andresen K, Christensen JJ. Six cases of Aerococcus sanguinicola infection: clinical relevance and bacterial identification. Scand J Infect Dis. 2008;40:761-5. [PubMed]
35. Imran M, Livesley P, Bell G, Pai P, Anijeet H.A Case Report of Successful Management of Aerococcus urinae Peritonitis in a Patient on Peritoneal Dialysis.Perit Dial Int. 2010;30:661-2. [PubMed]
36. Jones R, Master R, Powell D. Antimicrobial susceptibility testing of Aerococcus urinae. 38th Interscience Conference on Antimicrobial Agents and Chemotherapy, San Diego, 24 - 27 September 1998; P E58
37. Kass M, Toye B, Veinot JP. Fatal infective endocarditis due to Aerococcus urinae--case report and review of literature. Cardiovasc Pathol. 2008;17:410-2. [PubMed]
38. Kemp M, Bangsborg J, Kjerulf A, Andersen Schmidt T, Christensen J, Irmukhamedov A, Bruun NE, Dargis1 R, Andresen K, Christensen JJ. Advantages and Limitations of Ribosomal RNA PCR and DNA Sequenc-ing for Identification of Bacteria in Cardiac Valves of Danish Patients. Open Microbiol J 2013;7:146-151. [PubMed]
39. Kristensen B, Nielsen G. Endocarditis caused by Aerococcus urinae, a newly recognized pathogen. Eur J Clin Microbiol Infect Dis 1995;14:49-51. [PubMed]
40. Lawson PA, Falsen E, Truberg-Jensen K, Collins MD.Aerococcus sanguicola sp. nov., isolated from a human clinical source.Int J Syst Evol Microbiol. 2001;51(Pt 2):475-9. [PubMed]
41. Lenherr N, Berndt A, Ritz N, Rudin C. Aerococcus urinae: a possible reason for malodorous urine in otherwise healthy children. Eur J Pediatr. 2014;173:1115-7. [PubMed]
42. Ling Z, Kong J, Liu F, Zhu H, Chen X, Wang Y, Li L, Nelson KE, Xia Y, Xiang C. Molecular analysis of the diversity of vaginal microbiota associated with bacterial vaginosis. BMC Genomics.2010;11:488. [PubMed]
43. Lupo A, Guilarte YN, Droz S, Hirzel C, Furrer H, Endimiani A. In vitro activity of clinically implemented β-lactams against Aerococcus urinae: presence of non-susceptible isolates in Switzerland. New Microbiol. 2014;37:563-6. [PubMed]
44. Miyazato A, Ohkusu K, Tabata M, Uwabe K, Kawamura T, Tachi Y, Ezaki T, Niinami H, Mitsutake K. Comparative molecular and microbiological diagnosis of 19 infective endocarditis cases in which causative microbes were identified by PCR-based DNA sequencing from the excised heart valves. J Infect Chemother. 2012;18:318-23. [PubMed]
45. Murray TS, Muldrew KL, Finkelstein R, Hampton L, Edberg SC, Cappello M. Acute pyelonephritis caused by Aerococcus urinae in a 12-year-old boy. Pediatr Infect Dis J. 2008;27:760-2.[PubMed]
46. Naghibi M, Javaid MM, Holt SG. Case study: Aerococcus urinae as pathogen in peritoneal dialysis peritonitis--a first report. Perit Dial Int. 2007;27:715-6. [PubMed]
47. Nielsen XC, Carkaci D, Dargis R, Hannecke L, Justesen US, Kemp M, Hammer M, Christensen JJ. 16S-23S Intergenic Spacer (ITS) Region Sequence Analysis: Applicability and Usefulness in Identifying Genera and Species Resembling Non-Hemolytic Streptococci. Clin Microbiol 2013;2:6.
48. Perdekamp MG, Serr A, Hench J, Mattern D, Bohnert M. Hemopericardium caused by endocarditis ulcerosa: an unusual cause of sudden death in adolescence. Arch Kriminol. 2002;210:158-66. [PubMed]
49. Rasmussen M. Aerococci and aerococcal infections. J Infect. 2013:467-74. [PubMed]
50. Reinhard M, Prag J, Kemp M, Andresen K, Klemmensen B, Højlyng N, Sørensen SH, Christensen JJ. Ten cases of Actinobaculum schaalii infection: clinical relevance, bacterial identification, and antibiotic susceptibility. J Clin Microbiol. 2005;43:5305-8. [PubMed]
51. Ruoff KL. 2007. Aerococcus, Abiotrophia, and other aerobic catalase-negative, Gram-positive cocci. In: Murray PR, Baron EJ, Jorgensen JH, Landry ML, Pfaller MA.Manual of clinical microbiology 9th edition. Washington, D.C.: ASM Press p. 443-54. [PubMed]
52. Sandven P, Lassen J. Ringtest for bakteriologi 3/99. 1999. National Institute of Public Health, Norway.
53. Santos R, Santos E, Goncalves S, Marques A, Sequeira J, Abecasis P, Cadete M. Lymphadenitis caused by Aerococcus urinae infection. Scand J Infect Dis. 2003;35:353-4. [PubMed]
54. Schuur PM, Kasteren ME, Sabbe L, Vos MC, Janssens MM, Buiting AG. Urinary tract infections with Aerococcus urinae in the south of The Netherlands. Eur J Clin Microbiol Infect Dis 1997;16:871-5.[PubMed]
55. Schuur PM, Sabbe L, van der Wouw AJ, Montagne GJ, Buiting AG. Three Cases of Serious Infection Caused by Aerococcus urinae. Eur J Clin Microbiol Infect Dis 1999:18:368–371. [PubMed]
56. Senneby E, Petersson AC, Rasmussen M. Clinical and microbiological features of bacteraemia with Aerococcus Urinae. Clin Microbiol Infect 2012; 18: 546–550 . [PubMed]
57. Senneby E, Nilson B, Petersson AC, Rasmussen M. Matrix-assisted laser desorption ionization-time of flight mass spectrometry is a sensitive and specific method for identification of aerococci. J Clin Microbiol. 2013;51:1303-4. [PubMed]
58. Serefhanoglu K, Turan H, Dogan R, Gullu H, Arslan H. A case of Aerococcus urinae septicemia: an unusual presentation and severe disease course. Chin Med J (Engl). 2005;118:1318-20. [PubMed]
59. Shannon O, Mörgelin M, Rasmussen M. Platelet activation and biofilm formation by Aerococcus urinae, an endocarditis-causing pathogen. Infect Immun. 2010;78:4268-75. [PubMed]
60. Shelton-Dodge K, Vetter EA, Kohner PC, Nyre LM, Patel R. Clinical significance and antimicrobial susceptibilities of Aerococcus sanguinicola and Aerococcus urinae. Diagn Microbiol Infect Dis. 2011;70:448-51. [PubMed]
61. Sierra-Hoffman M, Watkins K, Jinadatha C, Fader R, Carpenter JL. Clinical significance of Aerococcus urinae: a retrospective review. Diagn Microbiol Infect Dis. 2005;53:289-92. [PubMed]
62. Skov R, Christensen JJ, Korner B, Frimodt-Moller N, Espersen F. In vitro antimicrobial susceptibility of Aerococcus urinae to 14 antibiotics, and time-kill curves for penicillin, gentamicin and vancomycin. J Antimicrob Chemother 2001;48:653-8. [PubMed]
63. Skov RL, Klarlund M, Thorsen S. Fatal endocarditis due to Aerococcus urinae. Diagn Microbiol Infect Dis 1995;21:219-21. [PubMed]
64. Slany M, Freiberger T, Pavlik P, Cerny J. Culture-negative infective endocarditis caused by Aerococcus urinae. J Heart Valve Dis. 2007;16:203-5.[PubMed]
65. Sturm PD, Van Eijk J, Veltman S, Meuleman E, Schülin T. Urosepsis with Actinobaculum schaalii and Aerococcus urinae. J Clin Microbiol. 2006;44:652-4.[PubMed]
66. Tekin A, Tekin G, Turunç T, Demiroğlu Z, Kizilkiliç O. Infective endocarditis and spondylodiscitis in a patient due to Aerococcus urinae: first report. Int J Cardiol. 2007 Feb 14;115(3):402-3. [PubMed]
67. Zbinden R, Santanam P, Hunziker L, Leuzinger B, von Graevenitz A. Endocarditis due to Aerococcus urinae: diagnostic tests, fatty acid composition and killing kinetics. Infection 1999;27:122-4.[PubMed]
68. Zhang Q, Kwoh C, Attorri S, Clarridge JE III. Aerococcus urinae in urinary tract infections. J Clin Microbiol 2000;38:1703-5. [PubMed]
![]()
Tables
Table 1. Phenotypic characteristics of Aerococcus species and other catalase-negative, Gram-positive, non-chain forming cocci, which have been isolated from humans.
| Hemolysis | Vancomycin susceptibility | 6.5% NaCl | Pyrrolidonyl aminopeptidase | Leucine aminopeptidase | Esculin hydrolysis | |
|---|---|---|---|---|---|---|
| A. urinae | α | S | + | - | + | -/(+) |
| A. sanguinicola | α | S | + | + | + | + |
| A. viridans | α | S | + | + | - | + |
| aA. christensenii | α | S | + | - | + | - |
| aA. urinaehominis | α | S | + | - | - | + |
| Dolosigranulum pigrum | n | S | + | + | + | + |
| Helcococcus kunzii | n | S | + | + | - | + |
| Pediococcus spp. | α | R | + | - | + | + |
| Gemella spp. | n/α | S | - | + | V | - |
| Alloiococcus otitidisb | n | S | + | + | + | - |
| Acid production from: | |||||
|---|---|---|---|---|---|
| sucrose | trehalose | mannitol | maltose | lactose | |
| A. urinae | + | - | + | - | - |
| A. sanguinicola | + | + | - | + | V |
| A. viridans | + | + | V | V | V |
| aA. christensenii | - | - | - | - | - |
| aA. urinaehominis | + | - | - | + | - |
| Dolosigranulum pigrum | - | - | - | - | - |
| Helcococcus kunzii | - | - | - | - | - |
| Pediococcus spp. | V | ||||
| Gemella spp. | + | ||||
| Alloiococcus otitidisb | - | ||||
Abbreviations: Hemolysis = hemolytic reaction on agar containing 5% sheep or horse blood; n = no hemolysis, V = variable.
a: data based on examination of one strain each (12)
b: Alloiococcus otitidis usually gives a weak positive reaction in the catalase test. Have been isolated from inner ear infections.
Table 2. Published data on minimal inhibitory concentrations (MICs) of antimicrobial agents for A. urinae and A. sanguinicolaa
| Antibiotic | A. urinae | A. sanguinicola | ||||
|---|---|---|---|---|---|---|
| (Breakpointsb: S;R in μg/ml) | ||||||
| Range in μg/ml | MIC50/MIC90 | No. of strains | Range | MIC50/MIC90 | No. of strains; (Reference) | |
| (Reference) | in μg/ml | |||||
| Penicillin G | ≤0.015-0.12 | 0.03/0.06 | n = 128 (32) | 0.03 | 0.03/0.03 | n = 15; (23) |
| (≤0.25; >2) | ≤0.004-0.25 | 0.016/0.064 | n = 80 (43) | |||
| 0.032-0.25 | 0.064/0.125 | n = 56; (61) | ||||
| <0.016/0.032 | n = 14 (56) | |||||
| 0.06 | 0.06/0.06 | n = 10; (13) | ||||
| Amoxicillin | ≤0.015-0.5 | 0.03/0.12 | n = 128 (32) | 0.03 | 0.03/0.03 | n = 15; (23) |
| (≤0.25; >2) | 0.016-0.5 | 0.032/0.064 | n = 80 (43) | 0.16-0.32 | 0.16/0.23 | n = 8; (5) |
| <0.032-0.25 | 0.064/0.125 | n = 56; (61) | ||||
| 0.08-0.32 | 0.23/0.32 | n = 20; (5) | ||||
| Piperacillin | 0.06-0.5 | 0.125/0.5 | n = 56; (61) | |||
| (≤0.25; >2) | ||||||
| Cefuroxim | 0.25-1 | 0.5/1 | n = 15; (23) | |||
| (≤0.5; >0.5) | ||||||
| Cefotaxim | ≤0.015-1 | 0.25/0.5 | n = 128 (32) | 0.06-0.25 | 0.12/0.25 | n = 15; (23) |
| (≤0.5; >0.5) | <0.016/0.125 | n = 14 (56) | ||||
| Ceftriaxone | ≤0.015-4 | 0.25/1 | n = 128 (32) | |||
| (≤0.5; >0.5) | ≤0.004-8 | 0.125/0.5 | n = 80 (43) | |||
| 0.125-32 | 8-Feb | n = 56; (61) | ||||
| Cefipime | 0.032-8 | 0.25/1 | n = 56; (61) | |||
| (≤0.5; >0.5) | ||||||
| Meropenem | ≤0.015-2 | 0.03/0.06 | n = 128 (32) | 0.06-2 | 0.06/1.0 | n = 15; (23) |
| (≤2; >2) | ||||||
| Gentamicin | 4-512 | 64/128 | n = 56; (61) | 24-Jun | 16/24 | n = 8; (5) |
| - | 1.5-48 | Apr-32 | n = 20; (5) | |||
| 16-Feb | n = 14 (56) | |||||
| Netilmicin | 4-256 | 32/64 | n = 56; (61) | |||
| - | ||||||
| Amikacin | 16-1024 | 256/512 | n = 56; (61) | |||
| - | ||||||
| Vancomycin | 0.12-1 | 0.5/0.5 | n = 128 (32) | 0.12-0.25 | 0.25/0.25 | n = 15; (23) |
| - | 0.064-1 | 0.38/0.5 | n = 80 (43) | 0.75-1 | 1-Jan | n = 8; (5) |
| 0.5-1 | 0.5/1 | n = 56; (61) | ||||
| 0.25/0.5 | n = 14 (56) | |||||
| 0.25-0.5 | 0.5/0.5 | n = 10; (13) | ||||
| 0.75-1.5 | 1-Jan | n = 20; (5) | ||||
| Teicoplanin | 0.19-1 | 0.5/0.75 | n = 20; (5) | 0.19-0.75 | 0.38/0.5 | n = 8; (5) |
| - | ||||||
| Rifampicin | 0.25 | 0.25/0.25 | n = 128 (32) | 2 | 2-Feb | n = 15; (23) |
| (≤0.06; >0.5) | <0.004-32 | 0.032/0.032 | n = 56; (61) | |||
| Erythromycin | 0.12->8 | 0.25/>8 | n = 128 (32) | 0.03-0.25 | 0.12/0.25 | n = 15; (23) |
| (≤0.25; >0.5) | 0.125-2 | 0.5/1 | n = 56; (61) | |||
| Clindamycin | 0.12-2 | 0.5/2 | n = 128 (32) | 0.03-0.5 | 0.25/0.5 | n = 15; (23) |
| (≤0.5; >0.5) | 0.125/0.5 | n = 14 (56) | ||||
| Tetracycline | 0.12->8 | 0.12/0.25 | n = 128 (32) | 2 | 2-Feb | n = 15; (22) |
| 4-Jan | 2-Feb | n = 56; (61) | ||||
| Ciprofloxacin | 0.125-4 | 2-Jan | n = 56; (61) | 4-Jan | 4-Jan | n = 15; (3) |
| - | 0.094->32 | 0.5/>32 | n = 20; (5) | 0.19->32 | 0.75/>32 | n = 8; (5) |
| 0.125/32 | n = 14 (56) | |||||
| Ofloxacin | 0.38->32 | 2/>32 | n = 20; (5) | 0.75->32 | 4/>32 | n = 8; (5) |
| - | ||||||
| Levofloxacin | 0.5->8 | 0.5/4 | n = 128 (32) | 0.5-16 | 16-Jan | n = 15; (23) |
| (≤1; >2) | 0.16-≥32 | 0.19/4 | n = 80 (29) | |||
| Trimetoprim | 16->128 | >128/>128 | n = 56; (61) | 0.25-4 | 2-Jan | n = 15; (23) |
| - | ||||||
| Co-trimoxazole | 0.25-8c | 0.5/1 | n = 128 (32) | 0.094-0.5 | 0.25/0.5 | n = 8; (5) |
| (≤1; >2) | ≤0.25-2.0c | 0.25/0.25 | n = 27 (33) | |||
| >4 | >4/>4 | n = 27 (33) | ||||
| >32 | >32/>32 | n = 20; (5) | ||||
| Fosfomycin | 4-128 | 8-Aug | n = 20; (5) | 48-128 | 64/128 | n = 8; (5) |
| - | ||||||
| Chloramphenicol | 4-Feb | 4-Feb | n = 15; (23) | |||
| (≤8; >8) | ||||||
| Quinopristin/ | 1 | 1-Jan | n = 15; (23) | |||
| Dalfopristin | ||||||
| - | ||||||
| Linezolid | 0.5-8 | 1/1 | n = 128 (32) | 2 | 2-Feb | n = 15; (23) |
| (≤2; >4) | ||||||
a: Only data from publications examining >2 strains are given.
b: Breakpoints as recommended for non-hemolytic streptococci by The European Committee on Antimicrobial Susceptibility Testing (EUCAST). A – denotes that no breakpoints are given for non-hemolytic streptococci.
c: Strains tested in cation-adjusted Mueller-Hinton (MH) broth (CAMHB) supplemented with 2.5% lysed horse blood (LHB). When examined on CAMHB plus lysed sheep blood (LSB) strains were non-susceptible.